Abstract
Background
Hyaluronic acid has been extensively used for treatment of knee osteoarthritis due to its anti-inflammatory properties and its ability to act as a synovial lubricant. Furthermore, it has found application in combination with other drugs in the dermatological field and in pre-clinical studies in animal models of osteoarthritis. Experimental evidence suggests that a combination of this macromolecule with other drugs may act as a slow-release depot. However, to date, to the best of our knowledge, no one has tested local intra-articular delivery of highly cross-linked hyaluronic acid combined with bisphosphonate or nonsteroidal anti-inflammatory drugs for management of knee osteoarthritis pain in the clinical setting. The aim of the present randomized double-blind study was to investigate, for the first time, the effect of a highly cross-linked hyaluronic acid, Variofill®, alone or in combination with diclofenac sodium or sodium clodronate, for management of bilateral knee osteoarthritis-related pain.
Methods
Sixty-two patients with symptomatic bilateral medial tibiofemoral knee osteoarthritis (Kellgren–Lawrence grade II and III) and pain in both knees corresponding to a daily visual analog scale (VAS) score ≥ 30 in the month before the beginning of the study were included in this investigation. Patients were divided into three groups: group 1, treated with an injection of hyaluronic acid alone (66 mg) into each knee; group 2, treated with an injection of hyaluronic acid (49.5 mg) plus diclofenac sodium (5 mg) into each knee; group 3, treated with an injection of hyaluronic acid (49.5 mg) plus sodium clodronate (5 mg) into each knee. Patients also underwent blood tests for measurement of erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) immediately before and at 6-month follow-up.
Results
Hyaluronic acid alone and in combination with sodium clodronate or diclofenac sodium produced a significant improvement in mean VAS pain score at 3 and 6-month follow-up. At 6-month follow-up, therapy with hyaluronic acid plus sodium clodronate was the most beneficial in terms of percentage improvement in VAS pain score. A significant improvement in ESR and CRP was observed at 6-month follow-up in each treatment group. No significant difference was observed when the percentage change from baseline related to these parameters was compared among the groups. No dropout was observed in any group. No serious adverse events were observed.
Conclusion
Further studies are necessary to determine the effect of a therapy based on hyaluronic acid combined with diclofenac sodium or sodium clodronate in larger cohorts of patients affected by knee osteoarthritis and in longer-term follow-up.
Introduction
Hyaluronic acid has been widely used for viscosupplementation in patients affected by knee osteoarthritis.Citation1 This is due to its ability to interact with collagen and chondrocytes, leading to modulation of angiogenic and inflammatory mediators.Citation2 In our clinic we had previous experience with Variofill®, a 100% cross-linked hyaluronic acid formula characterized by very high viscoelasticity. Variofill® is prepared from 33 mg/mL non-cross-linked hyaluronic acid, followed by an extended cross-linking process with divinyl sulfone, fragmentation of the strong cross-linked hyaluronic acid gel mass, and homogenization without dilution. The final product is highly viscoelastic and easily injectable. Hyaluronic acid has already been used in combination with other compounds in experimental models of osteoarthritis. For instance, a combination of hyaluronic acid and growth hormone has been attempted in a rabbit model of collagenase-induced arthritis, suggesting that injections of this mixture are more effective than hyaluronic acid alone, as reflected by a lower histopathological score and less cartilage damage. Citation3 In a further experimental study, diclofenac and dexamethasone, alone or in combination, have been delivered to the knee joint in a single injection using bioadhesive liposomes carrying hyaluronan or collagen as their surface-anchored ligand in the rat monosodium iodoacetate model of osteoarthritis. Citation4 In this study, every therapeutic regimen reduced osteoarthritis-related inflammation over a period of 17 days. However, a combination of both drugs and liposomes carrying hyaluronan was the most effective. This study also showed highly efficient drug encapsulation for all compounds tested and an ability to function as slow-release depots.Citation4 Many studies have investigated the effect of topical application of a combination of hyaluronic acid and diclofenac for treatment of skin-related pathologies. For instance, Lima et al showed that topical application of 3% diclofenac in 2.5% hyaluronic acid gel in the area affected by actinic cheilitis resulted in total remission of the condition in 44% of patients who completed the study.Citation5 In 56% of patients, a partial remission of plaques was observed. Topical application of diclofenac and hyaluronic acid has also been studied in the context of actinic keratosis, showing that a topical combination of diclofenac 3% and hyaluronic acid 2.5% for 90 days produced a reduction in the expression of three markers of inflammation, ie, cyclooxygenase-2 (COX-2), CD3 and CD8 in 20 patients.Citation6 In the orthopaedic clinic, local bisphosphonate injection has already been investigated. For instance, a clinical study involving 20 patients affected by synovitis secondary to knee osteoarthritis investigated the effect of repeated intra-articular injection of clodronate, and showed a statistically significant reduction in spontaneous pain and pain on active movement, as assessed by visual analog scale (VAS).Citation7 In this study, the decrease in pain was correlated with a bisphosphonate-induced reduction in prostaglandin E2 levels. Repeated administration of clodronate has also been tested at different doses (0.5 mg, 1 mg, and 2 mg injection once a week for 4 weeks and two 1 mg injections once a week for 2 weeks) versus injection of 20 mg hyaluronic acid once a week for 4 weeks in patients affected by knee osteoarthritis.Citation8 In this study, intra-articular clodronate resulted in symptomatic and functional improvements as good as those obtained with hyaluronic acid and they persisted for at least 2 weeks following the last injection.Citation8
To date, to the best of our knowledge, no one has tested local intra-articular delivery of highly cross-linked hyaluronic acid combined with bisphosphonate or nonsteroidal anti-inflammatory drugs for the management of knee osteoarthritis-related pain in the clinical setting. The aim of this study was to determine the effectiveness of a single injection of the new highly cross-linked hyaluronic acid Variofill®, alone or in combination with diclofenac sodium or sodium clodronate, for management of bilateral knee osteoarthritis-related pain.
Materials and methods
The inclusion criteria for this double-blind randomized study were symptomatic bilateral medial tibiofemoral knee osteoarthritis (Kellgren–Lawrence grade II and IIICitation9), as assessed by x-rays taken 2–3 months prior to the beginning of the study and pain in both knees corresponding to daily VAS ≥ 30 mm in the previous month. Exclusion criteria were: unilateral knee osteoarthritis or unilateral/bilateral knee osteoarthritis concerning predominantly the patellofemoral region, meniscal-related or ligamentous-related instability as assessed by physical examination, any prior viscosupplementation or intra-articular injection of corticosteroids or any other drugs into the knee during the 5 months prior to the beginning of the study and presence of concomitant pathology affecting the knee.
One hundred and twenty-two patients were screened. Sixty patients were not included in the study because they did not meet the inclusion criteria. Sixty-two patients (37 men and 25 women) signed the informed consent and participated in the present study. The mean age was 50.9 ± 1.04 years and the mean body mass index was 21.5 ± 0.2 kg/m2. The protocol was planned and carried out in agreement with the Declaration of Helsinki. The study was approved by the institutional review board at Poliambulatorio del Secondo Parere (Modena, Italy) where the patients were recruited and the procedure was performed. In order to allow random allocation of patients to different treatment groups, two operators undertook recruitment and patient list construction (patient names were allocated randomly to treatment group from a computer-generated list). The primary outcome measurement was knee pain as assessed by VAS (0–100 mm, 0 = no pain, 100 = very severe pain) at baseline and at 3 and 6 months after treatment (VAS pain score was calculated for each knee and then values were averaged together). Secondary outcome measures were erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) assessed by blood tests performed immediately before and at 6-month follow-up.
Patients were divided into three groups in a randomized fashion. Group 1 (n = 20) was treated with an injection of hyaluronic acid alone (66 mg/2 mL [Variofill®, Adoderm, GmbH, Langenfeld, Germany]) into each knee; group 2 (n = 21) was treated with an injection of hyaluronic acid (49.5 mg/1.5 mL [Variofill®, Adoderm, GmbH, Langenfeld, Germany]) plus diclofenac sodium (0.5 mL/5 mg [INFORCE, IBSA, Lugano, Switzerland]) into each knee; and group 3 (n = 21) was treated with an injection of hyaluronic acid (49.5 mg/1.5 mL [Variofill®, Adoderm, GmbH, Langenfeld, Germany]) plus sodium clodronate (0.5 mL/5 mg [Clasteon®, Abiogen Pharma, Pisa, Italy]) into each knee. The overall volume injected was 2.5 mL because 0.5 mL of 1% lidocaine (Angelini, Rome, Italy) was added to every injection in order to relieve injection-related pain.
Injections were prepared under aseptic conditions by the same operator throughout the study using an emulsification needle to obtain a complete physical mixture of the drugs before delivery. The study injections were given by a surgeon who was blinded for the duration of the study. The patients were also blinded to their treatment allocation. Following viscosupplementation, all patients were advised to avoid NSAIDs for 6 months, but paracetamol, at a maximum dose of 2000 mg/day, was allowed for pain management. All patients were advised to stop paracetamol for 24 hours before assessment at 3- and 6-month follow-up examination.
Statistical analysis
The data were analyzed using GraphPad Prism 5 software. Percentage change in VAS score from baseline was calculated for all groups. One-way analysis of variance using the post hoc Bonferroni test was used to compare percentage change in VAS pain score, ESR, and CRP among the three treatment groups. A value of P < 0.05 was considered significant. Data are presented as the mean ± standard error of the mean (SEM).
Results
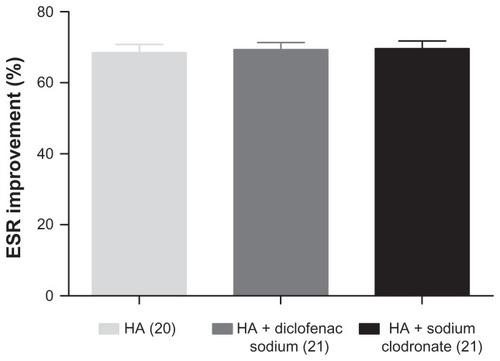
A one-way analysis of variance showed that hyaluronic acid alone or in combination with sodium clodronate or diclofenac sodium produced a significant improvement in mean VAS pain score in patients affected by bilateral knee osteoarthritis (–). Group 1 showed a decrease in VAS pain score from a mean baseline value of 67.5 ± 2.04 mm to 46.8 ± 2.09 mm at 3 months and to 31.3 ± 2.4 mm at 6 months. Group 2 showed a decrease in VAS pain score from a mean baseline value of 71.9 ± 1.1 mm to 48.86 ± 0.9 mm at 3 months and to 32.1 ± 1.1 mm at 6 months. Group 3 showed a decrease in VAS pain score from a mean baseline value of 76.9 ± 1.9 mm to 47.5 ± 1.05 mm at 3 months and to 26.8 ± 1.2 mm at 6 months. When comparing the percentage change in mean VAS pain score from baseline in the three treatment groups, the therapy including sodium clodronate was the most beneficial in terms of percentage improvement in VAS pain score (10.1% improvement versus group 1; 8.8% improvement versus group 2; ). A significant decrease in ESR and CRP versus baseline was observed at 6 months after the procedure in each treatment group. In group 1, ESR decreased from 76.4 ± 2.6 mm/hr to 23.7 ± 1.5 mm/hr (P ≤ 0.001) and CRP decreased from 7.4 ± 0.3 mg/L to 1.5 ± 0.09 mg/L (P ≤ 0.001). In group 2, ESR decreased from 77.1 ± 2.5 mm/hr to 23.2 ± 1.1 mm/hr (P ≤ 0.001) and CRP decreased from 7.1 ± 0.3 mg/L to 1.8 ± 0.1 mg/L (P ≤ 0.001). In group 3, ESR decreased from 76.7 ± 2.5 mm/hr to 22.8 ± 1.2 mm/hr (P ≤ 0.001) and CRP decreased from 6.8 ± 0.3 mg/L to 1.5 ± 0.08 mg/L (P ≤ 0.001). No significant difference was observed when the percentage change from baseline related to these parameters was compared among the groups ( and ). No dropouts and no serious adverse events were observed in any group. Some bruising at 4 hours after injection containing sodium clodronate was reported by four patients, but resolved without any further treatment. No pain was observed at the injection site.
Figure 1 Effect of hyaluronic acid injection on VAS pain score at 3- and 6-month follow-up in 20 patients affected by bilateral osteoarthritis of the knee.
Abbreviations: VAS, visual analog score; SEM, standard error of mean.
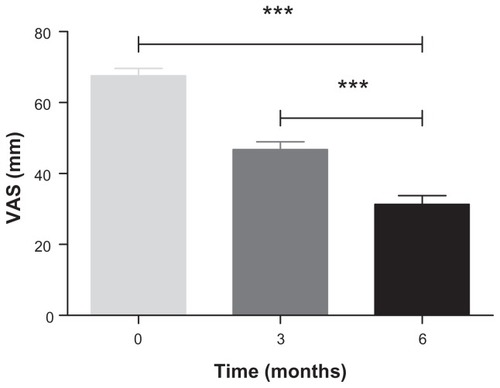
Figure 2 Effect of hyaluronic acid plus diclofenac sodium injection on VAS pain score at 3- and 6-month follow-up in 21 patients affected by bilateral osteoarthritis of the knee.
Abbreviations: VAS, visual analog score; SEM, standard error of mean.
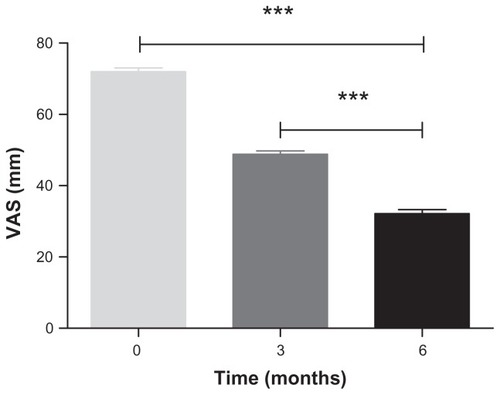
Figure 3 Effect of hyaluronic acid plus sodium clodronate injection on VAS pain score at 3- and 6-month follow-up in 21 patients affected by bilateral osteoarthritis of the knee.
Abbreviations: VAS, visual analog score; SEM, standard error of mean.
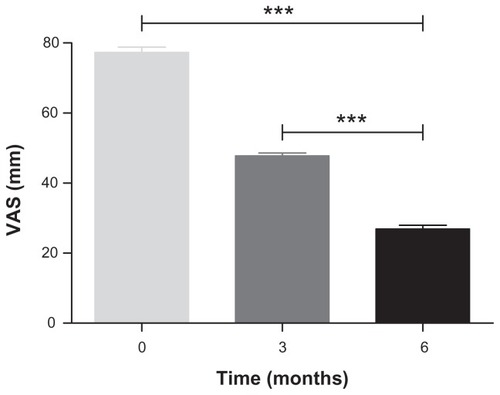
Figure 4 Percentage improvement in VAS pain score in patients affected by bilateral osteoarthritis of the knee at 6-month follow-up following hyaluronic acid alone (n = 20), hyaluronic acid plus diclofenac sodium (n = 21), and hyaluronic acid plus sodium clodronate (n = 21) injection.
Abbreviations: HA, hyaluronic acid; VAS, visual analog score; SEM, standard error of mean.
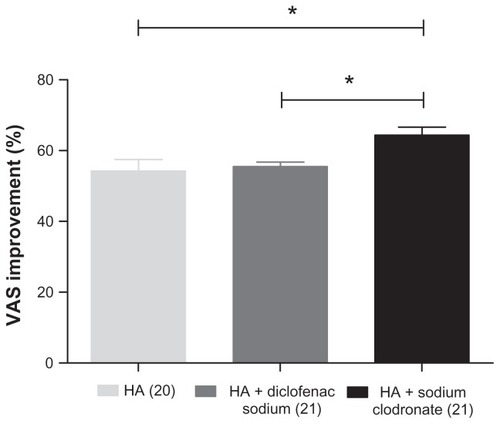
Figure 5 Percentage CRP improvement in patients affected by bilateral osteoarthritis of the knee at 6-month follow-up after hyaluronic acid alone (n = 20), hyaluronic acid plus diclofenac sodium (n = 21), and hyaluronic acid plus sodium clodronate (n = 21) injection.
Abbreviations: CRP, C-reactive protein; HA, hyaluronic acid; SEM, standard error of mean.
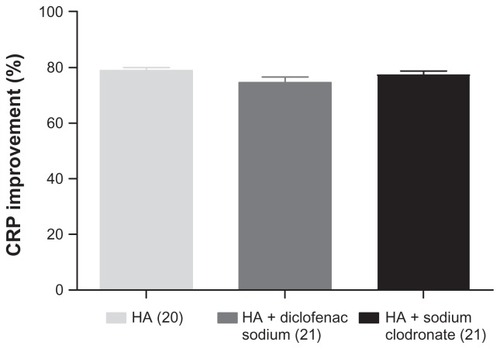
Figure 6 Percentage ESR improvement in patients affected by bilateral osteoarthritis of the knee at 6-month follow-up following hyaluronic acid alone (n = 20), hyaluronic acid plus diclofenac sodium (n = 21), and hyaluronic acid plus sodium clodronate (n = 21) injection.
Abbreviations: ESR, erythrocyte sedimentation rate; HA, hyaluronic acid; SEM, standard error of mean.
Discussion and conclusion
The present study was designed to investigate the effect of a combination of drugs mechanically mixed with a highly cross-linked hyaluronic acid gel, ie, Variofill®. Hyaluronic acid has well established evidence-based properties as a synovial lubricantCitation10,Citation11 and is effective in cartilage remodelling, Citation12 counteracting inflammatory breakdown.Citation13 Our study shows that intra-articular hyaluronic acid, alone or in combination with sodium clodronate or diclofenac sodium, improved VAS pain score in patients affected by bilateral osteoarthritis of the knee. This was consistent with a significant decrease in ESR and CRP at 6 months after the procedure in each treatment group and without significant intergroup differences.
ESR and CRP measurements have been extensively used in the orthopaedic and rheumatology clinics.Citation14–Citation16 In this study, ESR and CRP were used to monitor the effect of the proposed pharmacological intervention in a cost-effective fashion. In particular, CRP is present at elevated levels during the acute-phase response, but returns to physiological values following tissue recovery and functional restoration.Citation17 ESR is also a measure of the acute-phase response, although it may be affected by several factors.Citation18 Treatment with hyaluronic acid plus sodium clodronate showed an increased percentage improvement in VAS pain score, if compared with hyaluronic acid alone or hyaluronic acid plus diclofenac sodium. The use of different drugs in combination with hyaluronic acid allows an individually tailored approach that may further benefit the patient in terms of partial anatomical restoration and at least partial functional recovery. In patients with low-pain thresholds and those at an advanced disease stage, injection with bisphosphonates may be helpful to further control inflammation and inhibit bone resorption. In our experience, treatment with bisphosphonates gives better results in terms of pain management in the long term (6-month follow-up), probably as a result of their action targeting proinflammatory cytokines and bone cells.Citation19 Hyaluronic acid alone and in combination with diclofenac sodium also improved VAS pain score at 6-month follow-up, but to a lesser extent if compared with the regimen including sodium clodronate. According to these results, highly cross-linked hyaluronic acid is suitable for use in combination with other drugs, namely NSAIDs or bisphosphonates without complications, probably acting as a slow-release drug delivery system as shown previously by Elron-Gross and coworkers in an experimental rat model of osteoarthritis.Citation4 A limitation of the present study is the fact that we did not take into account functional outcome measures, such as the Western Ontario and McMaster Universities Osteoarthritis Index. However, this research was intended as a preliminary clinical study to address osteoarthritis-related pain. Further studies in larger cohorts of patients affected by knee osteoarthritis in longer-term follow-up are required.
Disclosure
The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in this work. The authors contributed equally to this work.
References
- Iannitti T Lodi D Palmieri B Intra-articular injections for the treatment of osteoarthritis: focus on the clinical use of hyaluronic acid Drugs R D 2011 11 1 13 27 21142290
- Garcia-Fuentes M Meinel AJ Hilbe M Meinel L Merkle HP Silk fibroin/hyaluronan scaffolds for human mesenchymal stem cell culture in tissue engineering Biomaterials 2009 30 28 5068 5076 19564040
- Kim SB Kwon DR Kwak H Additive effects of intra-articular injection of growth hormone and hyaluronic acid in rabbit model of collagenase-induced osteoarthritis J Korean Med Sci 2010 25 5 776 780 20436717
- Elron-Gross I Glucksam Y Margalit R Liposomal dexamethasone-diclofenac combinations for local osteoarthritis treatment Int J Pharm 2009 376 1–2 84 91 19409466
- da Lima GS Silva GF Gomes AP de Araujo LM Salum FG Diclofenac in hyaluronic acid gel: an alternative treatment for actinic cheilitis J Appl Oral Sci 2010 18 5 533 537 21085813
- Maltusch A Rowert-Huber J Matthies C Lange-Asschenfeldt S Stockfleth E Modes of action of diclofenac 3%/hyaluronic acid 2.5% in the treatment of actinic keratosis J Dtsch Dermatol Ges 2011 9 12 1011 1017 21585654
- Cocco R Tofi C Fioravanti A Effects of clodronate on synovial fluid levels of some inflammatory mediators, after intra-articular administration to patients with synovitis secondary to knee osteoarthritis Boll Soc Ital Biol Sper 1999 75 11–12 71 76 11433681
- Rossini M Viapiana O Ramonda R Intra-articular clodronate for the treatment of knee osteoarthritis: dose ranging study vs hyaluronic acid Rheumatology 2009 48 7 773 778 19406908
- Kellgren JH Lawrence JS Radiological assessment of osteo-arthrosis Ann Rheum Dis 1957 16 4 494 502 13498604
- Ogston AG Stanier JE The physiological function of hyaluronic acid in synovial fluid; viscous, elastic and lubricant properties J Physiol 1953 119 2–3 244 252 13035748
- Swann DA Radin EL Nazimiec M Weisser PA Curran N Lewinnek G Role of hyaluronic acid in joint lubrication Ann Rheum Dis 1974 33 4 318 326 4415649
- Homandberg GA Ummadi V Kang H Hyaluronan enhances cartilage repair through low grade tissue remodeling involving cytokines and matrix metalloproteinases Inflamm Res 2004 53 10 534 543 15597148
- Ialenti A Di Rosa M Hyaluronic acid modulates acute and chronic inflammation Agents Actions 1994 43 1–2 44 47 7741040
- Foglar C Lindsey RW C-reactive protein in orthopedics Orthopedics 1998 21 6 687 691 9642707
- Turan Y Bal S Gurgan A Topac H Koseoglu M Serum hyaluronan levels in patients with knee osteoarthritis Clin Rheumatol 2007 26 8 1293 1298 17205214
- van Leeuwen MA van Rijswijk MH Acute phase proteins in the monitoring of inflammatory disorders Baillieres Clin Rheumatol 1994 8 3 531 552 7525084
- Tarik MH David HK C-reactive protein and erythrocyte sedimentation rate in orthopaedics The University of Pennsylvania Orthopaedic Journal 2002 15 13 16
- Ng T Erythrocyte sedimentation rate, plasma viscosity and C-reactive protein in clinical practice Br J Hosp Med 1997 58 10 521 523 10193457
- Iannitti T Rosini S Lodi D Frediani B Rottigni V Palmieri B Bisphosphonates: focus on inflammation and bone loss Am J Ther 2012 19 3 228 246 22549638