
Abstract
Background
Data regarding osteoporosis in COPD patients in Taiwan remain limited. The primary end point of this study was to evaluate the prevalence and risk factors of osteoporosis in COPD patients in Taiwan. The secondary end point was to examine the association between osteoporosis and health-related quality of life (HRQL) in COPD patients.
Materials and methods
This prospective cross-sectional study enrolled 125 COPD patients (mean age 73.6 years, forced expiratory volume in 1 second [FEV1] 1.19±0.43 L) who had bone mineral-density measurements performed consecutively. Demographic data, lung function, and HRQL including modified Medical Research Council dyspnea scale, St George’s Respiratory Questionnaire, oxygen-cost diagram, Center for Epidemiologic Studies – depression scale, and COPD Assessment Test scores were recorded.
Results
A total of 50 (40%) participants were diagnosed as having osteoporosis. In a multivariate logistic regression model including age, smoking amount (pack-year), body mass index (BMI), and FEV1, only BMI (odds ratio 0.824, 95% confidence interval 0.73–0.93; P=0.002) and FEV1 (odds ratio 0.360, 95% confidence interval 0.13–0.98; P=0.046) were negatively associated with an increased risk of osteoporosis in COPD patients. In addition, COPD patients with osteoporosis had significantly higher modified Medical Research Council dyspnea scale scores (1.7±0.8 vs 1.4±0.8, P=0.046), St George’s Respiratory Questionnaire scores (36.6 vs 28.0, P=0.01), and COPD Assessment Test scores (14.7±8 vs 11.5±7, P=0.019), and lower oxygen-cost diagram score (4.8±1.8 vs 5.4±1.6, P=0.045) than patients without osteoporosis.
Conclusion
The prevalence of osteoporosis in COPD patients was high at a community hospital in Taiwan. BMI and FEV1 were the independent risk factors for osteoporosis in COPD. In addition, COPD patients with osteoporosis had worse HRQL than those without osteoporosis.
Introduction
COPD is characterized by persistent airflow limitation caused by an enhanced chronic inflammatory response in the airways and the lungs.Citation1–Citation3 It is not only a pulmonary disease but is also being recognized a systemic disease with widespread comorbidities, such as cardiovascular diseases, psychological disorders, and osteoporosis.Citation4–Citation6 COPD is the fourth-leading cause of death in the world, and the economic burden related to this disease is projected to increase in coming decades because of continued exposure to COPD risk factors and aging of the general population.Citation7,Citation8
Osteoporosis has been recognized as a major comorbidity in COPD, but it is often underdiagnosed and associated with poor health status and prognosis.Citation9 The etiology of osteoporosis in COPD is complex, and various risk factors may contribute to its pathogenesis, such as older age, tobacco smoking,Citation10 systemic inflammation, vitamin D deficiency, and the use of oral or inhaled corticosteroids (ICS).Citation11 The reported prevalence of osteoporosis in COPD patients ranges widely from 23% to ~50% as diagnosed by bone mineral density (BMD), and from 24% to ~80% as diagnosed by BMD or vertebral compression fracture.Citation10,Citation12–Citation20 However, there are currently no studies regarding the prevalence and risk factors of osteoporosis in patients with COPD in Taiwan. In addition, few studies have reported an association between health-related quality of life (HRQL) and osteoporosis in patients with COPD.Citation21
The primary end point of this study was to investigate the prevalence and risk factors of osteoporosis in COPD among Taiwanese patients. The secondary end point was to examine the association between HRQL and osteoporosis in patients with COPD.
Materials and methods
Study setting
In this cross-sectional study, we examined the data (collected from March 2011 to December 2012) of participants enrolled in the CMPICO study.Citation22 In brief, part of the CMPICO study was designed to investigate relevant comorbidities in patients with COPD, such as osteoporosis, cardiovascular diseases, and psychological diseases. The study was carried out at the outpatient department of the Division of Pulmonary and Critical Care Medicine, Ditmanson Medical Foundation, Chia-Yi Christian Hospital, which is a 1,000-bed community-based teaching hospital in Chiayi, Taiwan. The Institutional Review Board of Ditmanson Medical Foundation approved this study (100001), and also approved the consent procedure outlined as follows. The majority of the enrolled individuals provided written informed consent; however, there were a few illiterate subjects enrolled. Our team explained the study design thoroughly to all of these illiterate subjects, and if they agreed to participate, they signed consent forms using fingerprints in lieu of a written signature. A total of 189 COPD patients at outpatient departments were recruited in the CMPICO study during the period, and 125 (66%) patients were willing to undergo BMD examination and X-ray survey.
Subjects
A total of 125 COPD patients who had undergone measurement for BMD and spinal X-rays were enrolled in the current study. The diagnosis of COPD was based on the GOLD (Global Initiative for Chronic Obstructive Lung Disease) guidelines.Citation23 Eligible patients were 47–90 years of age with a postbronchodilator forced expiratory volume in 1 second (FEV1) to forced vital capacity (FVC) ratio of less than 0.7.Citation19 Patients with a history of bronchial asthma and other structural lung diseases (such as lung cancer, bronchiectasis, and fibrotic lung) were excluded. A chest physician carefully reviewed the chest radiographs of all the patients. A total of 125 patients (98% male) with a mean age of 73.6±7.69 years met the inclusion criteria and were enrolled.
Diagnosis of osteoporosis
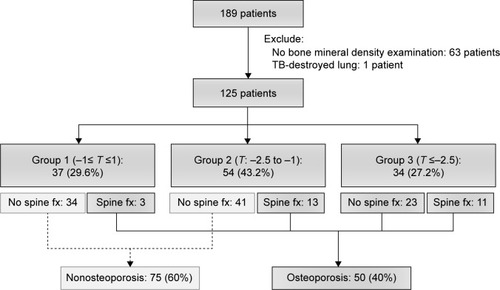
BMD was measured by performing a dual-energy X-ray absorptiometry scan of the lumbar spine and bilateral femoral neck. Bone with artificial implantation was excluded in this study. T-scores were calculated based on the results of BMD, as described by Brunader and Shelton.Citation24 Osteoporosis is defined as a systemic skeletal disease characterized by low-bone density and microarchitectural deterioration of bone tissue, with a consequent increase in bone fragility.Citation25 Notably, vertebral fracture has been demonstrated to have a strong relationship with microarchitectural deterioration.Citation26 Vertebral fracture was evaluated from a lateral chest X-ray and lumbosacral spine X-ray by an orthopedic surgeon. Fracture was defined as >20% reduction in anterior, middle, or posterior height using the semiquantitative method, as described by Genant et al.Citation27 As a result, patients with low BMD (T-score ≤−2.5) or vertebral fracture were diagnosed as having osteoporosis in our study. Otherwise, patients with a T-score >−2.5 and no vertebral fracture were classified into the nonosteoporosis group ().
Figure 1 Algorithm of the study.
Health-related quality of life and depression
Questionnaire tools included the modified Medical Research Council (mMRC) dyspnea scale,Citation28 St George’s Respiratory Questionnaire (SGRQ),Citation29 COPD Assessment Test (CAT),Citation30 oxygen-cost diagram (OCD),Citation31 and Center for Epidemiologic Studies – depression (CES-D) scale,Citation32 and scores were obtained to evaluate each patient’s life quality and the severity of depression.
Data collection
Interviews were conducted by a trained staff member in charge of COPD case management who used a well-established questionnaire to collect demographic information of the study participants, including date of birth, sex, smoking status, and personal medical history. Body weight, height, and blood pressure were measured for each participant. Body mass index (BMI) was calculated as weight (kilograms) divided by the square of the height (meters). The subjects self-reported their medical history, including hypertension, hyperlipidemia, and diabetes mellitus, for which the diagnostic definitions are detailed in our previous study.Citation22 Smoking status was also evaluated by a self-reported questionnaire.
Statistical analysis
Data were analyzed by SPSS statistical software for Windows version 22 (IBM Corporation, Armonk, NY, USA). Relationships between two continuous parameters were evaluated by independent Student’s t-test. Relationships between two discrete parameters were evaluated by cross-table χ2 test. Continuous data are expressed as means ± standard deviation. Variables with significant difference between the osteoporosis and nonosteoporosis groups were analyzed using a multivariate logistic regression model.
Results
Of the 125 participants, 50 (40%) were diagnosed as having osteoporosis. The most common comorbidity observed was hypertension (n=63, 50.4%), followed by diabetes mellitus (n=16, 12.8%), and hyperlipidemia (n=13, 10.4%). A total of 118 (94.4%) had a history of smoking (at least 10 pack-years), including current (n=53, 42.4%) and former (n=65, 52%) smokers. Mean pack-years of smoking was 47.22.
As shown in , there were no significant differences in clinical characteristics between the COPD patients with and without osteoporosis with the exception of BMI, which showed that COPD patients with osteoporosis had a lower BMI than patients without osteoporosis (21.75±3.4 vs 23.93±3.3, P=0.001). Certainly, COPD patients with osteoporosis had lower values with regard to the parameters of lumbar spine, left femoral neck, right femoral neck, and T-score in terms of BMD than COPD patients without osteoporosis.
Table 1 Clinical characteristics of COPD patient with and without osteoporosis
Severity of COPD had been classified in stages (I–IV) previously and groups (A–D) currently according to the GOLD guidelines. Comparing the GOLD stages (I–IV) between the COPD patients with and without osteoporosis, there was no significant difference between the two groups. However, if patients were classified by current GOLD groups (A–D), there was a significant difference between the two groups (P=0.024, ). However, COPD patients with osteoporosis had significantly lower FEV1 (1.07±0.37 vs 1.28±0.45 L, P=0.007), and FEV1/FVC (52.79±11.0 vs 58.43±8.9, P=0.002) than those without osteoporosis.
Table 2 GOLD stage and pulmonary function in COPD patients with and without osteoporosis
Using a multivariate logistic regression model that included age, smoking amount (pack-year), BMI, and FEV1, only BMI (odds ratio [OR] 0.824, 95% confidence interval 0.73–0.93; P=0.002) and FEV1 (OR 0.360, 95% confidence interval 0.13–0.98; P=0.046) were significantly associated with an increased risk of osteoporosis in COPD patients ().
Table 3 Multivariate logistic regression analysis of factors for osteoporosis in COPD patients
To evaluate the HRQL in all enrolled patients, various questionnaires were obtained and analyzed (). COPD patients with osteoporosis had significantly higher mMRC scores (1.7±0.8 vs 1.4±0.8, P=0.046), higher SGRQ scores (36.6 vs 28.0, P=0.01), lower OCD scores (4.8±1.8 vs 5.4±1.6, P=0.045), and higher CAT scores (14.7±8 vs 11.5±7, P=0.019) than patients without osteoporosis. However, there was no significant difference in CES-D scores between the two groups.
Table 4 Health-related quality of life in COPD patients with and without osteoporosis
Discussion
To the best of our knowledge, this is the first study to highlight the prevalence and risk factors of osteoporosis in patients with COPD at a community hospital in Taiwan. Our study showed that the prevalence of osteoporosis was 40% in patients with COPD. COPD patients with osteoporosis had lower BMI, FEV1, and FEV1/FVC than COPD patients without osteoporosis. In a multivariate logistic regression model, only BMI and FEV1 were significantly associated with an increased risk of osteoporosis in COPD patients. When comparing the HRQL between the two groups, COPD patients with osteoporosis had significantly higher mMRC scores, SGRQ scores, CAT scores, and lower OCD scores than those without osteoporosis, indicating that osteoporosis patients had worse quality of life and exercise performance.
Osteoporosis has been recognized as an emerging issue in the care of COPD, since osteoporosis would increase the difficulty and complexity in the management of COPD. It has also been identified as most at risk for the experiencing of severe exacerbations requiring hospitalization.Citation33 As shown in , there have been a number of studies investigating the prevalence and related risk factors worldwide over the past decade.Citation12,Citation15,Citation17–Citation20 Based on different definitions, the prevalence of osteoporosis ranges from 23% to 42% diagnosed only by BMD and from 47% to 83.7% diagnosed by both BMD and vertebral compression fracture.Citation12,Citation17–Citation20 The wide range with regard to osteoporosis-prevalence rates in the world may be in part be related to the methodological differences of osteoporosis diagnosis and the enrollment criteria of patient populations, such as age and severity of COPD.
Table 5 Prevalence and related risk factors of osteoporosis in COPD patients for the past decade worldwide
Malnutrition, indicated by lower BMI, is a possible cause of bone loss and fractures, frequently associated with inflammation and hormonal change.Citation34 Several studies have confirmed that BMI is positively associated with BMD in a variety of patient populations.Citation35–Citation38 Not surprisingly, this is consistent in patients with COPD based on previous studiesCitation12,Citation13,Citation15,Citation16,Citation19 and also as seen in our findings, which all showed that BMI was an independent risk factor for osteoporosis.
Similarly to previous reports,Citation12,Citation13,Citation15,Citation16,Citation19 our data showed that pulmonary function, like FEV1 or FVC, was the independent risk factor for osteoporosis. A South Korean study that enrolled 456 premenopausal women who had never smoked showed that FVC and FEV1 were correlated with BMD.Citation39 This is consistent with our findings showing that FEV1 is an independent risk factor regardless of smoking history.
The related literature has been inconsistent as to whether oral steroid use is a risk factor for osteoporosis in COPD.Citation13,Citation15,Citation17,Citation40 The TORCH study demonstrated that ICS use was not associated with BMD.Citation18 Other studies likewise have shown that oral steroid use was not correlated with osteoporosis in patients with COPD.Citation15,Citation17 On the contrary, ICS use was associated with a modest but statistically significant increase (>20%) in the risk of fractures in patients with COPD from a meta-analysis of randomized controlled trials (16 trials) and observational studies (seven trials).Citation41 Another large case–control study showed that current use of high-dose ICS (more than 700 μg/day) was associated with an increased risk of nonvertebral fractures compared with patients with no ICS exposure (adjusted OR 1.68). Therefore, the impact of ICS should be further verified by studies in the future.
A study reported on an association between HRQL and osteoporosis in patients with COPD.Citation21 This study showed that HRQL, which was assessed by mMRC scale, SGRQ, and CAT scores, was significantly worse in patients with osteoporosis than those without osteoporosis. The mMRC scale is based on the patient’s perception of dyspnea in daily activities,Citation28 and is a practical tool to assess the HRQL of patients with COPD.Citation42 Notably, current GOLD guidelines combine a dyspnea scale (mMRC or CAT) and pulmonary function to classify the severity of COPD, which is compatible with our finding that the proportion of osteoporosis was more correlated with group classification than stage classification (pulmonary function alone). This study showed that osteoporosis was associated with higher mMRC dyspnea scores in patients with COPD, which is similar with results from previous studies.Citation43,Citation44 There is a paucity of data regarding the association between SGRQ and osteoporosis. To the best of our knowledge, this is the first study revealing that COPD patients with osteoporosis had higher SGRQ scores than those without osteoporosis. The CES-D scale is a short self-reporting scale designed to measure depressive symptomatology in the general population. This study showed that depression was not associated with osteoporosis in patients with COPD.
This study has a number of limitations that are worth noting. First, the sample size was small, and the majority of patients were male. A previous study has shown that the ratio of male to female smoking rates was 10.9 to 1 among adults in Taiwan.Citation9 Since smoking is the major risk factor for COPD, it is reasonable that COPD patients are predominantly male in Taiwan. However, large studies are needed to verify our results. Second, information regarding possible risk factors like vitamin D deficiency and oral steroid use was unavailable during our study. However, most previous studies showed that oral steroids were not associated with increased risk of osteoporosis in patients with COPD.
In conclusion, the prevalence of osteoporosis in COPD patients was high in Taiwan. BMI and FEV1 were the independent risk factors for osteoporosis in COPD. Therefore, measuring BMD in COPD patients with lower BMI or pulmonary function should be recommended. As a result, further study may be required to investigate whether the prevention of osteoporosis utilizing such strategies as increasing body weight, encouraging smoke cessation, and/or prescribing medications that can help prevent osteoporosis would improve the quality of life in patients with COPD.
Disclosure
The authors report no conflicts of interest in this work.
References
- HoggJCChuFUtokaparchSThe nature of small-airway obstruction in chronic obstructive pulmonary diseaseN Engl J Med2004350262645265315215480
- TamimiASerdarevicDHananiaNAThe effects of cigarette smoke on airway inflammation in asthma and COPD: therapeutic implicationsRespir Med2012106331932822196881
- Garcia-RioFMiravitllesMSorianoJBSystemic inflammation in chronic obstructive pulmonary disease: a population-based studyRespir Res2010116320500811
- FabbriLMLuppiFBeghéBRabeKFComplex chronic comorbidities of COPDEur Respir J200831120421218166598
- SorianoJBVisickGTMuellerovaHPayvandiNHansellALPatterns of comorbidities in newly diagnosed COPD and asthma in primary careChest200512842099210716236861
- DecramerMJanssensWMiravitllesMChronic obstructive pulmonary diseaseLancet201237998231341135122314182
- FletcherMJUptonJTaylor-FishwickJCOPD uncovered: an international survey on the impact of chronic obstructive pulmonary disease [COPD] on a working age populationBMC Public Health20111161221806798
- ManninoDMKirizVAChanging the burden of COPD mortalityInt J Chron Obstruct Pulmon Dis20061321923318046859
- WenCPLevyDTChengTYHsuCCTsaiSPSmoking behaviour in Taiwan, 2001Tob Control200514Suppl 1i51i5515923450
- VriezeAde GreefMHWijkstraPJWempeJBLow bone mineral density in COPD patients related to worse lung function, low weight and decreased fat-free massOsteoporos Int20071891197120217347789
- RommeEASmeenkFWRuttenEPWoutersEFOsteoporosis in chronic obstructive pulmonary diseaseExpert Rev Respir Med20137439741023952337
- WatanabeRTanakaTAitaKOsteoporosis is highly prevalent in Japanese males with chronic obstructive pulmonary disease and is associated with deteriorated pulmonary functionJ Bone Miner Metab Epub201475
- HattiholiJGaudeGSPrevalence and correlates of osteoporosis in chronic obstructive pulmonary disease patients in IndiaLung India201431322122725125807
- LiLBrennanKJGaughanJPCiccolellaDEKuzmaAMCrinerGJAfrican Americans and men with severe COPD have a high prevalence of osteoporosisCOPD20085529129718972277
- SilvaDRCoelhoACDumkeAOsteoporosis prevalence and associated factors in patients with COPD: a cross-sectional studyRespir Care201156796196821352667
- RittayamaiNChuaychooBSriwijitkamolAPrevalence of osteoporosis and osteopenia in Thai COPD patientsJ Med Assoc Thai20129581021102723061305
- JørgensenNRSchwarzPHolmeIHenriksenBMPetersenLJBackerVThe prevalence of osteoporosis in patients with chronic obstructive pulmonary disease: a cross sectional studyRespir Med2007101117718516677808
- FergusonGTCalverleyPMAndersonJAPrevalence and progression of osteoporosis in patients with COPD: results from the TOwards a Revolution in COPD Health studyChest200913661456146519581353
- Graat-VerboomLSmeenkFWvan den BorneBERisk factors for osteoporosis in Caucasian patients with moderate chronic obstructive pulmonary disease: a case control studyBone20125061234123922426499
- Graat-VerboomLSmeenkFWvan den BorneBEProgression of osteoporosis in patients with COPD: a 3-year follow up studyRespir Med2012106686187022369986
- SundhJJohanssonGLarssonKComorbidity and health-related quality of life in patients with severe chronic obstructive pulmonary disease attending Swedish secondary care unitsInt J Chron Obstruct Pulmon Dis20151017318325653516
- LinMSHsuKYChenYJChenCRChenCMChenWPrevalence and risk factors of asymptomatic peripheral arterial disease in patients with COPD in TaiwanPLoS One201385e6471423717654
- JohannessenANilsenRMStorebøMGulsvikAEaganTBakkePComparison of 2011 and 2007 Global Initiative for Chronic Obstructive Lung Disease guidelines for predicting mortality and hospitalizationAm J Respir Crit Care Med20131881515923590268
- BrunaderRSheltonDKRadiologic bone assessment in the evaluation of osteoporosisAm Fam Physician20026571357136411996418
- Le GallJRLemeshowSSaulnierFA new Simplified Acute Physiology Score (SAPS II) based on a European/North American multicenter studyJAMA199327024295729638254858
- GenantHKDelmasPDChenPSeverity of vertebral fracture reflects deterioration of bone microarchitectureOsteoporos Int2007181697617028792
- GenantHKWuCYvan KuijkCNevittMCVertebral fracture assessment using a semiquantitative techniqueJ Bone Miner Res199389113711488237484
- MahlerDAWellsCKEvaluation of clinical methods for rating dyspneaChest19889335805863342669
- JonesPWQuirkFHBaveystockCMLittlejohnsPA self-complete measure of health status for chronic airflow limitation. The St George’s Respiratory QuestionnaireAm Rev Respir Dis19921456132113271595997
- JonesPWHardingGBerryPWiklundIChenWHKline LeidyNDevelopment and first validation of the COPD Assessment TestEur Respir J200934364865419720809
- MahlerDAHarverAA factor analysis of dyspnea ratings, respiratory muscle strength, and lung function in patients with chronic obstructive pulmonary diseaseAm Rev Respir Dis19921452 Pt 14674701736759
- van ManenJGBindelsPJDekkerFWIJzermansCJvan der ZeeJSSchadéERisk of depression in patients with chronic obstructive pulmonary disease and its determinantsThorax200257541241611978917
- McGarveyLLeeAJRobertsJGruffydd-JonesKMcKnightEHaughneyJCharacterisation of the frequent exacerbator phenotype in COPD patients in a large UK primary care populationRespir Med2015109222823725613107
- MontalciniTRomeoSFerroYMigliaccioVGazzarusoCPujiaAOsteoporosis in chronic inflammatory disease: the role of malnutritionEndocrine2013431596423055015
- LloydJTAlleyDEHawkesWGHochbergMCWaldsteinSROrwigDLBody mass index is positively associated with bone mineral density in US older adultsArch Osteoporos20149117524664472
- HoxhaRIslamiHQorraj-BytyqiHThaçiSBahtiriERelationship of weight and body mass index with bone mineral density in adult men from KosovoMater Sociomed201426530630825568627
- NagiRDeviBKRakeshNReddySSSantanaNShettyNRelationship between femur bone mineral density, body mass index and dental panoramic mandibular cortical width in diagnosis of elderly postmenopausal women with osteoporosisJ Clin Diagn Res201488ZC36ZC4025302265
- PinnettiCRelationship between body mass index and bone mineral density in HIV-infected patients referred for DXAJ Int AIDS Soc2014174 Suppl 31956925394076
- JeonYKShinMJKimWJThe relationship between pulmonary function and bone mineral density in healthy nonsmoking women: the Korean National Health and Nutrition Examination Survey (KNHANES) 2010Osteoporos Int20142551571157624577346
- GrossmanJMGordonRRanganathVKAmerican College of Rheumatology 2010 recommendations for the prevention and treatment of glucocorticoid-induced osteoporosisArthritis Care Res (Hoboken)201062111515152620662044
- LokeYKCavallazziRSinghSRisk of fractures with inhaled corticosteroids in COPD: systematic review and meta-analysis of randomised controlled trials and observational studiesThorax201166869970821602540
- HsuKYLinJRLinMSChenWChenYJYanYHThe modified Medical Research Council dyspnoea scale is a good indicator of health-related quality of life in patients with chronic obstructive pulmonary diseaseSingapore Med J201354632132723820542
- MillerJEdwardsLDAgustíAComorbidity, systemic inflammation and outcomes in the ECLIPSE cohortRespir Med201310791376138423791463
- SinDDManJPManSFThe risk of osteoporosis in Caucasian men and women with obstructive airways diseaseAm J Med20031141101412543283