Abstract
Background
Depression is a common psychiatric disorder worldwide, including in Iran, and is estimated to affect 10%–15% of the population. Antidepressant drugs can have multiple side effects, so a good choice of drug is important for successful treatment. This study compared the efficacy of nortriptyline with that of fluoxetine in the treatment of patients with major depressive disorder and assessed related factors, including age, gender, and level of education.
Methods
The study was a double-blind, randomized clinical trial with a six-month follow-up period. Participants were 120 patients aged 15–60 years with a diagnosis of major depressive disorder based on a psychiatry interview and the Beck depression rating scale, which were performed at the beginning, middle, and end of the study. The patients were treated with nortriptyline or fluoxetine. The paired t-test, independent t-test, and the k chi-square test were used to analyze the data.
Results
Twenty-three patients dropped out and 97 remained in the trial. Before intervention, the mean depression score was 32.85 ± 6.23 in the nortriptyline group and 33.12 ± 6.50 in the fluoxetine group. The results of the independent t-test showed a significant difference between depression score means before and after treatment in both groups. Changes at the end of the trial compared with baseline scores were 13.4 ± 4.68 and 16.96 ± 4.96 for nortriptyline and fluoxetine, respectively. Paired t-testing showed a significant difference in the mean depression score for both the nortriptyline and fluoxetine groups. Age, gender, and level of education had no significant effects on the outcome of treatment in the two groups.
Conclusion
The present study suggests that both nortriptyline and fluoxetine were effective in the treatment of depression, but that fluoxetine was more effective than nortriptyline after 3 and 6 months of treatment.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Introduction
Depression is a common psychiatric disorder characterized by a number of signs and symptoms which may include depressed mood, anhedonia, insomnia, anorexia, difficulty in concentration, and suicidal thought. The lifetime prevalence of the condition in the general population is reported to be 10%–15%, but in women has been reported to be up to 25%.Citation1–Citation3 Depression is much more common in women, occurring in a ratio of 2:1, and is the leading cause of disease-related disability in women.Citation4,Citation5 Mental health patterns in Iran are similar to those in other countries, but it seems that the prevalence of mental health disorders in Iran is lower than reported elsewhere. A review of the literature shows a prevalence rate for depression of 4.29% in Iran.Citation6,Citation7
Treatment of depression includes pharmacotherapy and psychotherapy. The common antidepressant drugs are tricyclic antidepressants, heterocyclic antidepressants, monoamine oxidase inhibitors, selective serotonin reuptake inhibitors (SSRIs), and sympathomimetics.Citation8,Citation9 The side effects of SSRI are reported to be nausea, headache, anger, weight loss, insomnia, yawning, diarrhea, weakness, fatigue, and dyspepsia. The side effects reported for tricyclic antidepressants include drowsiness, anticholinergic effects, weight gain, hypotension, tiredness, dullness, and tachycardia. Among the tricyclic antidepressants, nortriptyline is said to have the fewest complications. Fluoxetine was the first of the SSRIs to be introduced onto the US market and remains the most commonly used antidepressant agent in the US.Citation10–Citation13
There are some controversies about the effectiveness of nortriptyline and fluoxetine in the treatment of depression. While some studies have shown that nortriptyline is more effective than fluoxetine,Citation13–Citation16 others have shown fluoxetine to be more effective than nortriptyline.Citation12,Citation17,Citation18 On the other hand, some studies have shown that there was no significant difference between the two drugs,Citation19–Citation21 although some researchers believe that there is a significant difference between the two drugs depending on age and gender.Citation22 SSRIs are believed to be better tolerated and to have a better safety profile than the tricyclic antidepressants.Citation20,Citation23,Citation24 The aim of this study was to compare the efficacy and patient satisfaction profile for nortriptyline with that of fluoxetine in the treatment of major depressive disorder and to determine the influence of related factors, including gender, age, and educational level, on outcome.
Materials and methods
This study was a randomized, double-blind, clinical trial with a 6-month follow-up period carried out in 120 patients referred to the Shahid Mofatteh Psychiatric Clinic, Yasuj, Iran, from 2007 to 2008. The patients were selected by convenience sampling and randomized to one of two treatment groups. Twenty-three participants did not complete the study as a result of lack of cooperation, not taking the drugs regularly, and lack of punctuality. Inclusion criteria were being aged 15–60 years and a diagnosis of major depressive disorder on the basis of an interview and the Beck depression rating scale. Patients were excluded if they had received any antidepressant drug previously, had criteria for grief, adjustment disorder, major depressive disorder with psychotic features, had concomitant axis II or III disorder, a history of bipolar disorder, or schizophrenia. Women were excluded if they were pregnant or breast-feeding. Patients who did not respond to the drugs within 8 weeks were also excluded. This research was approved by the ethics committee and vice chancellor for research at Yasuj University of Medical Sciences. Patients were informed about the survey, and written consent was obtained from all participants or their legal guardians.
The study data were gathered from interviews with participants at the beginning of the study, and by clinical examination and using the Beck depression rating scale at the beginning, middle, and end of the study. The Beck depression inventory was used because it has been localized and validated for Iran. It also has appropriate reliability and validity.Citation25,Citation26 Both patients and the evaluating team were unaware of treatment allocation.
The patients received nortriptyline or fluoxetine treatment for 6 months. At the end of trial, 23 patients had withdrawn and 97 had remained. For the Beck depression inventory, a score >10 was considered to be depression, with 10–19 scored as mild, 20–29 as moderate, 30–39 as partially severe, and >40 as severe depression.Citation27,Citation28 All participants had a score ≥30 (severe depression). Nortriptyline up to 150 mg/day or fluoxetine up to 60 mg/day was used for 6 months according to the severity of depression. Another self-developed questionnaire was used to record the age, gender, and educational level of the participants. Educational level was divided into four groups, ie, illiterate, primary school, high school, and university graduate. For illiterate cases, the questions were read out verbally and a complete verbal explanation was given.
A questionnaire was developed to measure the patient’s satisfaction with their trial medication and any side effects. It consisted of 11 items measured on a three-point Likert scale (1 = unsatisfied, 2 = fairly satisfied, 3 = satisfied). The reliability of the instruments was measured using Cronbach’s alpha. The reliability index was good at 8.41. Drug side effects were also recorded.
Statistical analysis
The paired t-test was used to compare mean Beck test scores for each group before and after treatment. The independent t-test was used to compare the means of the two groups at baseline, and at 3-month and 6-month follow-up. Paired t-tests were used to compare mean depression scores at the beginning of treatment with those at the 3-month and 6-month follow-up. The total score for satisfaction in terms of side effects and treatment outcome was estimated, and using cut-off points of 40 and 60 was converted into qualitative scores of satisfied, partially satisfied, and unsatisfied. Fisher’s Exact test was then used to calculate the total satisfaction scores for the two treatment groups. The results are presented as the mean ± standard deviation, and the significance level was set at P < 0.05.
Results
There were approximately equal numbers of men and women in both treatment groups, and the mean age was 35 years (). – show that there was no significant difference between the two groups with regard to basic demographic data including age, gender, and educational level. The results also indicate that there was no significant difference between the two groups for mean Beck depression test scores before intervention. However, there was a significant difference for these scores between the groups after 3 and 6 months of treatment (). Both drugs were effective in major depression at 3 and 6 months of follow-up, but fluoxetine was more effective than nortriptyline (). The results also indicate that there was a significant difference between the groups for mean Beck depression score before and after 3 and 6 months of treatment (P < 0.05, ). The descriptive statistics shown in indicate that the changes in mean Beck depression score at the end of the study compared with baseline was 16.96 ± 4.96 and 13.14 ± 4.68 for fluoxetine and nortriptyline, respectively.
Figure 1 Comparison of mean Beck depression scores for patients referred to Yasuj Psychiatry Clinic according to treatment allocation.
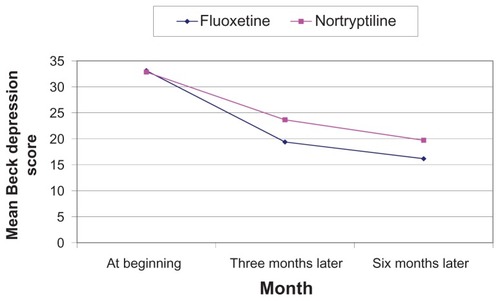
Table 1 Baseline data for fluoxetine and nortriptyline groups
Table 2 Comparison of mean Beck depression scores according to age before and after 3 and 6 months of treatment with fluoxetine or nortriptyline
Table 3 Comparison of mean Beck depression scores according to gender before and after 3 and 6 months of treatment with fluoxetine or nortriptyline
Table 4 Comparison of mean Beck depression scores based on educational level before and after 3 and 6 months of treatment with fluoxetine or nortriptyline
Table 5 Mean Beck scores for depressed patients referring to Yasuj Psychiatric Clinic, Iran, by time and kind of treatment
Both drugs had side effects, including headache, drowsiness, constipation, anorexia, nausea, and vomiting. Fluoxetine was significantly correlated with nausea while nortriptyline was not. Nortriptyline was significantly correlated with headache, dizziness, drowsiness, weakness, aggression, and constipation (). Total satisfaction with the drugs was estimated by patient perception of side effects, and the outcomes were compared between the two groups. The results indicated the patients were more satisfied with fluoxetine than with nortriptyline ().
Table 6 Mean percent frequency of treatment-emergent adverse events
Table 7 Satisfaction profile for nortriptyline and fluoxetine in depressed patients referred to Yasuj Psychiatry Clinic, Iran
Discussion
Depression is a common psychiatric disorder which may cause depressed mood, anhedonia, insomnia, anorexia, difficulty in concentration, and suicidal thought. It can be treated by both psychotherapy and pharmacotherapy. Tricyclic antidepressants and SSRIs are drugs commonly used in the treatment of depression. This study compared the efficacy of nortriptyline (a tricyclic antidepressant) and fluoxetine (an SSRI) in the treatment of patients with major depressive disorder. Its findings suggest that both nortriptyline and fluoxetine were effective, which is in agreement with other studies. However, fluoxetine was more effective than nortriptyline in the treatment of major depressive disorder, and age, gender, and educational level of the patients did not have a significant impact on the treatment.
Our results are different from those of previous studies reported by Fabre et al, Roose et al, Akhondzadeh et al, and Robinson et al.Citation13–Citation16 These reported that nortriptyline was more effective than fluoxetine. Roose et al also reported that nortriptyline was more effective than fluoxetine in depression with melancholic features. Our results are also different in this respect from the studies reported by Anderson et al, Finkel et al, and Song et al, Citation19–Citation21 Further, unlike Joyce et al, who reported that older male melancholic patients had a markedly superior response to nortriptyline compared with fluoxetine, and that young female melancholic patients had a markedly superior response to fluoxetine,Citation22 the results of our study showed that fluoxetine is more effective than nortriptyline but with no effect of age and gender.
However, the results of our study are similar to those of Khade et al, Attari et al, Bhurghri et al, and Anderson et al.Citation12,Citation17–Citation19 In our study, fluoxetine was compared with nortriptyline, but in the study by Khade et al nortriptyline was compared with fluvoxamine (an SSRI), and fluvoxamine was reported to be better than nortriptyline.Citation12
In terms of toxicity, it could be argued that both drugs had some side effects. In our study fluoxetine was associated with nausea, similar to other studies.Citation10–Citation13,Citation23,Citation24 Meanwhile, Khade et al and Otsubo et al reported that fluvoxamine was associated with nausea and Uher et al reported that escitalopram was associated with insomnia, diarrhea, and yawning.Citation10,Citation12,Citation24 In our study, fluoxetine was significantly associated with nausea, whereas Bhurghri et al reported that nortriptyline was significantly associated with nausea and headache.Citation18 Our results indicate that nortriptyline was not significantly associated with dry mouth, but other studies have found this relationship. In our study, nortriptyline was significantly associated with headache, dizziness, constipation, drowsiness, weakness, and aggression, which seems to be in line with other studies.Citation10–Citation13,Citation23,Citation24 Khade et al reported that drowsiness, tiredness, and dullness were related to this drug, and Uher et al further reported that dry mouth, constipation, and weight gain were associated with nortriptyline.Citation10,Citation12
Based on the results of our study, which are consistent with those of Finkel et al, Kasper et al, and Otsubo et al,Citation20,Citation23,Citation24 it could be argued that the patient satisfaction and tolerability profiles of fluoxetine are better than those of nortriptyline (). Finally, we can conclude that fluoxetine and nortriptyline are effective in major depressive disorder, but that fluoxetine was more effective than nortriptyline, and age, gender, and educational level did not contribute to the efficacy profiles of these drugs.
Acknowledgments
The authors thank all the patients who participated in this study along with their families. They are also grateful to staff of the Research Center of Social Factors Affecting Health, Yasuj University of Medical Sciences, for their support, and our colleagues in Rajaee Hospital, Shahid Mofatteh Psychiatric Clinic, and the vice chancellor for research, Yasuj University of Medical Sciences for assistance with this study.
Disclosure
The authors report no conflicts of interest in this work.
References
- KesslerRCWaltersEEEpidemiology of DSMIII-R major depression and minor depression among adolescents and young adults in the National Comorbidity SurveyDepress Anxiety199873149592628
- HirschfieldRMajor depression, dysthymia and depressive personality disorderBr J Psychiatry Suppl19942623307873134
- KaelberCTMoulDEFarmerMEEpidemiology of depressionBeckhamEELeberWRHandbook of Depression2nd edNew York, NYGuilford Press2009
- KesslerRCEpidemiology of women and depressionJ Affect Disord20037451312646294
- WeissmanMMBlandRJoycePRSex difference in rates of depression: cross-national perspectiveJ Affect Disord19932977848300980
- MohammadiMRDavidianHNoorbalaAAAn epidemiological survey of psychiatric disorders in IranClin Pract Epidemiol Ment Health200511616185355
- NoorbalaAABagheri YazdiSAYasamyMTMohammadKMental health survey of the adult population in IranBr J Psychiatry2004184707314702230
- GelderMMayouRGeddesJConcise Oxford Textbook of Psychiatry2nd edNew York, NYOxford University Press1999
- SadockSJKaplanHIMood disorders: clinical featuresKaplan and Sadock’s Synopsis of Psychiatry9th edPhiladelphia, PALippincott Williams and Wilkins2003
- UherRFarmerAHenigsbergNAdverse reactions to antidepressantsBr J Psychiatry2010192202207
- DalyEJTrivediMHFavaMThe relationship between adverse event during selective serotonin reuptake inhibitor treatment for major depressive disorder and non remission in the suicide assessment methodology studyJ Clin Psychopharmacol201131313821192140
- KhadeABasirMKaleASTurankarAStudy of the effect of nortriptyline and fluvoxamine on psychomotor functions in healthy volunteersIndian J Psychol Med20103210410721716778
- FabreLFScharfMBItilTMComparative efficacy and safety of nortriptyline and fluoxetine in the treatment of major depression: a clinical studyJ Clin Psychiatry199152 Suppl62672050651
- RooseSPGlassmanAHAttiaEComparative efficacy of selective Serotonin reuptake inhibitors and Tricyclic in the treatment of melancholiaAm J Psychiatry1994151173517397977878
- AkhondzadehSFarajiHSadeghiMAfkhamKFakhrzadehHKamalipourADouble-blind comparison of fluoxetine and nortriptyline in the treatment of moderate to severe major depressionJ Clin Pharm Ther20032837938414632962
- RobinsonRGSchultzSKCastilloCNortriptyline versus fluoxetine in the treatment of depression and in short-term recovery after stroke: a placebo-controlled, double-blind studyAm J Psychiatry200015735135910698809
- AttariAMoghadamYHassanzadehMSComparison of efficacy with nortriptyline and fluoxetine in treatment of major depression in children and adolescents: a double blind studyJ Res Med Sci2006112430
- BhurghriGRKorejoHBQureshiMARole of fluoxetine and nortriptyline in major depressive disordersRawal Medical Journal2011363840
- AndersonIMTomensonBMThe efficacy of selective serotonin reuptake inhibitors in depression: a meta analysis of studies against tricyclic antidepressantsJ Psychopharmacol1994823824922298630
- FinkelSIEfficacy and tolerability of antidepressant therapy in the old-oldJ Clin Psychiatry199657 Suppl23288647789
- SongFFreemantleNSheldonTASelective reuptake inhibitors: meta analysis of efficacy and acceptabilityBr Med J19933066836878471919
- JoycePRMulderRTLutySEMcKenzieJMRaeAMA differential response to nortriptyline and fluoxetine in melancholic depression: the importance of age and genderActa Psychiatr Scand2003108202312807373
- KasperSHoflichGSchollHPSafety and antidepressant efficacy of selective serotonin re-uptake inhibitorsHum Psychopharmacol19949112
- OtsuboTAkimotoYYamadaHA comparative study of the efficacy and safety profile between fluvoxamine and nortriptyline in Japanese patients with major depressionPharmacopsychiatry200538303515706464
- GhassemzadehHMojtabaiRKaramghadiriNEbrahimkhaniNPsychometric properties of a Persian-language version of the Beck depression inventory – second edition: BDI-II-PERSIANDepress Anxiety20052118519216075452
- DadsetanBMansoriAValidity and reliability of Beck depression test in social survey198721223 In Farsi
- BeckATSteerRAGarbinMGPsychometric properties of the Beck depression inventoryClin Psychol Rev198877100
- DobsonKSMohammad KhaniPPsychometric characteristics of the Beck Depression InventoryJournal of Rehabilitation20072982 Farsi