Abstract
Decreasing levels of estrogens during menopause are associated with reduced bone density and an increased risk of osteoporosis. Many women also experience bothersome vasomotor and vaginal symptoms during the menopausal transition. Results of systematic reviews and meta-analyses of randomized controlled trials have shown that both systemic estrogen therapy or hormone therapy (estrogen combined with a progestin) are useful to prevent bone loss, and they are the most effective treatment for such climacteric symptoms as hot flushes, sweating, vaginal dryness, and dyspareunia. Unfortunately, estrogen therapy and hormone therapy increase the risk of endometrial and breast cancer, respectively. The selective estrogen receptor modulators (SERMs) result in positive estrogenic effects on bone, with no negative effects on the endometrium and breast but do not provide relief from postmenopausal symptoms. The combination of a SERM with estrogen as a tissue selective estrogen complex (TSEC) is a new strategy for the prevention of bone loss and the treatment of climacteric symptoms. This combination is particularly interesting from a clinical point of view, taking into account that estrogen alone did not increase breast cancer risk by the Women’s Health Initiative. TSEC is hypothesized to provide the benefits of estrogen-alone therapy, with an improved tolerability profile because the SERM component can make possible the elimination of progestin. The objective of this review was to critically evaluate the evidence from the reports published to date on the use of bazedoxifene (a third-generation SERM) in combination with conjugated estrogens in postmenopausal women. The conclusion is that effectively, the combination of bazedoxifene and conjugated estrogens may be a promising alternative to hormone therapy for the prevention of osteoporosis and the treatment of postmenopausal symptoms in non-hysterectomized postmenopausal women.
Introduction
Notable is the increased risk of osteoporosis, cardiovascular disease, and vasomotor instability observed in women, subsequent to the cessation of ovarian estrogen production that occurs at menopause.Citation1,Citation2 Climacteric symptoms, such as hot flushes (HFs) or sweating, and vulvar and vaginal atrophy (VVA) are common complaints in postmenopausal women.Citation3–Citation6 Bone loss, although asymptomatic, can be relevant, especially in their early postmenopausal years.Citation7,Citation8 It is not surprising, therefore, that estrogen therapy (ET) (estrogen alone) or hormone therapy (HT) (estrogen combined with a progestin) are among the most effective therapies for the treatment and prevention of osteoporosis.Citation9 Both regimens normalize bone remodeling and, unlike other antiresorptive therapies, such as bisphosphonates, their use is not associated with increased risk of atypical femoral fractures or osteonecrosis of the jaw.Citation10–Citation12 However, while the beneficial effects of ET/HT in bone are unquestioned, the increased risk of breast cancer, cardiovascular disease, and dementia observed in elderly women participating in the Women’s’ Health Initiative (WHI) study, have resulted in a dramatic decrease in the use of estrogen treatment in the climacteric patient and in postmenopausal women at high risk for osteoporosis.Citation13,Citation14
Regardless, it is clear that the estrogen receptor (ER) and its signaling pathways are extremely useful targets in bone, and it is anticipated that compounds that modulate this axis, and exhibit a more favorable therapeutic index, will have considerable clinical utility. The selective estrogen receptor modulators (SERMs), a class of compounds whose relative ER-agonist/antagonist activity can differ between target organs, are a first step in this direction. An “ideal” SERM would act as an ER agonist by having a protective effect on bone and improving lipid parameters, while also acting as an ER antagonist by maintaining breast and endometrial safety.Citation15 In this way, the treatment could result in positive estrogenic effects on bone and lipid metabolism, with no negative effects on the endometrium and breast.
SERMs are useful for the prevention and treatment of postmenopausal osteoporosis, but unfortunately, they do not provide relief from climacteric symptoms.Citation16,Citation17
A new strategy is the combination of a SERM with estrogen(s), described as a tissue selective estrogen complex (TSEC), based on the simultaneous but differential effects of each compound on estrogen receptor activity.Citation18–Citation24
In this review, we critically evaluate the evidence from the reports published to date on the use of bazedoxifene (BZA) (a third-generation SERM) in combination with conjugated estrogens (CE) in postmenopausal women. PubMed was searched from inception to February 2013, using the key words bazedoxifene and conjugated estrogens.
Bazedoxifene (bazedoxifene acetate)
BZA is a novel SERM developed for the prevention and treatment of postmenopausal osteoporosis. It is a new molecule with unique structural characteristics compared with raloxifene and tamoxifen, two other compounds referred to as SERMs.Citation20 Its molecule was developed based on the raloxifene model, replacing the benzothiophene core with an indole ring.Citation20,Citation25 BZA can interact with ERs alpha and beta in bone, breast, uterus, blood vessels, and liver; the binding affinity is slightly greater for ER-alpha versus ER-beta. The average half-life is 28 hours and maximum concentration is reached in 1–2 hours after oral administration; it is mainly excreted by feces (84.7%), while renal excretion is negligible.Citation26,Citation27 The main metabolic pathway is glucurono-conjugation; its metabolism is poorly mediated by cytochrome P450, and as a consequence, BZA has a low risk of pharmacological interactions.Citation27
In animal models, BZA treatment was shown to maintain or increase bone mineral density (BMD), preserve normal histological bone quality, improve bone compressive strength, and reduce total cholesterol levels.Citation28 The evidence shown in the animal model has also been confirmed in the human. In fact, in a Phase II, randomized, double-blind, controlled study of healthy postmenopausal women, BZA (up to 40 mg daily dose) did not stimulate the endometrium, nor increase the incidence of breast pain and induced a significant reduction in markers of bone remodeling.Citation29–Citation31
Clinically, BZA has been evaluated in two global, randomized, double-blind, placebo- and active-controlled, Phase III studies: an osteoporosis prevention study and an osteoporosis treatment study.Citation32,Citation33
The osteoporosis prevention study was a large 24-month, randomized, double-blind clinical trial involving 1,434 healthy postmenopausal women (mean age, 58 years; mean time from last menstrual period, 11 years) with a BMD T-score at the lumbar spine or femoral neck between −1.0 and −2.5 or clinical risk factors for osteoporosis. This study compared the efficacy and safety of three doses of daily BZA (10, 20, or 40 mg) with placebo and raloxifene (60 mg daily) in the prevention of postmenopausal osteoporosis.Citation32 All doses of BZA and raloxifene prevented lumbar and femoral bone loss, while in the placebo group, a significant loss in BMD was found. All active groups showed significant differences in comparison with the placebo group (P < 0.001), in terms of BMD changes. A significant decrease in osteocalcin and C-telopeptide plasma levels versus the baseline and placebo group level was observed in all active-treatment groups, from the third month of observation and throughout the study (P < 0.001). The study showed that the treatment with BZA prevented the postmenopausal bone loss and reduced bone turnover markers (BTM) equally as well as raloxifene and was generally well tolerated, without stimulating the endometrium.Citation34
The osteoporosis treatment study was a registrative international, multicenter, double-blind, randomized, placebo- and active-controlled Phase III trial conducted at 206 sites worldwide. It was performed to evaluate the safety and efficacy of BZA in treating postmenopausal women with osteoporosis.Citation33 This trial used an active comparator (raloxifene), in addition to placebo and involved 7,492 women (55–85 years of age) with radiographically confirmed vertebral fractures (about 56% of study population) or with lumbar spine or femoral neck BMD T-scores between −2.5 and −4.0. The primary endpoint was the incidence of new radiographically confirmed vertebral fractures after 3 years.Citation33 Secondary endpoints included incidence of nonvertebral fractures, changes from baseline in BMD of the lumbar spine and total hip, and changes in biochemical markers of bone resorption and bone formation. In the intent-to-treat analysis, the incidence of new vertebral fractures was significantly lower (P < 0.05) in all active-treatment groups versus the placebo group, with relative risk reductions of 42%, 37%, and 42%, respectively in patients treated with BZA 20 mg, BZA 40 mg, and raloxifene 60 mg.Citation33 No significant differences were found in the incidence of nonvertebral osteoporosis-related fractures among treatment groups, but in a post hoc analysis of a subgroup of women (n = 1,772) at higher risk of fracture (femoral neck T-score <−3.0 and/or more than one moderate or severe vertebral fracture or multiple mild vertebral fractures), BZA 20 mg showed a 50% and 44% reduction in nonvertebral fracture risk relative to placebo (P < 0.02) and raloxifene 60 mg (P < 0.05) respectively. When the data for both BZA treatment groups were combined, the incidence of nonvertebral fractures was 40% lower compared with placebo (P = 0.03).Citation33 The osteoporosis treatment study also confirmed positive data on the surrogate markers of fracture’s risk: BMD and the BTMs.Citation33
Further data from subsequent 5-year (4,216 women) and 7-year (1,732 women) extensions of the 3-year study have confirmed anti-fracture efficacy at the vertebral level with BZA 20 mg/day, with a relative risk reduction of 30% in comparison with placebo (P < 0.022).Citation35,Citation36
BZA was generally well tolerated, both in the osteoporosis prevention and treatment study: the overall incidence of adverse events, serious adverse events, and adverse events leading to treatment interruption, in the BZA-treated groups was not different from placebo.Citation32,Citation33 Nevertheless, in the prevention study, the incidence of HFs in the BZA groups (20%–24%) and the raloxifene group (19%) was higher than that in the placebo group (14%) (overall P < 0.05).Citation32 Also during the osteoporosis treatment study, the incidence of HFs and leg cramps was similar among the bazedoxifene and raloxifene treatment groups (12.6% vs 12.0% and 10.9% vs 11.7%, respectively), but significantly higher than that reported with placebo (6.3% and 8.2%, respectively).Citation33 However, another study evaluated BZA’s role in inducing HFs in postmenopausal women, in comparison with placebo, during a 12-weeks period of observation; results showed that BZA did not increase the incidence, number, or intensity of hot flushes compared with placebo, in postmenopausal women not suffering from this symptom before the start of administration.Citation37 The incidence of venous thromboembolism (VTE) was greater with BZA 20 mg/day compared with placebo, however low in absolute terms (BZA 20 mg/day: 2.8 cases per 1,000 women-year; placebo: 1.7 cases per 1,000 women-year).Citation32,Citation33
Bazedoxifene/conjugated estrogens
Rationale
The known antimitotic activity of BZA in the uterus and endometrium offers the possibility to associate this SERM to an estrogen, in the form of a CE, to form an association currently called a TSEC, so as to control menopausal syndrome (hot flushes, sweating, vaginal dryness, bone loss, etc) in postmenopausal women.Citation21,Citation22 In this way, a SERM, like BZA, can protect the endometrium from the proliferative action exerted by an estrogen, and this fact allows us to use estrogen without progestin in postmenopausal women, taking into account that estrogen alone does not increase breast cancer risk in postmenopausal women, as demonstrated in the estrogen-only arm of the WHI.Citation38 Moreover the association of BZA with CE might protect the skeleton from bone loss, in postmenopausal women.
Preclinical studies
Preclinical studies have shown different responses to various SERMs when combined with CE.
In ovariectomized rats, BZA/CE increased BMD and volume, without alterations in bone histology.Citation22 Moreover, animal studies have shown different responses of estrogen tissues to various SERMs when combined with CE. BZA was the most potent SERM in inhibiting CE-induced increases in uterine wet weight, and the mammary gland stimulation in response to CE was inhibited to the greatest extent with BZA versus raloxifene or lasofoxifene.Citation23
Clinical studies
The Phase II clinical trial of BZA/CE included 412 healthy postmenopausal women; the findings were that several doses of BZA/CE diminished the frequency and severity of hot flushes and reduced bone resorption, without stimulation of the endometrium or breast.Citation39
The results from four Phase III studies, known as the Selective estrogens, Menopause, And Response to Therapy (SMART) trials, were recently reported in several publications.Citation40–Citation46 The design of the SMART trials, including participant inclusion criteria, is summarized in .
Table 1 Study design of the randomized, double-blind, placebo-controlled SMART trials in postmenopausal womenCitation40–Citation46
Safety and tolerability were also reported for each of the SMART trials.Citation41,Citation42,Citation44–Citation46
Effects on BMD and BTMs
The efficacy of BZA/CE in preventing bone loss was evaluated by changes in BMD, as measured by dual-energy X-ray absorptiometry; changes in BTMs, as surrogate markers of bone formation and bone resorption, were also assessed. Although there has been some variability associated with BTMs measurement, these markers are widely used to evaluate bone metabolism and treatment response to bone-active therapies.
BMD
In both sub-studies of the SMART-1study, an increase in BMD at the lumbar spine, from baseline to 12 and 24 months, was observed in postmenopausal women treated with BZA/CE; this was significantly different (P < 0.001) from the decrease in BMD observed with placebo.Citation43 The adjusted annual percent changes in lumbar spine BMD from baseline in women >5 years postmenopause are shown in . The BMD increases seen in women taking higher BZA doses (combined with CE) were smaller than those in women taking lower BZA doses, probably based on the simultaneous but differential effects of each compound on estrogen receptor activity.
Figure 1 Adjusted annual percent changes in lumbar spine BMD from baseline, in women >5 years postmenopause randomly assigned to one of eight treatment groups in the SMART-1 trial.Citation43
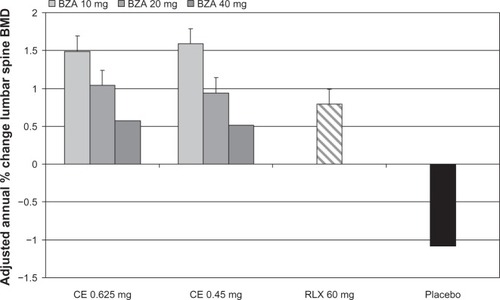
However, compared with raloxifene, mean changes in BMD in the lumbar spine at month 24 were significantly greater for all BZA/CE doses, except for 40 mg BZA, in women 1 to 5 years postmenopause, which was similar to raloxifene.Citation43
Similar significant results for total hip BMD were also observed for all BZA/CE doses versus placebo (P < 0.01) at months 12 and 24 in both groups of women.Citation43 Generally, mean percentage increases in BMD at 12 and 24 months were also significant (P < 0.05) compared with placebo, at the femoral subregions (intertrochanteric, neck, and trochanteric regions), for all BZA/CE doses.Citation43
Significant differences in total hip BMD between BZA/CE and raloxifene were only seen for BZA/CE doses containing 10 mg BZA, in both substudy populations.Citation43
BTMs
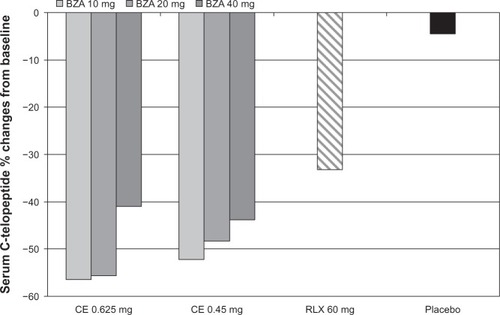
The median percentage changes from baseline in the BTMs osteocalcin and C-telopeptide were also significantly greater with all BZA/CE doses versus placebo (P < 0.001) and most with BZA/CE doses versus raloxifene (P < 0.05) ().Citation43
Figure 2 Median percent changes in serum C-telopeptide at 12 months from baseline for women between 1 and 5 years postmenopause, in the SMART-1study.Citation43
Effects on estrogen deficiency symptoms
Postmenopausal women may experience a variety of symptoms associated with a decline in the level of estrogens. Vasomotor symptoms, such as HFs, are reported by 60%–85% of women during menopause. Symptoms of VVA (vaginal dryness, irritation, soreness, or dyspareunia, and increases in urinary frequency, urgency, or incontinence) are reported by 50% of postmenopausal women.
HFs
The efficacy of BZA/CE on vasomotor symptoms was evaluated by measuring the frequency and severity of HFs in response to treatment.
In the SMART-1 study, HFs were evaluated in 261 women with at least seven moderate-to-severe HFs per day or 50 per week.Citation41 Compared with placebo, all BZA/CE doses significantly reduced the daily number of HFs at most time points and HF severity at week 12, except for BZA/CE doses containing BZA 40 mg.Citation41
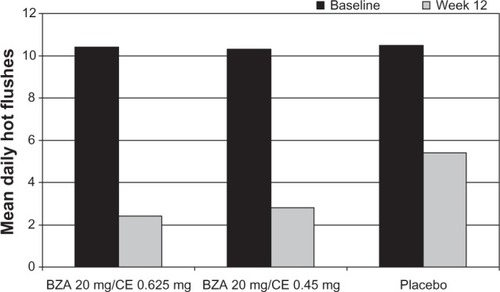
The SMART-2 study examined HFs as a primary endpoint.Citation44 At weeks 4 and 12, women taking BZA/CE had significant reductions from baseline in the mean daily number and severity of moderate-to-severe HFs compared with placebo.Citation44 The number of HFs was reduced by 74% and 80% with BZA 20 mg/CE 0.45 and 0.625 mg, respectively, versus 51% with placebo ().Citation44 Significant decreases in HF frequency and severity with both BZA/CE doses compared with placebo were seen as early as week 2 or 3.Citation41,Citation44
Figure 3 The mean daily number of moderate-to-severe hot flushes at 12 weeks vs baseline in healthy postmenopausal women randomized to BZA 20 mg/CE 0.625, BZA 20 mg/CE 0.45 mg, or placebo in the SMART-2 trial.Citation44
VVA
Changes in the proportion of vaginal superficial, parabasal, and intermediate cells improved, showing increased numbers of superficial cells (an estrogen-like effect on the vaginal surface) in women using BZA 10 or 20 mg/CE 0.625 or 0.45 mg in the SMART-1 trial.Citation41 VVA was also assessed using four coprimary endpoints, in 664 postmenopausal women taking BZA 20 mg/CE 0.45 mg, BZA 20 mg/CE 0.625 mg, BZA 20 mg, or placebo, in the SMART-3 trial.Citation45 Similar results were reported at week 12 with both BZA/CE doses compared with placebo and BZA alone. Superficial cell increases with CE 0.625 mg alone have previously been reported, by approximately 20% after about 1 year of observation.Citation47 Even if direct comparison between these studies cannot be made based on time-point differences, the increase was approximately 6% with BZA 20 mg/CE 0.625 mg at 12 weeks.Citation45
It is known that low estrogen levels induce a reduction in the glycogen content of the vaginal epithelium, which leads to inhibition of lactic acid production in the vagina and an increase in vaginal pH. Vaginal pH changes significantly improved with BZA 20 mg/CE 0.625 mg versus placebo and for both BZA/CE doses versus BZA alone.
About 70% of women with vaginal dryness and dyspareunia do not voluntarily mention this symptom to their general practitioner, even though they suffer from decreased quality of life as a result of these conditions. Improvements in the severity of the most bothersome VVA symptoms (vaginal dryness for example) were found for BZA 20 mg/CE 0.625 mg compared with placebo and for both BZA/CE doses compared with BZA alone.
Sleep, quality of life, satisfaction
Sleep disruptions, including increased time to fall asleep, nighttime awakenings, and daytime tiredness are common among postmenopausal women. Moreover, during menopause, many women experience bothersome symptoms, such as mood disturbances or sexual dysfunction, which may negatively impact quality of life.
Significant improvements, from the SMART trials, in terms of sleep, quality of life, and satisfaction in women treated with BZA/CE compared with placebo, are summarized in .Citation48–Citation51
Table 2 Significant improvements from SMART trials, in terms of sleep, quality of life, and satisfaction, in women treated with BZA/CE compared with placeboCitation48–Citation51
In the SMART-1 trial, women treated with BZA 20 mg/CE 0.45 and 0.625 mg had significant reductions in mean number of minutes to fall asleep, increases in mean minutes slept, and increases in quality of sleep score compared with placebo.Citation48
In the SMART-2 trial, BZA 20 mg/CE 0.45 and 0.625 mg significantly improved time to fall asleep, sleep disturbance, sleep adequacy, and overall sleep problems compared with placebo (P < 0.001 for all), as assessed on the Medical Outcomes Study sleep scale.Citation49
In the SMART-1 trial, BZA 20 mg/CE 0.45 and 0.625 mg significantly improved total and vasomotor function Menopause-specific Quality Of Life (MENQOL) scores compared with placebo (P < 0.001).Citation50 Similar results were observed in the SMART-2 trial.Citation49,Citation50
In the SMART-3 trial, women treated with BZA 20 mg/CE 0.45 and 0.625 mg reported significant improvements in ease of lubrication on the Arizona Sexual Experiences scale compared with placebo. Moreover, BZA 20 mg/CE 0.45 and 0.625 mg were associated with significant improvements from baseline in the total, vasomotor, and sexual function scores compared with placebo (P < 0.001 for all).Citation51
In the SMART-2 trial, the Menopause Symptoms Treatment Satisfaction Questionnaire results showed that 73.5% of women treated with BZA 20 mg/CE 0.45 mg and 78.2% of women treated with BZA 20 mg/CE 0.625 mg were satisfied with treatment compared with 44.4% of women given placebo (P < 0.001).Citation49 Similar results were observed in the SMART-3 trial.Citation51
Safety
In all the SMART trials, the overall incidence of adverse events (AEs) was similar between women in the BZA/CE and placebo groups, without significant difference in the number of patients discontinuing because of AEs.Citation41,Citation44,Citation45
In the SMART-1 trial, the largest and longest SMART trial, the incidence of VTE or cardiovascular events was low and similar for women treated with BZA/CE or placebo.Citation41 No VTEs were reported in the SMART-2 or SMART-3 trials, but these studies were of 12-week duration.Citation44,Citation45
However, the SMART trials were not powered to determine between-group differences in VTE or cardiovascular events.
In terms of laboratory findings, it is known that women may experience adverse changes in metabolic profile during the menopausal transition, including increases in total cholesterol, triglycerides, low-density lipoprotein (LDL) cholesterol, and decreases in high-density lipoprotein (HDL) cholesterol.Citation52 The long-term effects of BZA/CE on lipid parameters were evaluated in the SMART-1 trial.Citation41 At Month 24, BZA 20 mg/CE 0.45 and 0.625 mg were associated with decreases from baseline in total cholesterol (for BZA 20 mg/CE 0.45 mg versus placebo [P < 0.05]) and LDL cholesterol (for both doses vs placebo [P < 0.01]). HDL cholesterol increased from baseline vs placebo (P < 0.01) with BZA 20 mg/CE 0.45 and 0.625 mg, as did triglycerides (P < 0.01). These effects on serum lipids and lipoproteins are similar to that described with CE, but not with transdermal estrogen administration.Citation53 Changes in coagulation factors, such as increases in levels of the coagulation protein factor VII and fibrinogen, have been shown to occur during the menopausal transition.Citation52 Significant decreases from baseline in levels of fibrinogen, protein S activity, and antithrombin III activity were reported for BZA 20 mg/CE in the SMART-1 trial.Citation41
After 12 months of therapy, no endometrial hyperplasia was observed for BZA 20 or 40 mg/CE 0.45 mg, BZA 40 mg/CE 0.625 mg, raloxifene, or placebo, and this did not increase after 24 months.Citation40 To the contrary, the 10 mg BZA dose did not prevent the estrogen dose-dependent endometrial hyperplasia when coupled with CE 0.45 or 0.625 mg.Citation40
A low incidence of bleeding or spotting was also seen in women using BZA 20 or 40 mg/CE 0.625 or 0.45 mg and was statistically similar to the results with placebo. In the recent SMART-4 study, BZA 20 mg/CE 0.45 and 0.625 mg significantly improved BMD while maintaining endometrial safety and showed a favorable safety/tolerability profile over 1 year.Citation46
No significant differences in the occurrence of breast pain were found between BZA/CE, raloxifene, or placebo groups at any time interval.Citation41,Citation44,Citation45
Conclusion
The results of systematic reviews and meta-analyses of randomized, controlled trials have shown that both systemic ET and HT are useful to prevent bone loss, and they are the most effective treatment for such climacteric symptoms as hot flushes, sweating, vaginal dryness, and dyspareunia. In women who have such symptoms, this treatment results in a 75% reduction in frequency and an 87% reduction in severity of the symptoms, relative to treatment with a placebo.Citation54 Unfortunately, ET and HT increase the risk of endometrial and breast cancer, respectively.Citation55,Citation56
BZA is a third-generation SERM that was developed on the raloxifene model, replacing its benzothiophene core with an indole ring. The results of Phase III studies of postmenopausal women at risk of osteoporosis (prevention study)Citation32 and with osteoporosis (treatment study)Citation33 demonstrate the efficacy of BZA in the prevention of postmenopausal bone loss and of vertebral fractures. Nevertheless, an increased incidence of HFs is common with SERMs administration, even if BZA did not increase HFs in comparison with placebo in postmenopausal women not suffering from this symptom at baseline.Citation37
This comprehensive review reports the clinical outcomes of randomized, double-blind, placebo-controlled Phase III trials using BZA/CE in postmenopausal women, supporting its use as a new menopausal therapy. BZA/CE therapy in postmenopausal women reduced the frequency and severity of HFs, improved symptoms of VVA, and prevented the loss of bone mass independently of years since menopause. Women taking various doses of BZA/CE might maintain or gain bone mass similarly to women taking currently approved CE/medroxyprogesterone acetate therapies.Citation57 The increase in BMD with BZA/CE previously shown was due to the decrease in bone remodeling, as demonstrated by the significant decrease in serum BTMs, for all BZA/CE doses compared with the placebo group. Furthermore, serum levels of C-telopeptide for women treated with BZA/CE were reduced to the levels of premenopausal women.Citation58 Reductions in BTMs are regarded as valid surrogate endpoints for anti-fracture efficacy. A relationship between reductions in BTMs and fracture incidence has also been reported: as BTMs decrease, fracture incidence decreases. A reduction of 30% in BTMs is sufficient to cause a significant decrease in vertebral fracture risk; the decrease has to be over 50% to have an effect on nonvertebral fracture incidence linked to effects on cortical bone, less responsive to treatment.Citation59–Citation61 The combination of 20 mg of BZA with 0.625 mg of CE achieves these results.
It was observed that adding incrementally higher doses of BZA to CE slightly diminished the effects of CE on BMD, BTMs, and HFs. Also, the data on endometrial safety show that doses containing 20 mg BZA have the most appropriate profile for postmenopausal women. Adding BZA to CE provides an alternative treatment for postmenopausal women that protects the endometrium, without the addition of a progestin. However despite current studies showing no increased risk for endometrial hyperplasia, breast cancer, or thromboembolic events, further studies evaluating a greater number of women for longer study periods will be needed to more accurately assess the risk for such AEs in women using such combination therapy.
In conclusion, BZA/CE may be a valid alternative to HT for the treatment of postmenopausal symptoms and prevention of osteoporosis in non-hysterectomized postmenopausal women. Thereby, the treatment target will not only be the osteoporosis, but also the whole menopausal syndrome. The results of the WHI study led to a drastic reduction of the use of ET and hormone replacement therapy for the prevention of osteoporosis, since the risk of breast and endometrial cancer seemed to outweigh the benefits. The combination of BZA/CE might extend the pharmacological prevention of osteoporosis to younger postmenopausal women for the lack of oncological risks and the symptomatic improvements. Therefore, this combination might improve the adherence to osteoporosis treatment in the clinical practice, often compromised by lack of motivation or safety concerns.Citation62
Disclosure
The authors declare no conflict of interests in this work.
References
- Chahal HS Drake WM The endocrine system and ageing J Pathol 2007 211 2 173 180 17200939
- Vagenakis AG Endocrine aspects of menopause Clin Rheumatol 1989 8 Suppl 2 48 51 2667871
- Rödström K Bengtsson C Lissner L Milsom I Sundh V Björkelund C A longitudinal study of the treatment of hot flushes: the population study of women in Gothenburg during a quarter of a century Menopause 2002 9 3 156 161 11973438
- Feldman BM Voda A Gronseth E The prevalence of hot flash and associated variables among perimenopausal women Res Nurs Health 1985 8 3 261 268 3852361
- Versi E Harvey MA Cardozo L Brincat M Studd JW Urogenital prolapse and atrophy at menopause: a prevalence study Int Urogynecol J Pelvic Floor Dysfunct 2001 12 2 107 110 11374507
- Haines CJ Xing SM Park KH Holinka CF Ausmanas MK Prevalence of menopausal symptoms in different ethnic groups of Asian women and responsiveness to therapy with three doses of conjugated estrogens/medroxyprogesterone acetate: the Pan-Asia Menopause (PAM) study Maturitas 2005 52 3–4 264 276 15921865
- Bjarnason NH Alexandersen P Christiansen C Number of years since menopause: spontaneous bone loss is dependent but response to hormone replacement therapy is independent Bone 2002 30 4 637 642 11934658
- Nilas L Christiansen C The pathophysiology of peri- and postmenopausal bone loss Br J Obstet Gynaecol 1989 96 5 580 587 2503028
- Cauley JA Seeley DG Ensrud K Ettinger B Black D Cummings SR Estrogen replacement therapy and fractures in older women. Study of Osteoporotic Fractures Research Group Ann Intern Med 1995 122 1 9 16 7985914
- Khosla S Update on estrogens and the skeleton J Clin Endocrinol Metab 2010 95 8 3569 3577 20685883
- Marx RE Pamidronate (Aredia) and zoledronate (Zometa) induced avascular necrosis of the jaws: a growing epidemic J Oral Maxillofac Surg 2003 61 9 1115 1117 12966493
- Park-Wyllie LY Mamdani MM Juurlink DN Bisphosphonate use and the risk of subtrochanteric or femoral shaft fractures in older women JAMA 2011 305 8 783 789 21343577
- Parente L Uyehara C Larsen W Whitcomb B Farley J Long-term impact of the women’s health initiative on HRT Arch Gynecol Obstet 2008 277 3 219 224 17713777
- Rossouw JE Anderson GL Prentice RL Writing Group for the Women’s Health Initiative Investigators Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results From the Women’s Health Initiative randomized controlled trial JAMA 2002 288 3 321 333 12117397
- Komm BS Lyttle CR Developing a SERM: stringent preclinical selection criteria leading to an acceptable candidate (WAY-140424) for clinical evaluation Ann N Y Acad Sci 2001 949 317 326 11795370
- Evista® (raloxifene hydrochloride) tablet [prescribing information] Indianapolis Eli Lilly and Company 2007
- Taylor HS Designing the ideal selective estrogen receptor modulator – an achievable goal? Menopause 2009 16 3 609 615 19182697
- Komm BS A new approach to menopausal therapy: the tissue selective estrogen complex Reprod Sci 2008 15 10 984 992 19088368
- Deroo BJ Korach KS Estrogen receptors and human disease J Clin Invest 2006 116 3 561 570 16511588
- Komm BS Kharode YP Bodine PV Harris HA Miller CP Lyttle CR Bazedoxifene acetate: a selective estrogen receptor modulator with improved selectivity Endocrinology 2005 146 9 3999 4008 15961563
- Crabtree JS Peano BJ Zhang X Komm BS Winneker RC Harris HA Activity of three selective estrogen receptor modulators on hormone-dependent responses in the mouse uterus and mammary gland Mol Cell Endocrinol 2008 287 1–2 40 46 18367319
- Kharode Y Bodine PV Miller CP Lyttle CR Komm BS The pairing of a selective estrogen receptor modulator, bazedoxifene, with conjugated estrogens as a new paradigm for the treatment of menopausal symptoms and osteoporosis prevention Endocrinology 2008 149 12 6084 6091 18703623
- Peano BJ Crabtree JS Komm BS Winneker RC Harris HA Effects of various selective estrogen receptor modulators with or without conjugated estrogens on mouse mammary gland Endocrinology 2009 150 4 1897 1903 19022889
- Hall JM McDonnell DP Coregulators in nuclear estrogen receptor action: from concept to therapeutic targeting Mol Interv 2005 5 6 343 357 16394250
- Gruber C Gruber D Bazedoxifene (Wyeth) Curr Opin Investig Drugs 2004 5 10 1086 1093
- Chandrasekaran A Ermer J McKeand W Bazedoxifene acetate metabolic disposition in healthy, postmenopausal women Clinical Pharmacology and Therapeutics 2003 73 47
- Chandrasekaran A McKeand WE Sullivan P DeMaio W Stoltz R Scatina J Metabolic disposition of [14C]bazedoxifene in healthy postmenopausal women Drug Metab Dispos 2009 37 6 1219 1225 19273530
- Miller CP Collini MD Tran BD Design, synthesis, and preclinical characterization of novel, highly selective indole estrogens J Med Chem 2001 44 11 1654 1657 11356100
- Ronkin S Northington R Baracat E Endometrial effects of bazedoxifene acetate, a novel selective estrogen receptor modulator, in postmenopausal women Obstet Gynecol 2005 6 105 1397 1404 15932835
- Boudes P Ronkin S Korner P Effects of bazedoxifene TSE-424, a novel tissue selective estrogen receptor modulator SERM, on the incidence of breast pain [abstract] Osteoporos Int 2003 14 Suppl 7 S14
- Ronkin S Baracat E Roma L TSE-424, a novel tissue selective estrogen, reduces biochemical indices of bone metabolism in a dose related fashion Presented at: Endocrine Society 83rd Annual Meeting June 20–23, 2001 Denver, CO
- Miller PD Chines AA Christiansen C Effects of bazedoxifene on BMD and bone turnover in postmenopausal women: 2-yr results of a randomized, double-blind, placebo-, and active-controlled study J Bone Miner Res 2008 23 4 525 535 18072873
- Silverman SL Christiansen C Genant HK Efficacy of bazedoxifene in reducing new vertebral fracture risk in postmenopausal women with osteoporosis: results from a 3-year, randomized, placebo-, and active-controlled clinical trial J Bone Miner Res 2008 23 12 1923 1934 18665787
- Pinkerton JV Archer DF Utian WH Bazedoxifene effects on the reproductive tract in postmenopausal women at risk for osteoporosis Menopause 2009 16 6 1102 1108 19546825
- Silverman SL Chines AA Kendler DL Bazedoxifene Study Group Sustained efficacy and safety of bazedoxifene in preventing fractures in postmenopausal women with osteoporosis: results of a 5-year, randomized, placebo-controlled study Osteoporos Int 2012 23 1 351 363 21779819
- Palacios S Silverman S Levine AB Long-term efficacy and safety of bazedoxifene in postmenopausal women with osteoporosis: results of a 7-year, randomized, placebo-controlled study [abstract] Climacteric 2011 14 Suppl 1 59 60
- Bachmann G Crosby U Feldman RA Ronkin S Constantine GD Effects of bazedoxifene in nonflushing postmenopausal women: a randomized phase 2 trial Menopause 2011 18 5 508 514 21289525
- Anderson GL Limacher M Assaf AR Women’s Health Initiative Steering Committee Effects of conjugated equine estrogen in postmenopausal women with hysterectomy: the Women’s Health Initiative randomized controlled trial JAMA 2004 291 14 1701 1712 15082697
- Pickar JH Tissue selective estrogen complex: a new paradigm for menopausal therapy Menopausal Med 2008 16 1 S10 S13
- Pickar JH Yeh IT Bachmann G Speroff L Endometrial effects of a tissue selective estrogen complex containing bazedoxifene/conjugated estrogens as a menopausal therapy Fertil Steril 2009 92 3 1018 1024 19635613
- Lobo RA Pinkerton JV Gass MLS Evaluation of bazedoxifene/conjugated estrogens for the treatment of menopausal symptoms and effects on metabolic bone parameters and overall safety profile Fertil Steril 2009 92 3 1025 1038 19635615
- Archer DF Lewis V Carr BR Olivier S Pickar JH Bazedoxifene/conjugated estrogens (BZA/CE): incidence of uterine bleeding in postmenopausal women Fertil Steril 2009 92 3 1039 1044 19635614
- Lindsay R Gallagher JC Kagan R Pickar JH Constantine G Efficacy of tissue-selective estrogen complex of bazedoxifene/conjugated estrogens for osteoporosis prevention in at-risk postmenopausal women Fertil Steril 2009 92 3 1045 1052 19635616
- Pinkerton JV Utian WH Constantine GD Olivier S Pickar JH Relief of vasomotor symptoms with the tissue-selective estrogen complex containing bazedoxifene/conjugated estrogens: a randomized, controlled trial Menopause 2009 16 6 1116 1124 19546826
- Kagan R Williams RS Pan K Mirkin S Pickar JH A randomized, placebo- and active-controlled trial of bazedoxifene/conjugated estrogens for treatment of moderate to severe vulvar/vaginal atrophy in postmenopausal women Menopause 2010 17 2 281 289 19779382
- Mirkin S Komm BS Pan K Chines AA Effects of bazedoxifene/conjugated estrogens on endometrial safety and bone in postmenopausal women Climacteric 2013 16 3 338 346 23038989
- Utian WH Shoupe D Bachmann G Pinkerton JV Pickar JH Relief of vasomotor symptoms and vaginal atrophy with lower doses of conjugated equine estrogens and medroxyprogesterone acetate Fertil Steril 2001 75 6 1065 1079 11384629
- Pinkerton JV Chines AA Racketa J Mirkin S Bazedoxifene/conjugated estrogens (BZA/CE): effect on sleep parameters in postmenopausal women [abstract] Menopause 2010 17 6 1237 1238
- Utian W Yu H Bobula J Mirkin S Olivier S Pickar JH Bazedoxifene/conjugated estrogens and quality of life in postmenopausal women Maturitas 2009 63 4 329 335 19647382
- Pinkerton JV Chines AA Racketa J Mirkin S Menopause-related quality of life and satisfaction in postmenopausal women treated with bazedoxifene/conjugated estrogens (BZA/CE) [abstract] Menopause 2010 17 6 1219
- Bachmann G Bobula J Mirkin S Effects of bazedoxifene/conjugated estrogens on quality of life in postmenopausal women with symptoms of vulvar/vaginal atrophy Climacteric 2010 13 2 132 140 19863455
- Spencer CP Godsland IF Stevenson JC Is there a menopausal metabolic syndrome? Gynecol Endocrinol 1997 11 5 341 355 9385535
- Adami S Rossini M Zamberlan N Bertoldo F Dorizzi R Lo Cascio V Long-term effects of transdermal and oral estrogens on serum lipids and lipoproteins in postmenopausal women Maturitas 1993 17 3 191 196 8133793
- Maclennan AH Broadbent JL Lester S Moore V Oral oestrogen and combined oestrogen/progestogen therapy versus placebo for hot flushes Cochrane Database Syst Rev 2004 4 CD002978 15495039
- Smith DC Prentice R Thompson DJ Hermann WL Association of exogenous estrogen and endometrial carcinoma N Engl J Med 1975 293 23 1164 1167 1186789
- Anderson GL Chlebowski RT Rossouw JE Prior hormone therapy and breast cancer risk in the Women’s Health Initiative randomized trial of estrogen plus progestin Maturitas 2006 55 2 103 115 16815651
- Lindsay R Gallagher JC Kleerekoper M Pickar JH Effect of lower doses of conjugated equine estrogens with and without medroxyprogesterone acetate on bone in early postmenopausal women JAMA 2002 287 20 2668 2676 12020302
- Adami S Bianchi G Brandi ML BONTURNO study group Determinants of bone turnover markers in healthy premenopausal women Calcif Tissue Int 2008 82 5 341 347 18470550
- Bauer DC Black DM Garnero P Fracture Intervention Trial Study Group Change in bone turnover and hip, non-spine, and vertebral fracture in alendronate-treated women: the fracture intervention trial J Bone Miner Res 2004 19 8 1250 1258 15231011
- Eastell R Barton I Hannon RA Chines A Garnero P Delmas PD Relationship of early changes in bone resorption to the reduction in fracture risk with risedronate J Bone Miner Res 2003 18 6 1051 1056 12817758
- Rossini M Orsolini G Adami S Kunnathully V Gatti D Osteoporosis treatment: why ibandronic acid? Expert Opin Pharmacother 2013 14 10 1371 1381 23650954
- Rossini M Bianchi G Di Munno O Treatment of Osteoporosis in clinical Practice (TOP) Study Group Determinants of adherence to osteoporosis treatment in clinical practice Osteoporos Int 2006 17 6 914 921 16538553