Abstract
Men undergo gradual bone loss with aging, resulting in fragile bones. It is estimated that one in five men will suffer an osteoporotic fracture during their lifetime. The prognosis for men after a hip fracture is very grim. A major cause is reduction of free testosterone. Many other factors result in secondary osteoporosis, including treatment for other diseases such as cancer and diabetes. Patients should be screened not only for bone density but also assessed for their nutritional status, physical activity, and drug intake. Therapy should be chosen based on the type of osteoporosis. Available therapies include testosterone replacement, bisphosphonates, and nutritional supplementation with calcium, vitamin D, fatty acids, and isoflavones, as well as certain specific antibodies, like denosumab and odanacatib, and inhibitors of certain proteins.
Introduction
Aging is associated with gradual bone loss in men, leading to fragile bones and increased fracture risk. Since bone loss in males was recognized as a serious medical condition a couple of decades ago, studies have focused on several aspects of the disease, including assessment, diagnosis, prevention, and treatment options. It is established that aging men lose bone mineral density (BMD) at a rate of 1% per year,Citation1 and that one in five men will suffer an osteoporotic fracture during their lifetime.Citation2,Citation3 It is also believed that the incidence of osteoporosis-related fracture is similar to that of myocardial infarction and exceeds that of lung and prostate carcinoma combined.Citation4 The disturbing fact is that when men have fractures, their chances of survival are considerably decreased. Moreover, awareness about osteoporosis in males is lacking in certain societies.Citation5–Citation7
Although it is recognized that osteoporosis in men is an important medical condition and will remain important as longevity increases around the globe, there are very poor tools for managing male osteoporosis.Citation8,Citation9 The diagnostic standards are dependent on the scales for women or young men, but there is a 10-year difference in age before men show signs of an age-related decrease in bone mass.Citation10 Moreover, many elderly men treated for fractures are not put on any medication regimen to treat osteoporosis.Citation11 It is recommended that men should be evaluated for their bone status after 50 years of age,Citation12 and the clinical practice guidelines recommend screening in men over 70 years.Citation11,Citation13
Patients older than 80 years are currently excluded, but the changes in physiology at this age usually put them at a different level of risk.Citation14 Although screening patients for BMD is the best measure to know the status of bone, it is very important to collect information about the probable reasons for bone loss, because 75% of patients have been found to have secondary osteoporosis.Citation15 There may be ethnicity-related differences among men as well. Roughly 7% of white men and 3% of black men have osteoporosis, with an additional 35% of white men and 19% of black men having low bone mass. This requires formulation of treatment and management strategies specific to ethnic groups.Citation16 In addition to this, men with a combination of low bone mass and low muscle mass are at higher risk of losing bone. In this review, available data on the causes, consequences, and treatment options are discussed.
Causes and consequences
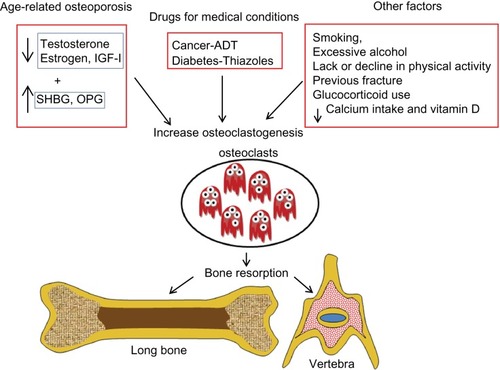
Several factors are believed to cause age-related bone loss in men, including decreased levels of sex hormones and insulin-like growth factor-1, drug side effects, and nutrition lacking minerals. Moreover, secondary osteoporosis may be due to several acquired habits and inherited conditions ().
Figure 1 Factors that cause bone loss in men.
Decrease in hormones
With age, there is certainly a decrease in hormone levels. Androgens may play an important role in the regulation of bone formation in men.Citation17 Total testosterone levels decrease at a rate of 0.8% per year, of which free and bound testosterone levels decrease at 2% per year (cross-sectional studies) and between 1.6% per year and 2%–3% per year (longitudinal studies).Citation18 On the other hand, levels of sex hormone binding globulin (SHBG) increase with age.Citation19–Citation23 This protein binds to testosterone and decreases free or bioavailable testosterone.Citation19,Citation21,Citation24–Citation26 Men are also affected by changes in estrogen due to aging, because testosterone is the precursor to estrogen and it is well established that estrogen plays a greater role in increasing bone resorption.Citation25 Therefore, in men, both hormones are important to maintain bone and are inversely related to fracture risk in older men contributed by decreased BMD.Citation27,Citation28 The action of androgen on bones in males may be explained by activation of the androgen receptor or the estrogen receptor (α and β).Citation28 Therefore, low serum estrogen and testosterone with high SHBG increases the risk of osteoporotic vertebral, nonvertebral, and hip fractures.Citation28,Citation29
Apart from alterations in sex hormones, decreased insulin-like growth factor-1 levels are found in men with vertebral fractures.Citation30 In addition, men with a low body mass index and a small body frame have decreased estrogen levels, and the offspring of these men also have low BMD.Citation31
Bone turnover and bone maintenance is a balance between proteins like osteoprotegerin and receptor activated nuclear factor kappa B ligand (RANKL). Osteoprotegerin levels in serum have been shown to increase with age,Citation32 which in turn may increase bone loss.
Side effects of drugs
Patients with prostate cancer undergoing androgen deprivation and cyclophosphamide therapy have an increased fracture risk.Citation33–Citation36 BMD measurements in men with prostate cancer and under an androgen deprivation regimen show 6.5%–17.3% bone loss. Moreover, this effect is site-specific and is also dependent on duration of treatment.Citation37–Citation39
Antidiabetic drugs like thiazides also cause bone loss.Citation40 Many studies in humans as well as in animals have shown that bone loss is accelerated by thiazoles.Citation41–Citation43 Rosiglitazone decreases bone quality by increasing porosity.Citation40 In women and men, decreased bone mass in long bones, but not in the vertebrae, has been attributed to thiazides.Citation44,Citation45 There are a few studies that explain the mechanism by which these antidiabetic drugs cause bone loss. In males, glitazones reduce the biosynthesis of androgens, increase their binding to SHBG, and attenuate androgen receptor activation, thus reducing the physiologic actions of testosterone, causing relative and absolute androgen deficiency.Citation46 In addition to this, activation of peroxisome proliferator activated receptor gamma initiates an imbalance in the bone resorption and bone formation process, resulting in high bone loss.Citation47 Moreover, rosiglitazone induces apoptosis of osteoblasts which reduces bone formation.Citation48
Changes in bone turnover markers
Bone turnover is assessed by measuring biomarkers such as cross linking C-terminal telopeptide of type I collagen and procollagen type 1 N-terminal propeptide. Cross linking C-terminal telopeptide of type I collagen, in addition to being a bone resorption marker, is also used to assess adherence with bisphosphonates, while procollagen type 1 N-terminal propeptide is a measure of bone formation. Higher bone turnover is not always related to decreased BMD in men.Citation49 However, in the Dubbo study, only cross linking C-terminal telopeptide of type I collagen could predict fractures.Citation50 Increased bone turnover reduces bone strength because faster bone loss increases bone formation. This sudden increase in bone formation impairs bone connectivity because a higher fraction of protein matrix undergoes partial post transcriptional modification, resulting in a malformed matrix. It is commonly observed that bone turnover markers are increased in institutionalized patientsCitation51 to a greater extent than in community-dwelling individuals. In older men, increased bone turnover markers are associated with lower areal BMD.Citation49
Secondary osteoporosis
Most men who sustain fractures do so because of multiple other factors, including age, smoking, alcohol consumption, low weight, physical/functional limitations, previous fracture, weight loss, prolonged corticosteroid use, androgen deprivation therapy, dietary calcium intake, chronic lung disease, and prostate cancer. Accumulation of kidney stones is negatively correlated with BMD.Citation52–Citation54 Recent research shows that low levels of free 25(OH) vitamin D result in bone loss.Citation55 The major mineral lost in bone loss is calcium, and calcium absorption is influenced by vitamin D. Therefore, individuals who consume calcium in low amounts and who are diagnosed with vitamin D deficiency also have an increased fracture risk.Citation56–Citation58
Osteoporosis affects men over 70 years of age. When BMD in both the trabecular and cortical bones is reduced, there is an increased risk of fractures of the hip and vertebrae, which are often fatal in men. Some patients have hypogonadism due to testicular failure or pituitary disorders, leading to bone loss.Citation59 Medications for other medical conditions, including those for cancer, diabetes, and seizures, also cause osteoporosis.Citation60 Apart from these, drugs that raise serum prolactin levels and chronic opioid use for pain control are also implicated in bone loss. Men who have fractures of the distal forearm and those who have symptomatic vertebral and hip fractures show lower BMD as well.Citation61
Nevertheless, men have the advantage of accruing a higher peak bone mass (8%–10%) compared with women.Citation62,Citation63 In addition, microarchitectural changes in the radius have been found to include higher trabecular thickness and bone volume/total volume in men compared with women.Citation64,Citation65 In the tibia, significantly higher bone volume/total volume, trabecular number, and cortical thicknessCitation65 were reported. Although trabecular thickness was also increased, this was not statistically significant. However, these data are from younger individuals aged 19 years and 20–29 years. Longitudinal studies in older men showed an age-related decrease in trabecular thickness of the radius. However, there was decreased trabecular thickness, number, and separation in the distal tibia.Citation66 Cortical porosity is increased with age in men.Citation67 Moreover, men undergo periosteal bone accretion compensating the endosteal bone loss and maintaining strength for almost a decade after women show bone fragility.Citation66–Citation70 However, men do lose bone gradually and are susceptible to fractures after the sixth decade of life.
The action of androgen on male bone may be explained by activation of the androgen receptor or estrogen receptor (α and β).Citation28 Serum estrogen and testosterone are inversely related to fracture risk in older men, while SHBG shows a positive relationship; low serum estrogen and testosterone levels coupled with high SHBG predict clinical vertebral and nonvertebral osteoporosis and hip fractures.Citation17 SHBG has been reported to increase with age and is associated with bone loss.Citation29
Orchidectomized rodents have been shown to have an increase in bone resorption markers and periosteal bone formation, and decreased bone strength, implicating the role of decreased testosterone.Citation71 Because androgens play an important role in regulation of bone formation in males, their receptors, ie, the androgen receptor and estrogen receptor, should be activated for maintenance of bone in male mice. Estrogen receptor-α and the androgen receptor were found to increase cortical radial bone growth and mediate protection of cancellous bone in males.Citation71 Moreover, androgen receptor activation is solely responsible for the development and maintenance of trabecular bone in males, and the androgen receptor and estrogen receptor-α are responsible for cortical bone mass and muscle mass.Citation72,Citation73 It is reported that estrogen receptor-α may act indirectly via the growth hormone-insulin-like growth factor-1 axis.Citation74 Therefore, there is ample evidence that an age-related reduction of hormone secretion, especially sex hormones, affects bone maintenance in men.
Osteoporosis in men is a gradual disease that progresses with age.Citation14 In the US, two million men are diagnosed with osteoporosis and another 12 million have low bone mass and are at the risk of developing the disease.Citation75 The outcome for male patients after hip fracture (30% of hip fractures occur in men) is grim. One third (32%) die within the first year of hip fracture.Citation76–Citation78 Only 21% are able to live independently in the community a year after the fracture, with 26% receiving home care and 53% living in an institution for the rest of their lives.Citation79 Unfortunately, men with osteoporosis have higher mortality rates than women, and the fracture burden also increases the problems of osteoporosis in men. In one study, men with subsequent fractures were found to have an increased mortality rate and more men were immobilized at 120 days after their fracture.Citation11
Treatment options
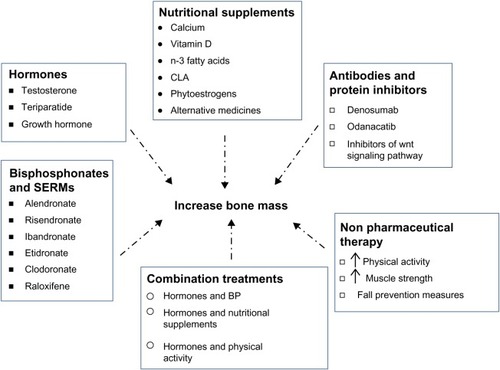
Available treatment options for men with osteoporosis are those that were developed for and are currently used in women. Many of these drugs/supplements have been very beneficial in males as well, and include hormones, bisphosphonates, antibodies, protein inhibitors, and nutritional supplements (). Pharmacologic options for treating osteoporosis in men are listed in .
Table 1 Pharmacological options available for treating osteoporosis in men
Figure 2 Treatment options for osteoporosis in men.
Hormones
Hormone therapy, especially estrogen, has been widely used to treat osteoporosis in women. Testosterone supplementation is also used in men, because a decrease in testosterone is linked to decreased bone mass. With such therapy, site-specific improvement has been reported in some cases, with benefits only at the spine and not at the hip.Citation80,Citation81 Moreover, treatment with testosterone not only increased BMDCitation82 but also increased prostate gland size and prostate specific antigen (PSA) levels. However, the prostate size is not affected when testosterone was given with finasteride (inhibitor of 5alpha reductase), therefore in these patients androgen replacement therapy was effective.Citation52 It is important to note that testosterone treatment should be given only to those who have low levels of testosterone and need agents that will prevent fractures.Citation80,Citation83
The only anabolic bone agent approved by the US Food and Drug Administration for prevention and treatment of osteoporosis is teriparatide, a truncated parathyroid hormone. It may be one option for treating osteoporosis in men because it is associated with major gains in BMD at the lumbar spine, but less at the hip.Citation4,Citation14,Citation80,Citation84–Citation86 Bone formation markers also increased with this treatment, and the risk of fracture reduced by 51%.Citation87 In patients with existing vertebral fractures, the risk went down to 13:1. However, continuous treatment with teriparatide is not recommended because of several side effects. Combination therapy using bisphosphonates and teriparatide did not increase BMD, however, patients on teriparatide therapy alone showed significantly increased BMD, in the lumbar and femur neck, although the BMT were similar in both groups (combined and teriparatide groups).Citation88 At this point in time, the Food and Drug Administration has approved the use of teriparatide only for 24 months. After cessation of teriparatide, patients show a gradual decrease in BMD unless they are put on other medications.Citation87 Although combination treatment with alendronate was not encouraging, administration of alendronate after teriparatide treatment maintained BMD, so sequential treatment is recommended.Citation86,Citation89,Citation90 Whenever treatment with teriparatide was restarted, there was an increase in BMD.Citation91
Another hormone that regulates circulating calcium is calcitonin. This hormone is a powerful inhibitor of osteoclasts. Administration of this agent is nasal, and it is reported to increase BMD at the lumbar spine and femoral neck but not at the proximal femur.Citation4,Citation14,Citation82,Citation86,Citation92,Citation93 During the last decade, calcitonin has been tested as a treatment option for osteoporosis in men.Citation92,Citation93 Growth hormone would also be beneficial to patients who are growth hormone-deficient.
Administration of hormones like testosterone, parathyroid hormone, and calcitonin may be useful for preventing bone loss and increasing bone mass. However, such treatment options should be used on an individual basis. Outcomes are dependent on the initial hormone status in some cases, while sequential treatment may be important in others.
Selective estrogen receptor modulators
Selective estrogen receptor modulators bind to estrogen receptors and have estrogen-like activity in bone. Raloxifene has been shown to increase bone mass and decrease urinary and circulating bone resorption markers.Citation94,Citation95 However, use of these agents may be limited to men with prostate cancer.
Bisphosphonates
Bisphosphonates are recommended for treating osteoporosis in men.Citation4,Citation80,Citation86 Alendronate (Fosamax®, Merck, Whitehouse Station, NJ, USA) improves BMD at the vertebrae and femoral neck in both eugonadal and hypogonadal men, with significant reductions in the incidence of vertebral fractures and less height loss.Citation14,Citation82,Citation96,Citation97 Other bisphosphonates like risendronate (Actonel®, Warner Chilcott, Dublin, Ireland) and ibandronate (Boniva®, Genentech Inc, South San Francisco, CA, USA) are also options for treating osteoporosis in men.Citation14 Intermittent etidronate (Didronel®, Warner Chilcott, Dublin, Ireland) therapy increases BMD at the lumbar spine by 3%, with smaller increases at the hip (0.7%) in patients with secondary osteoporosis.Citation82,Citation98 Ibandronate, another bisphosphonate, when given intravenously in combination with calcium and vitamin D supplementation increased BMD at the spine, femoral neck, and trochanter in a small study of 14 individuals.Citation99 In yet another study, administration of ibandronate increased BMD at the lumbar vertebrae and hip in men and significantly reduced the risk of vertebral fractures.Citation100 Zoledronate (Zometa®, Zomera®, Aclasta®, Reclast®, Novartis, Basel, Switzerland) may be an alternative (administered intravenously, which may be better than the oral route for bisphosphonates) and is shown to be as effective as other bisphosphonates.Citation14,Citation101–Citation104 Bisphosphonates have been shown to be effective therapeutic agents for patients with osteoporosis, but there are certain limitations in using them. Many patients show tolerance, and each of the oral bisphosphonates has very strict and specific guidelines for dosage. However, great strides have been made in developing drugs that can be taken daily, weekly, monthly, or even yearly.
Antibodies and protein inhibitors
A recent trend in drug development has focused on targeting important proteins involved in development of osteoporosis. Specific antibodies and inhibitors of these proteins have been developed, and are listed in . RANKL stimulates osteoclastogenesis and increases bone resorption. Denosumab, a monoclonal antibody against RANKL, is one of the newer medications that is available as a therapeutic option.Citation14,Citation94,Citation105,Citation106 It decreases bone resorption, thereby decreasing bone loss. This antibody should be taken with caution because it can affect the immune system, leading to infections.
Table 2 Biological therapy possibilities for treating osteoporosis in men
Another protein, cathepsin K, which is expressed in osteoclasts and is capable of releasing minerals from bone, has also been targeted. Odanacatib, an inhibitor of cathepsin K, decreased bone resorption markers and increased BMD at the spine and hip over two years.Citation94,Citation107 This therapy is recommended in men because it increases BMD and decreases the fracture rate in patients with prostate cancer, delays the time to the first skeletal-related event, and increases bone metastasis-free survival.Citation108
The wingless-type and integrase 1 (Wnt) signaling pathway regulates osteoblastogenesis, and inhibitors of some of these proteins can be considered as potential drug targets.Citation109 When sclerostin (a natural antagonist of the Wnt signaling pathway) is inhibited, the anabolic properties of bone are increased in animal models.Citation110 In healthy men, inhibition of sclerostin using AMG 785 significantly increased bone formation markers and BMD, while significantly decreasing bone resorption markers.Citation111 A polymorphism of the gene coding for sclerostin showed site-specific association with BMD of the femoral neck.Citation105 Dickkopf 1, another endogenous inhibitor of the Wnt signaling pathway, has also been investigated, and a Dickkopf 1 antagonist was found to increase bone formation.Citation109 Another possible target is the frizzled-related proteins, which are also inhibitors of the Wnt signaling pathway. Studies in mice have shown that overexpression of serum frizzled-related proteins decreases bone mass and inhibits osteoblast function as well as the anabolic effects of parathyroid hormone.Citation109,Citation112 Other possible targets that have been reported include glycogen synthase kinase 3 (GSK-3), another endogenous inhibitor of the Wnt signaling pathway.Citation109 Further, several inhibitors of GSK-3, including lithium, 603281-31-8, 6-bromoindirubin-3′-oxime, and AR28, have been tested.Citation109 However, a major concern in using Wnt signaling pathway antagonists is the oncogenic effects resulting from inhibition of this pathway.Citation109 Targeting specific proteins in the metabolic pathway related to bone metabolism is a novel approach, but extreme caution is needed because many of these proteins are not just part of bone metabolism but also play a key role in other important pathways. Therefore, when these drugs are used, a balanced approach that increases the benefits but decreases other health complications and side effects must be taken into consideration. This approach is very important in treating osteoporosis, mainly because a majority of the patients are elderly, moreover, with increase in life expectancy the quality of life should also be improved.
Nutritional supplementation
Several nutritional supplements are also implicated in maintaining bone health. These include minerals like calcium, vitamins, fatty acids, and herbal products (). Nutritional supplementation with calcium and vitamin D to increase calcium absorption is commonly prescribed to patients with osteoporosis, including men.Citation4,Citation97,Citation113–Citation117 Calcium and vitamin D monotherapy has been reported to reduce hip fractures.Citation14,Citation80,Citation118,Citation119 It is reported that community-dwelling elders are likely to have suffcient intake of calcium and vitamin D, but institutionalized elders showed calcium and vitamin D deficiency. Intermittent monofluorophosphate and calcium increased bone density and decreased the risk of vertebral fractures in upper middle aged men (mean age 53).Citation120 Irrespective of ethnic background, vitamin D supplementation is recommended.Citation16 Supplementation with calcium and vitamin D, in addition to helping bone, decreases hyperthyroidism and improves muscle strength, function, and balance.Citation56–Citation58
Table 3 Possible nutritional supplements for the prevention and treatment of osteoporosis in men
Other nutritional supplements that have shown promise in reducing bone loss are n-3 fatty acids, conjugated linoleic acid, soy isoflavones, and some herbal compounds. Several studies of n-3 fatty acids have reported benefits on bones in male animal models by decreasing prostaglandin 2Citation121,Citation122 and bone resorption as well as increasing BMD at the lumbar vertebraeCitation123 and tibia.Citation124 n-3 fatty acids benefit bone mainly by reducing bone turnover.Citation125 In men, a positive correlation has been found between consumption of docosahexaenoic acid and peak BMD.Citation126 Another fatty acid, known as conjugated linoleic acid and commonly found in milk and dairy products, increased bone mass in male mice.Citation127 Phytoestrogens like soy isoflavones increased bone mass in orchidectomized rats, primarily by increasing bone turnover markers and the microarchitecture of trabecular bone.Citation128 Ipriflavone, a synthetic isofavone, is also beneficial in maintaining bone mass.Citation116
Herbal supplements and alternative medicines, including vitamin E, black cohosh, red clover, Fructus linguistri lucidi, Cissus quadrangularis, and prunes, have shown to have bone-protective properties in preclinical studies.Citation116,Citation129–Citation131 Although many of these studies have been conducted in females, there is a high probability that these will also be beneficial to men. More systematic studies using these promising compounds may be worth pursuing to develop safer and more cost-effective treatment options.
Apart from drug interventions, nonpharmacologic therapies () including exercise and muscle-strengthening strategies are also recommended, eg, increasing physical activity in patients with osteoporosis.Citation80 Fall prevention measures such as checking vision and hearing, neurologic assessment, and installing safety features in the home should be part of the treatment regimen.Citation132,Citation133 In addition, leading a healthy lifestyle, including eating healthy foods, avoiding tobacco, and limiting alcohol consumption is also recommended.Citation133
Table 4 Nonpharmacologic therapies available for men
Conclusion
Traditionally, osteoporosis was considered a disease that affects only women. However, a little over two decades ago, osteoporosis came to be recognized as a disease that is also prevalent in elderly men and with bleak survival outcomes following fracture. As the population is moving toward an increased life span, it is logical to predict that the number of patients with osteoporosis will increase. In individuals suffering from osteoporosis, living conditions are highly compromised, apart from the financial burden on society.
Although we have learned a lot about osteoporosis from studies in women, there are basic differences between women and men which need to be addressed, hence a need for more studies in men. In particular, assessment must include standards determined for men followed by treatment options. Evidence from existing studies shows most men do not get treated for osteoporosis after a hip fracture. Patients should be screened during initial evaluation for serum calcium, phosphorus, creatine, alkaline phosphatase, vitamin D, liver transaminases, thyroid-stimulating hormone, total testosterone, 25-hydroxyvitamin D, parathyroid hormone, prostate-specific antigen, bone turnover markers (ie, terminal telopeptide and procollagen type 1 amino-terminal propeptide), glucocorticoid use, and family history in order to decide on the correct treatment options.Citation4,Citation88,Citation106 Currently there are very few clinical studies on osteoporosis in men, limiting the understanding and development of the disease as well as the therapeutic options.Citation134 Dual X-ray absorptiometry, high resolution quantitated computed tomography with finite element analysis, and magnetic resonance imaging are common methods for detection of the disease.Citation62,Citation94 Use of these diagnostic tools in men after a certain age will help in identifying those at risk so that preventive measures to avoid fractures can be implemented. Moreover, the focus in identifying new drugs for preventing and treating osteoporosis should also include reducing or eliminating harmful side effects and be more cost-effective.
Acknowledgments
The author thanks Jorge F Navarro and Mahaboob MH Khan for their assistance in literature collection for this review.
Disclosure
The author has no conflicts of interest to report in this work.
References
- Hannan MT Felson DT Dawson-Hughes B Risk factors for longitudinal bone loss in elderly men and women: the Framingham Osteoporosis Study J Bone Miner Res 2000 15 4 710 720 10780863
- Khosla S Update in male osteoporosis J Clin Endocrinol Metab 2010 95 1 3 10 20056806
- Melton LJ3rd Chrischilles EA Cooper C Lane AW Riggs BL Perspective. How many women have osteoporosis? J Bone Miner Res 1992 7 9 1005 1010 1414493
- Binkley N A perspective on male osteoporosis Best Pract Res Clin Rheumatol 2009 23 6 755 768 19945687
- Edelstein OE What do Israeli osteoporotic men know and do about their disease? J Osteoporos 2011 2011 719862 21772976
- McLeod KM Johnson CS A systematic review of osteoporosis health beliefs in adult men and women J Osteoporos 2011 2011 197454 21941678
- Solimeo SL Living with a ‘women’s disease’: risk appraisal and management among men with osteoporosis J Mens health 2011 8 3 185 191 22125585
- Madeo B Zirilli L Caffagni G The osteoporotic male: overlooked and undermanaged? Clin Interv Aging 2007 2 3 305 312 18044181
- Rao SS Budhwar N Ashfaque A Osteoporosis in men Am Fam Physician 2010 82 5 503 508 20822086
- Seeman E Reduced bone formation and increased bone resorption: rational targets for the treatment of osteoporosis Osteoporos Int 2003 14 Suppl 3 S2 S8 12730770
- Lambert JK Zaidi M Mechanick JI Male osteoporosis: epidemiology and the pathogenesis of aging bones Curr Osteoporos Rep 2011 9 4 229 236 21853294
- Compston J Cooper A Cooper C Guidelines for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK Maturitas 2009 62 2 105 108 19135323
- National Osteoporosis Foundation Making a diagnosis Available from: http://www.nof.org/articles/8 Accessed October 16, 2012
- Gates BJ Das S Management of osteoporosis in elderly men Maturitas 2011 69 2 113 119 21481552
- Ryan CS Petkov VI Adler RA Osteoporosis in men: the value of laboratory testing Osteoporos Int 2010 22 6 1845 1853 20936403
- Dawson-Hughes B Racial/ethnic considerations in making recommendations for vitamin D for adult and elderly men and women Am J Clin Nutr 2004 80 Suppl 6 1763S 1766S 15585802
- Leder BZ LeBlanc KM Schoenfeld DA Eastell R Finkelstein JS Differential effects of androgens and estrogens on bone turnover in normal men J Clin Endocrinol Metab 2003 88 1 204 210 12519853
- Mohr BA Guay AT O’Donnell AB McKinlay JB Normal, bound and nonbound testosterone levels in normally ageing men: results from the Massachusetts Male Ageing Study Clin Endocrinol (Oxf) 2005 62 1 64 73 15638872
- Feldman HA Longcope C Derby CA Age trends in the level of serum testosterone and other hormones in middle-aged men: longitudinal results from the Massachusetts Male Aging Study J Clin Endocrinol Metab 2002 87 2 589 598 11836290
- Morley JE Kaiser FE Perry HM3rd Longitudinal changes in testosterone, luteinizing hormone, and follicle-stimulating hormone in healthy older men Metabolism 1997 46 4 410 413 9109845
- Muller M den Tonkelaar I Thijssen JH Grobbee DE van der Schouw YT Endogenous sex hormones in men aged 40–80 years Eur J Endocrinol 2003 149 6 583 589 14641001
- Svartberg J Midtby M Bonaa KH Sundsfjord J Joakimsen RM Jorde R The associations of age, lifestyle factors and chronic disease with testosterone in men: the Tromso Study Eur J Endocrinol 2003 149 2 145 152 12887292
- Vermeulen A Kaufman JM Giagulli VA Influence of some biological indexes on sex hormone-binding globulin and androgen levels in aging or obese males J Clin Endocrinol Metab 1996 81 5 1821 1826 8626841
- Ferrini RL Barrett-Connor E Sex hormones and age: a cross-sectional study of testosterone and estradiol and their bioavailable fractions in community-dwelling men Am J Epidemiol 1998 147 8 750 754 9554416
- Litman HJ Bhasin S Link CL Araujo AB McKinlay JB Serum androgen levels in black, Hispanic, and white men J Clin Endocrinol Metab 2006 91 11 4326 4334 16912139
- Yeap BB Testosterone and ill-health in aging men Nat Clin Pract Endocrinol Metab 2009 5 2 113 121 19165223
- Khosla S Amin S Orwoll E Osteoporosis in men Endocr Rev 2008 29 4 441 464 18451258
- Sinnesael M Boonen S Claessens F Gielen E Vanderschueren D Testosterone and the male skeleton: a dual mode of action J Osteoporos 2011 2011 240328 21941679
- LeBlanc ES Nielson CM Marshall LM The effects of serum testosterone, estradiol, and sex hormone binding globulin levels on fracture risk in older men J Clin Endocrinol Metab 2009 94 9 3337 3346 19584177
- Kurland ES Cosman F McMahon DJ Rosen CJ Lindsay R Bilezikian JP Parathyroid hormone as a therapy for idiopathic osteoporosis in men: effects on bone mineral density and bone markers J Clin Endocrinol Metab 2000 85 9 3069 3076 10999788
- Van Pottelbergh I Goemaere S Zmierczak H Kaufman JM Perturbed sex steroid status in men with idiopathic osteoporosis and their sons J Clin Endocrinol Metab 2004 89 10 4949 4953 15472190
- Trouvin AP Goeb V Receptor activator of nuclear factor-kappaB ligand and osteoprotegerin: maintaining the balance to prevent bone loss Clin Interv Aging 2011 5 345 354 21228900
- Israeli RS Ryan CW Jung LL Managing bone loss in men with locally advanced prostate cancer receiving androgen deprivation therapy J Urol 2008 179 2 414 423 18076933
- Liu H Paige NM Goldzweig CL Screening for osteoporosis in men: a systematic review for an American College of Physicians guideline Ann Intern Med 2008 148 9 685 701 18458282
- Lopez AM Pena MA Hernandez R Val F Martin B Riancho JA Fracture risk in patients with prostate cancer on androgen deprivation therapy Osteoporos Int 2005 16 6 707 711 15714259
- Shahinian VB Kuo YF Freeman JL Goodwin JS Risk of fracture after androgen deprivation for prostate cancer N Engl J Med 2005 352 2 154 164 15647578
- Diamond TH Higano CS Smith MR Guise TA Singer FR Osteoporosis in men with prostate carcinoma receiving androgen-deprivation therapy: recommendations for diagnosis and therapies Cancer 2004 100 5 892 899 14983482
- Daniell HW Dunn SR Ferguson DW Lomas G Niazi Z Stratte PT Progressive osteoporosis during androgen deprivation therapy for prostate cancer J Urol 2000 163 1 181 186 10604342
- Kiratli BJ Srinivas S Perkash I Terris MK Progressive decrease in bone density over 10 years of androgen deprivation therapy in patients with prostate cancer Urology 2001 57 1 127 132 11164157
- Sardone LD Renlund R Willett TL Fantus IG Grynpas MD Effect of rosiglitazone on bone quality in a rat model of insulin resistance and osteoporosis Diabetes 2011 60 12 3271 3278 21998400
- Debiais F Thiazolidinediones: antidiabetic agents with effects on bone Joint Bone Spine 2009 76 3 221 223 19362505
- Grey A Thiazolidinedione-induced skeletal fragility – mechanisms and implications Diabetes Obes Metab 2009 11 4 275 284 18671797
- Rosen CJ The rosiglitazone story – lessons from an FDA Advisory Committee meeting N Engl J Med 2007 357 9 844 846 17687124
- Aubert RE Herrera V Chen W Haffner SM Pendergrass M Rosiglitazone and pioglitazone increase fracture risk in women and men with type 2 diabetes Diabetes Obes Metab 2010 12 8 716 721 20590749
- Chakreeyarat S Saetung S Chailurkit LO Elevated vitamin D status in postmenopausal women on thiazolidinediones for type 2 diabetes Endocrine 2010 39 3 278 282 21069575
- Carruthers M Trinick TR Jankowska E Traish AM Are the adverse effects of glitazones linked to induced testosterone deficiency? Cardiovasc Diabetol 2008 7 30 18922158
- Lecka-Czernik B Bone loss in diabetes: use of antidiabetic thiazolidinediones and secondary osteoporosis Curr Osteoporos Rep 2010 8 4 178 184 20809203
- Soroceanu MA Miao D Bai XY Su H Goltzman D Karaplis AC Rosiglitazone impacts negatively on bone by promoting osteoblast/osteocyte apoptosis J Endocrinol 2004 183 1 203 216 15525588
- Szulc P Biochemical bone turnover markers and osteoporosis in older men: where are we? J Osteoporos 2011 2011 704015 22220284
- Meier C Nguyen TV Center JR Seibel MJ Eisman JA Bone resorption and osteoporotic fractures in elderly men: the Dubbo Osteoporosis Epidemiology study J Bone Miner Res 2005 20 4 579 587 15765176
- Theiler R Stahelin HB Kranzlin M Tyndall A Bischoff HA High bone turnover in the elderly Arch Phys Med Rehabil 1999 80 5 485 489 10326908
- Adler RA Epidemiology and pathophysiology of osteoporosis in men Curr Osteoporos Rep 2006 4 3 110 115 16908000
- Herrara AL-EA Mateo J Gil J Ibarz E Garcia L Male osteoporosis: a review World J Orthop 2012 3 12 223 234 23362466
- Shimizu Y Sakai A Menuki K Reduced bone formation in alcohol-induced osteopenia is associated with elevated p21 expression in bone marrow cells in aldehyde dehydrogenase 2-disrupted mice Bone 2011 48 5 1075 1086 21256255
- Al-oanzi ZH Tuck SP Raj N Assessment of vitamin D status in male osteoporosis Clin Chem 2006 52 2 248 254 16339300
- Bischoff-Ferrari HA Conzelmann M Stahelin HB Is fall prevention by vitamin D mediated by a change in postural or dynamic balance? Osteoporos Int 2006 17 5 656 663 16508700
- Gielen E Boonen S Vanderschueren D Calcium and vitamin D supplementation in men J Osteoporos 2011 2011 875249 21876835
- Gupta R Sharma U Gupta N Effect of cholecalciferol and calcium supplementation on muscle strength and energy metabolism in vitamin D-deficient Asian Indians: a randomized, controlled trial Clin Endocrinol (Oxf) 2010 73 4 445 451 20455886
- Behre HM Kliesch S Leifke E Link TM Nieschlag E Long-term effect of testosterone therapy on bone mineral density in hypogonadal men J Clin Endocrinol Metab 1997 82 8 2386 2390 9253305
- Farhat G Yamout B Mikati MA Demirjian S Sawaya R El-Hajj Fuleihan G Effect of antiepileptic drugs on bone density in ambulatory patients Neurology 2002 58 9 1348 1353 12011279
- Scane AC Francis RM Sutcliffe AM Francis MJ Rawlings DJ Chapple CL Case-control study of the pathogenesis and sequelae of symptomatic vertebral fractures in men Osteoporos Int 1999 9 1 91 97 10367034
- Amin S Khosla S Sex- and age-related differences in bone microarchitecture in men relative to women assessed by high-resolution peripheral quantitative computed tomography J Osteoporos 2012 2012 129760 22496983
- Gennari L Bilezikian JP Osteoporosis in men: pathophysiology and treatment Curr Rheumatol Rep 2007 9 1 71 77 17437671
- Khosla S Riggs BL Atkinson EJ Effects of sex and age on bone microstructure at the ultradistal radius: a population-based noninvasive in vivo assessment J Bone Miner Res 2006 21 1 124 131 16355281
- Sode M Burghardt AJ Kazakia GJ Link TM Majumdar S Regional variations of gender-specific and age-related differences in trabecular bone structure of the distal radius and tibia Bone 2010 46 6 1652 1660 20188877
- Macdonald HM Nishiyama KK Kang J Hanley DA Boyd SK Age-related patterns of trabecular and cortical bone loss differ between sexes and skeletal sites: a population-based HR-pQCT study J Bone Miner Res 2010 26 1 50 62 20593413
- Burghardt AJ Kazakia GJ Ramachandran S Link TM Majumdar S Age- and gender-related differences in the geometric properties and biomechanical significance of intracortical porosity in the distal radius and tibia J Bone Miner Res 2009 25 5 983 993 19888900
- Russo CR Lauretani F Seeman E Structural adaptations to bone loss in aging men and women Bone 2006 38 1 112 118 16242391
- Seeman E During aging, men lose less bone than women because they gain more periosteal bone, not because they resorb less endosteal bone Calcif Tissue Int 2001 69 4 205 208 11730251
- Seeman E The structural and biomechanical basis of the gain and loss of bone strength in women and men Endocrinol Metab Clin North Am 2003 32 1 25 38 12699291
- Vanderschueren D Vandenput L Boonen S Lindberg MK Bouillon R Ohlsson C Androgens and bone Endocr Rev 2004 25 3 389 425 15180950
- Callewaert F Venken K Ophoff J Differential regulation of bone and body composition in male mice with combined inactivation of androgen and estrogen receptor-alpha FASEB J 2009 23 1 232 240 18809737
- Sims NA Dupont S Krust A Deletion of estrogen receptors reveals a regulatory role for estrogen receptors-beta in bone remodeling in females but not in males Bone 2002 30 1 18 25 11792560
- Olson LE Ohlsson C Mohan S The role of GH/IGF-I-mediated mechanisms in sex differences in cortical bone size in mice Calcif Tissue Int 2010 88 1 1 8 21113585
- National Osteoporosis Foundation Just for men Available from: http://www.nof.org/articles/236 Accessed October 15, 2012
- Bass E French DD Bradham DD Rubenstein LZ Risk-adjusted mortality rates of elderly veterans with hip fractures Ann Epidemiol 2007 17 7 514 519 17420142
- Cooper C Campion G Melton LJ3rd Hip fractures in the elderly: a world-wide projection Osteoporos Int 1992 2 6 285 289 1421796
- Johnell O Kanis JA An estimate of the worldwide prevalence and disability associated with osteoporotic fractures Osteoporos Int 2006 17 12 1726 1733 16983459
- Poor G Atkinson EJ Lewallen DG O’Fallon WM Melton LJ3rd Age-related hip fractures in men: clinical spectrum and short-term outcomes Osteoporos Int 1995 5 6 419 426 8695962
- Duque G Troen BR Understanding the mechanisms of senile osteoporosis: new facts for a major geriatric syndrome J Am Geriatr Soc 2008 56 5 935 941 18454751
- Snyder PJ Peachey H Hannoush P Effect of testosterone treatment on bone mineral density in men over 65 years of age J Clin Endocrinol Metab 1999 84 6 1966 1972 10372695
- Licata A Osteoporosis in men: suspect secondary disease first Cleve Clin J Med 2003 70 3 247 254 12678216
- Kanis JA Bianchi G Bilezikian JP Towards a diagnostic and therapeutic consensus in male osteoporosis Osteoporos Int 2011 22 11 2789 2798 21509585
- Gruenewald DA Matsumoto AM Testosterone supplementation therapy for older men: potential benefits and risks J Am Geriatr Soc 2003 51 1 101 115 12534854
- Cusano NE Costa AG Silva BC Bilezikian JP Therapy of osteoporosis in men with teriparatide J Osteoporos 2011 2011 463675 22132345
- Girotra M Rubin MR Bilezikian JP Anabolic skeletal therapy for osteoporosis Arq Bras Endocrinol Metabol 2006 50 4 745 754 17117299
- Kaufman JM Orwoll E Goemaere S Teriparatide effects on vertebral fractures and bone mineral density in men with osteoporosis: treatment and discontinuation of therapy Osteoporos Int 2005 16 5 510 516 15322742
- Finkelstein JS Leder BZ Burnett SM Effects of teriparatide, alendronate, or both on bone turnover in osteoporotic men J Clin Endocrinol Metab 2006 91 8 2882 2887 16684825
- Kurland ES Heller SL Diamond B McMahon DJ Cosman F Bilezikian JP The importance of bisphosphonate therapy in maintaining bone mass in men after therapy with teriparatide [human parathyroid hormone(1–34)] Osteoporos Int 2004 15 12 992 997 15175844
- Kraenzlin ME Meier C Parathyroid hormone analogues in the treatment of osteoporosis Nat Rev Endocrinol 2011 7 11 647 656 21750510
- Finkelstein JS Hayes A Hunzelman JL Wyland JJ Lee H Neer RM The effects of parathyroid hormone, alendronate, or both in men with osteoporosis N Engl J Med 2003 349 13 1216 1226 14500805
- Toth E Csupor E Meszaros S The effect of intranasal salmon calcitonin therapy on bone mineral density in idiopathic male osteoporosis without vertebral fractures – an open label study Bone 2005 36 1 47 51 15664001
- Trovas GP Lyritis GP Galanos A Raptou P Constantelou E A randomized trial of nasal spray salmon calcitonin in men with idiopathic osteoporosis: effects on bone mineral density and bone markers J Bone Miner Res 2002 17 3 521 527 11874243
- Honig S Osteoporosis – new treatments and updates Bull NYU Hosp Jt Dis 2010 68 3 166 170 20969546
- Smith MR Fallon MA Lee H Finkelstein JS Raloxifene to prevent gonadotropin-releasing hormone agonist-induced bone loss in men with prostate cancer: a randomized controlled trial J Clin Endocrinol Metab 2004 89 8 3841 3846 15292315
- Gonnelli S Cepollaro C Montagnani A Alendronate treatment in men with primary osteoporosis: a three-year longitudinal study Calcif Tissue Int 2003 73 2 133 139 14565594
- Orwoll ES Oviatt SK McClung MR Deftos LJ Sexton G The rate of bone mineral loss in normal men and the effects of calcium and cholecalciferol supplementation Ann Intern Med 1990 112 1 29 34 2152844
- Anderson FH Francis RM Bishop JC Rawlings DJ Effect of intermittent cyclical disodium etidronate therapy on bone mineral density in men with vertebral fractures Age Ageing 1997 26 5 359 365 9351480
- Lamy O Sandini L Pache I Fatio S Burnand J Burckhardt P Intravenous ibandronate in men with osteoporosis: an open pilot study over 2 years J Endocrinol Invest 2003 26 8 728 732 14669826
- Boonen S Reginster JY Kaufman JM Fracture risk and zoledronic acid therapy in men with osteoporosis N Engl J Med 2012 367 18 1714 1723 23113482
- Piper PKJr Gruntmanis U Management of osteoporosis in the aging male: focus on zoledronic acid Clin Interv Aging 2009 4 289 303 19750231
- Sewerynek E Stuss M The role of I.V. ibandronate administration in osteoporosis therapy Endokrynol Pol 2011 62 1 51 60 21365580
- Black DM Delmas PD Eastell R Once-yearly zoledronic acid for treatment of postmenopausal osteoporosis N Engl J Med 2007 356 18 1809 1822 17476007
- Black DM Reid IR Boonen S The effect of 3 versus 6 years of zoledronic acid treatment of osteoporosis: a randomized extension to the HORIZON-Pivotal Fracture Trial (PFT) J Bone Miner Res 2012 27 2 243 254 22161728
- Piters E de Freitas F Nielsen TL Andersen M Brixen K Van Hul W Association study of polymorphisms in the SOST gene region and parameters of bone strength and body composition in both young and elderly men: data from the Odense Androgen Study Calcif Tissue Int 2011 90 1 30 39 22076526
- Kaufman JM Reginster JY Boonen S Treatment of osteoporosis in men Bone 2012 53 1 134 144 23201268
- Gagnon C Ebeling PR Recent advances in managing osteoporosis F1000 Med Rep 2009 1 pii 96
- Morgans AK Smith MR RANKL-targeted therapies: the next frontier in the treatment of male osteoporosis J Osteoporos 2011 2011 941310 22013547
- Baron R Hesse E Update on bone anabolics in osteoporosis treatment: rationale, current status, and perspectives J Clin Endocrinol Metab 2012 97 2 311 325 22238383
- Li X Ominsky MS Warmington KS Sclerostin antibody treatment increases bone formation, bone mass, and bone strength in a rat model of postmenopausal osteoporosis J Bone Miner Res 2009 24 4 578 588 19049336
- Lewiecki EM Sclerostin: a novel target for intervention in the treatment of osteoporosis Discov Med 2011 12 65 263 273 22031665
- Cho HY Choi HJ Sun HJ Transgenic mice overexpressing secreted frizzled-related proteins (sFRP)4 under the control of serum amyloid P promoter exhibit low bone mass but did not result in disturbed phosphate homeostasis Bone 2010 47 2 263 271 20472109
- Dawson-Hughes B Harris SS Krall EA Dallal GE Effect of calcium and vitamin D supplementation on bone density in men and women 65 years of age or older N Engl J Med 1997 337 10 670 676 9278463
- Trivedi DP Doll R Khaw KT Effect of four monthly oral vitamin D3 (cholecalciferol) supplementation on fractures and mortality in men and women living in the community: randomised double blind controlled trial BMJ 2003 326 7387 469 12609940
- Compston J Clinical and therapeutic aspects of osteoporosis Eur J Radiol 2009 71 3 388 391 19660883
- Moyad MA Complementary/alternative therapies for reducing hot fashes in prostate cancer patients: reevaluating the existing indirect data from studies of breast cancer and postmenopausal women Urology 2002 59 4 Suppl 1 20 33 11937433
- Avenell A Gillespie WJ Gillespie LD O’Connell D Vitamin D and vitamin D analogues for preventing fractures associated with involutional and post-menopausal osteoporosis Cochrane Database Syst Rev 2009 2 CD000227 19370554
- Boonen S Lips P Bouillon R Bischoff-Ferrari HA Vanderschueren D Haentjens P Need for additional calcium to reduce the risk of hip fracture with vitamin d supplementation: evidence from a comparative metaanalysis of randomized controlled trials J Clin Endocrinol Metab 2007 92 4 1415 1423 17264183
- Tang BM Eslick GD Nowson C Smith C Bensoussan A Use of calcium or calcium in combination with vitamin D supplementation to prevent fractures and bone loss in people aged 50 years and older: a meta-analysis Lancet 2007 370 9588 657 666 17720017
- Ringe JD Dorst A Kipshoven C Rovati LC Setnikar I Avoidance of vertebral fractures in men with idiopathic osteoporosis by a three year therapy with calcium and low-dose intermittent monofluorophosphate Osteoporos Int 1998 8 1 47 52 9692077
- Watkins BA Li Y Lippman HE Seifert MF Omega-3 polyunsaturated fatty acids and skeletal health Exp Biol Med (Maywood) 2001 226 6 485 497 11395919
- Fernandes G Bhattacharya A Rahman M Zaman K Banu J Effects of n-3 fatty acids on autoimmunity and osteoporosis Front Biosci 2008 13 4015 4020 18508495
- Weiler HA Dietary supplementation of arachidonic acid is associated with higher whole body weight and bone mineral density in growing pigs Pediatr Res 2000 47 5 692 697 10813598
- Weiler HA Fitzpatrick-Wong SC Modulation of essential (n-6):(n-3) fatty acid ratios alters fatty acid status but not bone mass in piglets J Nutr 2002 132 9 2667 2672 12221227
- Shen CL Yeh JK Rasty J Improvement of bone quality in gonad-intact middle-aged male rats by long-chain n-3 polyunsaturated fatty acid Calcif Tissue Int 2007 80 4 286 293 17406770
- Hogstrom M Nordstrom P Nordstrom A n-3 Fatty acids are positively associated with peak bone mineral density and bone accrual in healthy men: the NO2 Study Am J Clin Nutr 2007 85 3 803 807 17344503
- Banu J Bhattacharya A Rahman M O’Shea M Fernandes G Effects of conjugated linoleic acid and exercise on bone mass in young male Balb/C mice Lipids Health Dis 2006 5 7 16556311
- Soung DY Devareddy L Khalil DA Soy affects trabecular microarchitecture and favorably alters select bone-specific gene expressions in a male rat model of osteoporosis Calcif Tissue Int 2006 78 6 385 391 16830200
- Banu J Varela E Fernandes G Alternative therapies for the prevention and treatment of osteoporosis Nutr Rev 2012 70 1 22 40 22221214
- Chai SC Hooshmand S Saadat RL Payton ME Brummel-Smith K Arjmandi BH Daily apple versus dried plum: impact on cardiovascular disease risk factors in postmenopausal women J Acad Nutr Diet 2012 112 8 1158 1168 22818725
- Hooshmand S Chai SC Saadat RL Payton ME Brummel-Smith K Arjmandi BH Comparative effects of dried plum and dried apple on bone in postmenopausal women Br J Nutr 2011 106 6 923 930 21736808
- Kondo KL Osteoporotic vertebral compression fractures and vertebral augmentation Semin Intervent Radiol 2008 25 4 413 424 21326583
- Levine JP Pharmacologic and nonpharmacologic management of osteoporosis Clin Cornerstone 2006 8 1 40 53 17591575
- Schwarz P Jorgensen NR Mosekilde L Vestergaard P The evidence for efficacy of osteoporosis treatment in men with primary osteoporosis: a systematic review and meta-analysis of antiresorptive and anabolic treatment in men J Osteoporos 2011 2011 259818 21776371