
Abstract
Background
Arm span length is related to standing height and has been studied as a substitute for current standing height for predicting lung function parameters. However, it has never been studied in elderly COPD patients.
Purpose
To evaluate the accuracy of substituting arm span length for current standing height in the evaluation of pulmonary function parameters and severity classification in elderly Thai COPD patients.
Materials and methods: Current standing height and arm span length were measured in COPD patients aged >60 years. Postbronchodilator spirometric parameters, forced vital capacity (FVC), forced expiratory volume in first second (FEV1), and ratio of FEV1/FVC (FEV1%), were used to classify disease severity according to global initiative for chronic obstructive lung disease criteria. Predicted values for each parameter were also calculated separately utilizing current standing height or arm span length measurements. Student’s t-tests and chi-squared tests were used to compare differences between the groups. Statistical significance was set at P<0.05.
Results
A total of 106 COPD patients with a mean age of 72.1±7.8 years, mean body mass index of 20.6±3.8 kg/m2, and mean standing height of 156.4±8.3 cm were enrolled. The mean arm span length exceeded mean standing height by 7.7±4.6 cm (164.0±9.0 vs 156.4±8.3 cm, P<0.001), at a ratio of 1.05±0.03. Percentages of both predicted FVC and FEV1 values based on arm span length were significantly lower than those using current standing height (76.6±25.4 vs 61.6±16.8, P<0.001 and 50.8±25.4 vs 41.1±15.3, P<0.001). Disease severity increased in 39.6% (42/106) of subjects using arm span length over current standing height for predicted lung function.
Conclusion
Direct substitution of arm span length for current standing height in elderly Thai COPD patients should not be recommended in cases where arm span length exceeds standing height by more than 4 cm.
Introduction
Pulmonary function tests use standardized reference values based on ethnic and anthropometric characteristics, including age, sex, and height.Citation1 It has become increasingly necessary to measure pulmonary function in patients who are unable to stand, as their current standing height cannot be accurately measured.Citation2,Citation3 The American Thoracic Society (ATS) and the European Respiratory Society (ERS) jointly recommend other options, including stated height or estimating from arm span when height cannot be measured.Citation4
Substitution of standing height measurements can be estimated from arm span measurements using the appropriate regression equations and might be an alternative method to use for subjects in whom current standing height cannot be measured (eg, subjects with skeletal deformities or standing inability).Citation5,Citation6 Substitution of arm span for standing height is important for assessment of predicted value of lung volume in elderly people with osteoporosis.Citation7 One study suggested that standing height estimated using arm span could be directly substituted for actual height in adults for whom height could not be measured reliably.Citation8 Other studies also suggested that arm span could be used for predicting lung function instead of height for elderly womenCitation9,Citation10 and that FEV1 values using height and arm span were not statistically different in elderly individuals.Citation11,Citation12
However, estimating height from arm span is controversial because the relationship between height and arm span varies with age and ethnicity.Citation13–Citation15 Although estimated height from arm span is highly correlated with standing height in general populations, there is very poor agreement with standing height in acutely ill elderly populations.Citation16 A longitudinal study showed that actual standing height is lost from age 30 to 80 years,Citation17 but arm span is still closely correlated to maximal standing height.Citation18 Elderly COPD patients may lose their standing height more rapidly than normal aging populations due to direct effects of the disease like osteoporosis, irrespective of corticosteroid use, age, and sex.Citation19–Citation21 Therefore, substituting arm span measurement for actual height in estimating pulmonary function parameters should be investigated in COPD patients with advanced age. This study aimed to evaluate the use of arm span length as an alternative measure for the estimation of height and in the prediction of spirometry in elderly Thai COPD patients.
Materials and methods
Participants and study design
We conducted a cross-sectional study enrolling Thai COPD patients who were more than 60 years of age and who were managed by pulmonologists at the chest clinic of Chiang Mai University Hospital, Chiang Mai, Thailand, between October 1, 2012 and September 30, 2013. Patients who were unable to stand, or had structural or neuromuscular defects, as well as subjects with chest or upper limb deformities were excluded. Accurate measurements of both standing height and arm span length in the same subjects were performed after the enrollment. Standing height was measured on barefooted subjects using a wall-mounted stadiometer (Zepper ZT160, China) while the subject was standing as tall as possible with buttocks, back, and head against the wall and looking straight ahead. Arm span was measured from tip-to-tip of middle fingers with hands maximally outstretched while standing against a wall, using a flexible calibrated steel tape measure (Butterfly brand tape measure, China). Both measurements were taken to the nearest centimeter, and the mean values recorded. Arm span: standing height ratios were calculated separately for all subjects. All subjects underwent spirometric evaluation using a spirometer (Vmax series 22, Sensor Medics, Bilthoven, Holland). Postbronchodilator (400 µg of salbutamol), forced vital capacity (FVC), forced expiratory volume in first second (FEV1), and ratio of FEV1/FVC were measured for all subjects using ATS/ERS standard guidelines.Citation1 Values were calculated using National Health and Nutrition Examination Survey (NHANES) III reference equations.Citation22 However, for Asians, a correction factor of 0.88 was applied to predicted FVC and FEV1.Citation23 COPD was classified according to global initiative for chronic obstructive lung disease (GOLD) severity classificationCitation24 using both current standing height and arm span length measurements for each subject. We considered results clinically significant if the percentage of predicted FEV1 based on arm span differed by 5% or more from standing height calculations.Citation20 The study protocol was approved by the Institutional Ethics Committee of the Faculty of Medicine, Chiang Mai University.
Sample size calculation
A standard deviation (SD) of 22 cm between arm span length and standing height in patients was previously estimated as significant.Citation2 In the same study, the maximum acceptable difference between standing height and arm span length was set at 8 cm. Our sample size calculation was based on the 95% confidence interval (CI), thus, keeping the type I error rate at 0.05 and probability (power) at 0.95. A total of 100 patients was the minimum required sample size considered necessary to provide valid results.
Statistical analysis
Results for numerical values are expressed as mean ± SD, and those for categorical data are expressed as absolute frequencies and percentages. Categorical variables were analyzed using chi-square tests, whereas continuous variables were compared using Student’s t-tests. Statistical significance was set at P<0.05. All analyses were carried out using the SPSS statistical package, version 16 for Windows (SPSS, Inc, Chicago, IL, USA).
Results
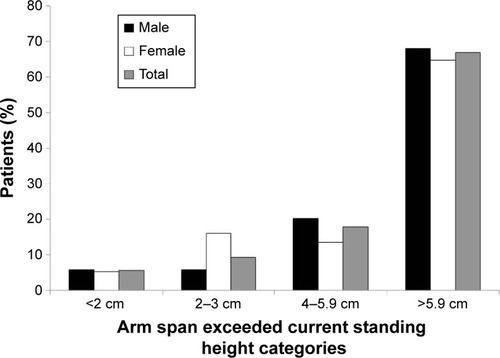
The baseline characteristics of all 106 enrolled COPD patients according to sex are shown in . Mean age of subjects was 72.1±7.8 years, with a mean body mass index of 20.6±3.8 kg/m2, and a mean standing height of 156.4±8.3 cm. Mean standing height and arm span lengths were 156.4±8.3 and 164.0±8.3 cm, respectively. Mean ratio of arm span length to current standing height was 1.05±0.03. Arm span length exceeded current standing height by a mean length of 7.7±4.6 cm. Mean percentage of predicted FEV1 was 50.8±25.4 and mean ratio of FEV1 to FVC was 51.8±11.0 based on current standing heights. Arm span measurements exceeded current standing height in 101 (95.3%) patients, without significant difference between sexes (), and was categorized into four groups: <2.0, 2.0–3.9, 4.0–5.9, and >5.9 cm comprising 6 (5.7%), 10 (9.4%), 19 (17.9%), and 71 (67.0%) patients, respectively ().
Table 1 Baseline characteristics according to sex and all patients
Table 2 Comparison of standing height and arm span length (n=106)
Figure 1 Percentage of patients whose arm span length exceeded standing height according to sex and all patients.
shows spirometric data and GOLD classification based on current standing height and arm span length. Both percentage of predicted FVC and percentage of FEV1 were significantly lower when based on arm span length compared to current standing height in both sexes. The variation between GOLD classification based on current standing height compared to arm span length was statistically significant (P<0.001). Disease severity based on GOLD stage classification was 39.6% (42/106) higher when standing height was used compared to arm span length, especially in males (52.2% vs 16.2% in females, P<0.001) (). When using arm span length, 41 cases (97.6%) were one GOLD classification lower, and 1 case (2.4%) was two GOLD classifications lower. In all, 69 subjects out of 90 had arm span lengths exceeding their respective standing heights by at least 4 cm, resulting in decreased predicted FEV1 values $5%, without significant differences between sexes ().
Table 3 Spirometric data and GOLD classification based on standing height and arm span length
Table 4 GOLD classification changes based on substituting arm span length for standing height
Table 5 The proportion of COPD subjects within each arm span exceed height category where the difference in percent predicted FEV1 exceed 5% point
Discussion
Our study aimed to evaluate the use of arm span length as an alternative to standing height in the prediction of spirometry in elderly Thai COPD patients. The results revealed that the percentages of predicted FVC and FEV1 based on arm span length were significantly lower than current standing height in elderly Thai COPD patients. Both measures of percentages of predicted FVC and FEV1 were significantly underestimated when using arm span length compared to standing height (mean percent difference: 15.1±13.5 and 9.7±9.9, respectively). A clinical underestimation of at least 5% of the predicted FEV1 values was revealed in all subjects whose arm span length exceeded standing heights of at least 4 cm. Underestimation of percentages of predicted FVC and FEV1 based on arm span length in this study resulted in significant reclassification (~40%) into a higher GOLD severity category. Treatment implications are different for patients classified into incorrect GOLD cateogies.Citation24 Because the absolute mean difference between height and arm span in any individual is usually small (mean: 3.4–4.7 cm) in previous studies, arm span was proposed as a direct substitution for height in prediction equations.Citation8–Citation10 Since this phenomenon is more marked in our elderly COPD patients, with an absolute mean difference between height and arm span almost twice higher (7.7 cm), a direct substitution of arm span length to current standing height incurred a significant underestimation of lung function and led to an almost 40% increase in GOLD severity classification. This should be considered as an incorrect interpretation of pulmonary function tests, misclassification of GOLD severity, and erroneous change in treatment regimen in elderly Thai COPD patients.
Our study should, therefore, draw attention to the potential discordance of arm span and height measurements in spirometric assessments of elderly COPD patients. Such a discrepancy may be related to ethnicity or may be due to extraordinary loss of current standing height as a result of COPD-related osteoporosis rather than the normal physiologic aging process.Citation9,Citation10 A previous longitudinal study suggests that current measured height may underestimate the progression of COPD, and that the use of arm span to determine height will give a more accurate measure of COPD progression.Citation25 We disagree with this suggestion because arm span length significantly differed from current standing height in our study. Current standing height is one of the standard variables for pulmonary function measurement; therefore, we may not be able to reliably replace standing height with arm span. The potential clinical significance of the discrepancy between arm span and standing height, including underestimation of disease severity, should be taken into consideration. Once a method is chosen to estimate height, parameters required for arm span length or current standing height should be considered. When surrogate measures of height for elderly COPD patients are used in a clinical setting, data collection should not be mixed with the methods of height estimation.
Further investigation is needed for patients with osteoporosis, as they were not investigated in our study. Our study was limited because no height estimation regression equation using arm span length is available for Thai populations and because the study was conducted with a limited sample size of elderly COPD patients.
We suggest that until a regression equation correlating arm span length to standing height for Thai patients is developed, arm span length cannot be substituted for standing height when evaluating elderly Thai COPD patients.
Conclusion
Direct substitution of arm span length for current standing height in elderly Thai COPD patients cannot be recommended in cases where arm span length exceeds standing height by more than 4 cm.
Author contributions
The first author, Chaicharn Pothirat, developed the study design and carried out acquisition and interpretation of data, statistical analysis, manuscript preparation, and critical revision of intellectual contents. The remaining authors contributed to acquisition and interpretation of data, revised the article for important intellectual content, and gave final approval of the version to be published.
Acknowledgments
The authors wish to thank the subjects who kindly took part in this study and acknowledge the staff members of the Division of Pulmonary, Critical Care and Allergy, Department of Internal Medicine, Faculty of Medicine, Chiang Mai University for their contribution to this study.
Disclosure
The authors report no conflicts of interest in this work.
References
- MillerMRHankinsonJBrusascoVStandardisation of spirometryEur Respir J200526231933816055882
- Sancho-ChustJNChinerECamarasaASenentCDifferences in pulmonary function based on height prediction obtained by using alternative measuresRespiration201079646146819713690
- Garcia-RioFPinoJMDorghamAAlonsoAVillamorJSpirometric reference equations for European females and males aged 65–85 yearsEur Respir J200424339740515358698
- PellegrinoRViegiGBrusascoVInterpretative strategies for lung function testsEur Respir J200526594896816264058
- CapderouABerkaniMBecqueminM-HZelterMReconsidering the arm span–height relationship in patients referred for spirometryEur Respir J201137115716320530045
- GolshanMAmraBHoghoghiMAIs arm span an accurate measure of height to predict pulmonary function parameters?Monaldi Arch Chest Dis200359318919215065313
- TeramotoSMatsuseTOuchiYSubstitution of arm span for standing height is important for the assessment of predicted value of lung volumes in elderly people with osteoporosisChest199911661837183810593822
- AggarwalANGuptaDJindalSKInterpreting spirometric data: impact of substitution of arm span for standing height in adults from North IndiaChest1999115255756210027459
- LeechJADulbergCKellieSPatteeLGayJRelationship of lung function to severity of osteoporosis in womenAm Rev Respir Dis1990141168712297189
- AllenSCThe relation between height, arm span and forced expiratory volume in elderly womenAge Ageing19891821131162729005
- KwokTWhitelawMNThe use of arm span in nutritional assessment of the elderlyJ Am Geriatr Soc19913954924962022801
- ChhabraSKUsing arm span to derive height: impact of three estimates of height on interpretation of spirometryAnn Thorac Med200833949919561887
- ParkerJMDillardTAPhillipsYYArm span-height relationships in patients referred for spirometryAm J Respir Crit Care Med19961542 Pt 15335368756834
- HibbertMELaniganARavenJPhelanPDRelation of arm span to height and the prediction of lung functionThorax19884386576593175981
- ReevesSLVarakaminCHenryCJThe relationship between arm-span measurement and height with special reference to gender and ethnicityEur J Clin Nutr19965063984008793422
- HicksonMFrostGA comparison of three methods for estimating height in the acutely ill elderly populationJ Hum Nutr Diet2003161132012581405
- SorkinJDMullerDCAndresRLongitudinal change in height of men and women: implications for interpretation of the body mass index: the Baltimore Longitudinal Study of AgingAm J Epidemiol1999150996997710547143
- HarrisJAJacksonCMPatersonDGScammonREThe Measurement of ManMinneapolis, MNUniversity of Minnesota Press1930
- FergusonGTCalverleyPMAndersonJAPrevalence and progression of osteoporosis in patients with COPD: results from the TOwards a Revolution in COPD Health studyChest200913661456146519581353
- KjensliARygMFalchJADoes body height reduction influence interpretation of lung function in COPD patients?Eur Respir J201036354054820110396
- Graat-VerboomLWoutersEFSmeenkFWvan den BorneBELundeRSpruitMACurrent status of research on osteoporosis in COPD: a systematic reviewEur Respir J200934120921819567604
- HankinsonJLOdencrantzJRFedanKBSpirometric reference values from asample of the general US populationAm J Respir Crit Care Med199915911791879872837
- HankinsonJLKawutSMShaharESmithLJStukovskyKHBarrRGPerformance of American Thoracic Society-recommended spirometry reference values in a multiethnic sample of adults: the multi-ethnic study of atherosclerosis (MESA) lung studyChest2010137113814519741060
- RabeKFHurdSAnzuetoAGlobal strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summaryAm J Respir Crit Care Med2007176653255517507545
- AnsariKKeaneyNPriceMPrecision in diagnosing and classifying COPD: comparison of historical height with current height and arm span to predict FEV1Open Respir Med J20126545822896775