
Abstract
Pulmonary arterial hypertension (PAH) is a complex and incurable disease for which pulmonary vasodilators remain the core therapy. Of the three primary pathways that vasodilators target, the prostacyclin pathway was the earliest to be used and currently has the largest number of modalities for drug delivery. Inhaled treprostinil has been introduced as a treatment option in PAH and, more recently, pulmonary hypertension (PH) due to interstitial lung disease (PH-ILD), and the earlier nebulized form has been joined by a dry powder form allowing for more convenient use. In this review, we discuss inhaled treprostinil, focusing on the dry powder inhalation (DPI) formulation, and explore its dosing, applications, and evidence to support patient tolerance and acceptance. Recent trials underpinning the evidence for use of inhaled treprostinil and the most recent developments concerning the drug are discussed. Finally, the review looks briefly into premarket formulations of inhaled treprostinil and relevant early studies suggesting efficacy in PAH treatment.
Introduction
Pulmonary hypertension (PH) is a disease whose core feature is elevated pressure in the pulmonary arteries. Though a variety of tools are used to evaluate and monitor the disease, the gold standard for diagnosis of PH remains right heart catheterization. The thresholds for making the diagnosis of PH were recently changed by the 6th World Symposium on pulmonary Hypertension, which revised the criteria for precapillary PH to a mean pulmonary arterial pressure (mPAP) of >20 mmHg with a pulmonary vascular resistance of 2 Wood units or greater.Citation1
The evaluation of management of PH hinges on the etiology of the elevation in pulmonary pressures. PH is classified according to the World Health Organization (WHO) Groups, which include WHO Group I, pulmonary arterial hypertension (PAH); WHO Group II, pulmonary hypertension related to left heart disease; WHO Group III, pulmonary hypertension related to chronic lung disease; WHO Group IV, pulmonary hypertension as a result of pulmonary obstructions (chronic thromboembolic pulmonary hypertension, CTEPH), and WHO Group V, pulmonary hypertension due to multifactorial mechanisms.Citation1 For the purposes of this review, we will limit our focus to the two WHO Groups for which data exists to support the therapeutic use of prostacyclins, namely pulmonary arterial hypertension (WHO Group I, PAH) and PH due to interstitial lung disease (WHO Group III, PH-ILD).
PAH is a complex, incurable, and heterogenous disease. The hallmark of PAH is a relentless increase in pulmonary vascular resistance which, left untreated, progresses to right ventricular failure and death. Endothelial injury resulting from environmental and/or genetic insults triggers a process of constitutive proliferation of the endothelial and smooth muscle cells forming the walls of the pulmonary arteries, producing medial hypertrophy and intimal fibrosis.Citation2 Multiple overlapping pathways contribute to this insidious process, including chronic inflammation, oxidative damage, derangements in metabolic pathways, and resistance to apoptosis. Compensatory hypertrophic changes occur in the right ventricle to minimize wall stress and maintain cardiac output in the face of high pulmonary vascular resistance. With progression of PAH, these changes become maladaptive, with the right ventricle becoming increasingly hypertrophied and fibrotic, eventually developing dilatation, tricuspid regurgitation, and both systolic and diastolic dysfunction.Citation3,Citation4
While the pathophysiological changes described in PH due to interstitial lung disease share some overlap with those of PAH, the mechanisms are distinct and remain poorly understood. The processes of parenchymal and vascular destruction through fibrosis and chronic hypoxic pulmonary vasoconstriction are now known to be accompanied by concurrent endothelial changes and chronic remodeling analogous to that seen in PAH.Citation5 Genetic and molecular factors appear to have considerable influence over these vascular changes, which may occur semi-independently from the underlying lung disease process, which may allow for further research to phenotype which patients with lung disease are likely to benefit from pulmonary vasodilator therapy. As we will discuss further, unlike PAH, only one therapy has been rigorously shown to be effective in treating PH-ILD.
Pulmonary arterial vasodilators are the core therapy for management of PAH. Calcium channel blockers, once a core part of the PAH armamentarium, are now used in a limited fashion in a small subset of PAH patients with relatively mild disease and a robust hemodynamic response on vasoreactivity testing on right heart catheterization. Furthermore, patients on calcium channel blockers require careful early monitoring for hemodynamic deterioration.Citation6 Outside of PAH, riociguat carries an FDA indication as a treatment option for patients with CTEPH (WHO Group IV) who are ineligible for surgery or who had persistent PH despite surgery. Outside of Group I and Group IV PH, studies of pulmonary vasodilators have long been disappointing, with multiple unsuccessful studies and several even showing trends towards harm. Routine use of vasodilators in these patients is not recommended, though highly symptomatic patients and/or those with PH out of proportion to their underlying contributory diseases should be referred to expert centers for management. The introduction of pulmonary vasodilator therapy for Group III PH related to ILD in the form of inhaled treprostinil is a relatively recent and important development established by the publication of the INCREASE trial, which is discussed in further detail below.Citation7
Though numerous drugs acting on a variety of disparate pathways are in active development or approaching market approval, the FDA-approved therapies for PAH at the time of this writing act on three established pathways: nitric oxide, endothelin, and prostacyclin. The prostacyclin pathway is the oldest of the three, and contains the widest variety of delivery pathways, including subcutaneous, intravenous, oral, and inhaled delivery.Citation8
Background of Prostacyclin Therapy in PAH
Prostacyclin was first discovered in 1976 by Moncada et al, and multiple derivatives of the molecule still in use today were developed in the next few years, including epoprostenol, iloprost, and treprostinil.Citation9 Use of exogenous prostacyclin analogs aims to replicate the potent vasodilatory and platelet inhibiting effects of endogenous prostaglandins.Citation10 Prostacyclins act on the IP receptor, a G protein-coupled receptor that increases intracellular cyclic adenosine monophosphate (cAMP) levels through adenylate cyclase, producing downstream vasodilatory effects in pulmonary arterial smooth muscle cells (PASMCs).Citation9 Small registries established beneficial symptomatic and hemodynamic effects of prostacyclin use from the early 1980s onward, culminating in the 1982 randomized study by Rubin et al demonstrating a 32 meter six-minute walk distance improvement and markedly improved mortality in the group assigned to intravenous epoprostenol.Citation11 Epoprostenol was approved by the FDA in 1995 and licensed in Europe the following year, the first specific pulmonary vasodilator to be approved.Citation12
Intravenous epoprostenol, while efficacious, requires cumbersome intravenous delivery and has a very short half-life due to its intrinsic instability at room temperature, resulting in potentially lethal consequences in the case of any stoppage in drug delivery. Use of epoprostenol in inhaled form was first reported in the early 1990s, and it continues to be commonly employed in the inpatient setting, but its short half-life (under 6 minutes) requires continuous delivery that is impossible to provide in outpatient use.Citation13 Inhaled iloprost (Ventavis) was introduced in 1994 as the first inhaled pulmonary vasodilator appropriate for outpatient use, with its efficacy in a mixed group of PAH and CTEPH patients demonstrated in 2002 through a study by Olschewski et al showing a 58.8 meter six minute walk distance (6MWD) in the PAH patients at 12 weeks.Citation14 Iloprost uses a handheld nebulized delivery system, but its very high frequency of dosing (six to nine times daily) has limited widespread adoption.
Treprostinil is a synthetic prostacyclin with higher stability at room temperature and a longer half-life than epoprostenol. It was first introduced initially for subcutaneous use and approved by the FDA for PAH in 2002. A series of later studies by Voswinckel et al published in 2006 evaluated its use in inhaled form and demonstrated favorable improvements in hemodynamics that were more durable than those of iloprost.Citation15
Inhaled treprostinil solution was first approved for use in patients as a nebulized add-on to oral therapy in 2009 based on the results of the Addition of Inhaled Treprostinil to Oral Therapy for Pulmonary Arterial Hypertension (TRIUMPH) study.Citation16 This was a multi-center, randomized, placebo-controlled, double-blind trial that recruited 235 patients with PAH on stable doses of either bosentan or sildenafil. Patients were initiated on 3 breaths (18 ug) per inhalation and titrated to a maximum dose of 9 breaths four times daily. Their primary endpoint, 6MWD within 10 to 60 minutes of treprostinil inhalation at 12 weeks, showed a modest statistically significant difference, with a median increase at 20 meters in the treprostinil group compared to placebo, though this difference was smaller and not statistically significant in the sildenafil group alone. A small significant decrease in NT-pro-BNP was also found. No significant differences were observed in a composite endpoint of time to clinical worsening, defined as time to death, transplantation, hospital stay due to worsening PAH, or initiation of additional approved PAH-specific therapy. In the subsequent TRIUMPH open-label extension, there was a persistent increase in 6MWD by 18 m in the patients that continued therapy up to 24 months, with 36% reporting an improvement in NYHA Functional Class.Citation17
Common to prostacyclin therapies is a side effect profile that includes headache, flushing, jaw pain and “first bite” phenomenon, and gastrointestinal effects including nausea, vomiting, and diarrhea. Most side effects can be managed, and therapy continued, with symptom-targeted pharmacotherapy and dietary management. Subcutaneous delivery systems have the added issues of site pain, which often requires management with topical analgesic therapy; sites must be also rotated on a regular basis.Citation8 Indwelling catheters required for intravenous delivery require careful maintenance and carry the risk of bloodstream infections and thrombosis.Citation18 As first demonstrated in the TRIUMPH studies, cough, headache, nausea, and flushing were frequently experienced in those taking nebulized treprostinil.Citation17 Advantages and disadvantages of prostacyclin delivery methods are outlined in .
Table 1 Advantages and Disadvantages of Prostacyclin Formulations
Prostacyclin Therapy in PH-ILD
Pulmonary hypertension is a feared consequence of parenchymal lung disease. The presence of pulmonary hypertension in lung disease portends a higher mortality and worse outcomes regardless of the underlying type of lung disease.Citation19 As previously mentioned, the pathophysiology of PH in parenchymal lung disease is not completely understood, but there is increasing understanding that many patients develop progressive pulmonary vascular changes analogous to those seen in PAH, presenting a common thread to justify explorations of pulmonary vasodilator therapies in lung disease.
The use of prostacyclin therapy in PH-ILD is much more contemporary than in PAH, and there are no proven benefits to pulmonary vasodilator therapy in Group III disease outside of interstitial lung disease. Very early trials using a variety of medications, including nitric oxide, epoprostenol, and sildenafil, suggested improvement in gas exchange in small numbers of patients.Citation20,Citation21 Subsequent trials showed mixed results; a larger randomized controlled trial using iloprost in 51 patients with idiopathic pulmonary fibrosis (IPF) showed no differences in six-minute walk distance, NYHA Functional Class, dyspnea score, or exertional oxygen saturation.Citation22 A 2010 trial by Zisman et al using sildenafil in 180 patients with IPF also did not meet its primary endpoint of a 20% increase in six-minute walk distance, though did show improvements in quality of life and oxygen saturation.Citation23 Finally, the 2016 RISE-IIP trial, which employed riociguat in 143 of patients with PH due to idiopathic interstitial pneumonias (IIPs), was stopped early due to suggestion of increased mortality and adverse events, dampening hope for pulmonary vasodilator treatment in Group III disease considerably.Citation24
This changed with the publication of the landmark INCREASE trial, the first and as of this writing the only trial to establish the use of the inhaled prostacyclin treprostinil as efficacious in the treatment of pulmonary hypertension due to interstitial lung disease (PH-ILD).Citation7 This study was a multicenter, randomized trial comparing nebulized treprostinil versus placebo in 326 patients with pulmonary hypertension due to ILD of a variety of causes, with idiopathic interstitial pneumonia being the most common type. At week 16, those in the treprostinil group had reached a median of 12 puffs four times daily. There was a 31.12-meter increase in 6-minute walk distance, the primary outcome, with significant decreases in clinical worsening, nt-pro-BNP, and exacerbations of underlying lung disease. There was no significant difference in serious adverse events. The open-label study showed sustained increases in 6MWD and reductions in exacerbations of underlying lung disease at 52 weeks.Citation25 Post hoc analyses also showed a reduction in multiple clinical worsening events versus placebo, including reductions in forced vital capacity (FVC) and 6MWD, cardiopulmonary hospitalization, and death.Citation26
Unexpectedly, small but significant improvements in FVC occurred in patients in the treprostinil group, which was most clear in the idiopathic interstitial pneumonia patients, particularly idiopathic pulmonary fibrosis (IPF).Citation27 This finding has powered the presently active TETON (NCT04708782) and TETON-2 (NCT05255991) trials, which will evaluate inhaled treprostinil use in patients with idiopathic pulmonary fibrosis independent of the presence of pulmonary hypertension.
The use of inhaled treprostinil in PH due to chronic obstructive pulmonary disease (COPD) has unfortunately not shown the same degree of promise. The TAPIT-1 trial, a small trial of 10 PH-COPD patients, demonstrated safety with inhaled treprostinil use in these patients.Citation28 The adaptive Phase 3 PERFECT trial (NCT03496623), a randomized controlled study evaluating the use of nebulized treprostinil in PH-COPD, was terminated in August 2022 upon recommendation of its Data Safety Monitoring Committee at interim review.
Treprostinil Inhalation Powder (Tyvaso DPI)
Nebulized treprostinil has proven efficacy but is hampered somewhat by the bulk of the nebulizer device and duration of treatment; each use of the nebulizer takes 2 to 3 minutes, not including the preparation, maintenance, and cleaning of the device itself, and the device requires consumable filter membranes and electrical power.Citation29 This lack of portability and convenience led to the development of a dry powder inhalation form of the drug ( and ).
Figure 1 (A and B) Tyvaso delivery devices. Views of the Tyvaso nebulizer device and Tyvaso direct powder inhaler (DPI) device, with sizes to scale. Drug ampules(in envelope) are used with the nebulizer device, while cartridges (here, a light green 64 mcg dose cartridge) are used with the DPI device.
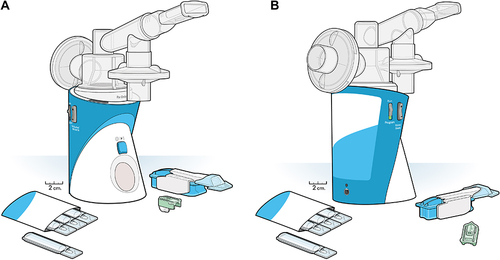
Tyvaso DPI powder (United Therapeutics, Silver Spring, MD) is at the time of this writing the only fully FDA-approved inhaled powder therapy and carries indications for both PAH and PH-ILD. The Tyvaso dry powder inhaler (DPI) using TreT was approved by the FDA on May 24, 2022. The formulation consists of a vehicle, fumaryl diketopiperazine (FDKP), and treprostinil, a prostacyclin mimetic that acts on the prostanoid receptors IP, DP1, and EP2.Citation30 The system uses a reusable inhaler device and single-use cartridges, which roughly approximate a set number of breaths from the Tyvaso nebulizer. Currently, cartridges are available in 16, 32, and 48, and 64 μg forms, with 80 μg dosage offered as the sequential use of a 64 μg and 16 μg cartridge. Like the nebulized form, the dry powder is rapidly inhaled, though pharmacokinetic variability appears to be less with the dry powder.
This formulation was first studied for safety and tolerability in a Phase 1 trial of 36 healthy normal volunteers given a spread of different drug doses and established 150 μg as the maximal tolerable dose.Citation31,Citation32 Clinical use of the Tyvaso DPI device was pioneered in the BREEZE study, an open-label clinical study focused on safety and tolerability of the device in PAH patients.Citation31 Fifty-one patients on a stable dose of inhaled nebulized treprostinil were transitioned to an equivalent dose of the DPI formulation; 49 completed the trial. Fifty-nine percent experienced an adverse effect, with no serious adverse effects attributed to the drug. Adverse effects were largely cough, headache, dyspnea, and nausea, and were felt to be consistent with those seen in other inhaled treprostinil studies.
A small but significant 11.5-meter improvement in six-minute walk distance was seen at just 3 weeks, with sustained improvements into the optional extension phase, though sample size decreased considerably at later time points. There was additionally improvement in the PAH-SYMPACT score, a multidomain questionnaire evaluating quality of life in patients with PAH. Patient satisfaction with the DPI device was clearly demonstrated, with 96% agreeing or strongly agreeing that they were satisfied with the device.
To date, there are no trials directly comparing nebulized treprostinil to the DPI form in a head-to-head fashion. The forms of inhaled treprostinil discussed in this review are summarized in .
Table 2 Approved and Experimental Formulations of Inhaled Treprostinil
Treprostinil Palmitil Inhalation Powder (TPIP)
A second form of inhaled trepostinil powder, treprostinil palmitil, is currently being developed by Insmed (Bridgewater, NJ). The principal difference between TPIP and Tyvaso DPI is the frequency of inhalation; TPIP is a prodrug with efficacy of at least 12 hours, and once daily dosing has been used in trials.Citation34 Two studies conducted using the Sugen/hypoxia rat model of PAH compared the hemodynamic effects of TPIP with other vasodilators – oral sildenafil in the first, and intravenous and inhaled treprostinil and oral selexipag in the second.Citation35,Citation36 These studies found at least equivalent efficacy in hemodynamic improvements in Su/Hx rats when comparing TPIP to established pulmonary vasodilators. Additionally, trials in animal models have suggested a higher cough threshold than conventional inhaled treprostinil, promising improved tolerance by reducing one of the drug’s principal adverse effects.Citation37
TPIP was first evaluated in human subjects in a phase Ib study to evaluate safety and tolerability of the drug.Citation38 Subjects were randomized to single or multiple (7 days) daily doses. Treatment-emergent adverse events largely consisted of cough, headache, and nausea, and upward dose titration appeared to reduce the incidence of adverse events compared to initiation at high dose. Pharmacokinetic testing found a drug half-life of between 6.84 and 8.82 hours, with overall testing supporting its use as a once-daily drug. Further development has focused on selection of an appropriate inhaler device, with a high inspiratory resistance of the RS01 device (Plastiape, S.p.A., Osnago, Italy) selected for use with capsules containing 8, 16, or 32 ug of TPIP.Citation39
A placebo-controlled, phase 2b study to evaluate TPIP in patients with PAH (NCT05147805) is currently recruiting, with patients gradually uptitrating the dose of TPIP over the 16-week trial period. Primary outcome is change in pulmonary vascular resistance from baseline at 16 weeks, with secondary outcomes including change in baseline six-minute walk distance, number of patients experiencing a treatment-emergent adverse event, and pharmacokinetic measurements. Primary completion is estimated in March of 2024. A smaller parallel phase 2 study (NCT05176951) aims to evaluate the drug in patients with PH-ILD and measuring primary outcomes of treatment-related adverse events, serious adverse events, and change in baseline peripheral oxygen saturation (SpO2). Both studies are planned to lead into an open-label extension (NCT05649748).
Yutrepia Treprostinil Inhalation Powder
A third formulation of treprostinil powder, Yutrepia (Liquidia Corporation, Morrisville, NC, USA), is also currently in development. Yutrepia is a dry powder inhalation form of treprostinil designed using a proprietary technology, PRINT, which aims to produce drug particles that are uniform in size, shape, and composition.Citation33 Like Tyvaso, the drug is dosed four times daily, though is inhaled as two breaths per capsule via a Plastiape inhaler device.
An initial phase 1 trial employing 79.5 ug of Yutrepia found that this dose had systemic exposure equivalent to that of nine breaths of nebulized treprostinil.Citation40 Bioavailability and tolerability appear to be similar to nebulized treprostinil.
A phase 3 open-label multicenter trial, INSPIRE, recruited patients with WHO Group I PAH who were either on a stable regimen that included nebulized treprostinil or who were naïve to prostacyclin therapy.Citation33 Patients were started at low dose (26.5 mcg qid) and uptitrated to a maximum of 212 mcg qid. As the trial was intended to support FDA approval of a new formulation of an approved drug, primary outcomes focused on the incidence of adverse and serious adverse events, with secondary outcomes including changes in six-minute walk distance, New York Heart Association Functional Class, and nt-pro-BNP levels from baseline. A total of 121 patients were enrolled, of whom 55 were in the group previously on nebulized treprostinil. Nearly all patients experienced at least one adverse event, and 28 (23.1%) experienced a serious adverse event, moreso in the prostacyclin-naïve group; 12 patients discontinued treatment before completing the trial.
As with other trials evaluating inhaled treprostinil therapy, cough was the most reported adverse event. Nearly all patients (98.2%) were reported to strongly favor the smaller Yutrepia system by week 2.
Yutrepia has not yet reached the market. Two months after the filing of the New Drug Application (NDA) for the compound in April 2020, United Therapeutics filed a lawsuit citing infringement of three patents. Yutrepia was granted tentative approval by the US Food & Drug Administration in November 2021; concurrently, the Patent Trial & Review Board issued a decision stating that the patent in question was unpatentable, a decision being appealed by United Therapeutics. Due to a district court ruling affirming that patent infringement did in fact occur, final FDA approval cannot be granted until patent expiration occurs in 2027. Amidst the ongoing legal process, Yutrepia will likely not see approval before 2026 or later.Citation41,Citation42 An amendment was submitted in September 2023 to add PH-ILD as an indication for the drug after the clinical investigation exclusivity for Tyvaso expires in March 2024.
Conclusions
Inhaled treprostinil is a relatively new addition to the pulmonary vasodilator arsenal in pulmonary arterial hypertension. Its efficacy for the treatment of PH-ILD, a subgroup previously without any proven PH-targeted treatment, is an exciting new development. The introduction of a dry inhalation powder form of the drug presents an option for drug delivery that is less cumbersome and more convenient than the nebulized form with a similar profile of adverse effects. New forms of inhaled treprostinil powder are also in development and may further expand the ability to deliver the drug to both PAH and PH-ILD patients when they enter the greater market.
Disclosure
Dr. Almario has no relevant disclosures. Dr. Ramani has served as a consultant for Merck and as a principal investigator for pharmaceutical studies with Janssen Pharmaceuticals and United Therapeutics. Dr. Cassady has served as principal investigator for pharmaceutical studies with Gossamer Bio, Ltd and reports consulting fees from Iota Biosciences Ltd., outside the submitted work. The authors report no other conflicts of interest in this work.
Acknowledgments
We wish to thank Dusica (Dee) Curanovic, PhD and Brittany Davis, PhD of United Therapeutics for their assistance in providing images to be used in this review.
References
- Humbert M, Kovacs G, Hoeper MM, et al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Respir J. 2022;1:3.
- Stacher E, Graham BB, Hunt JM, et al. Modern age pathology of pulmonary arterial hypertension. Am J Respir Crit Care Med. 2012;186(3):261–272. doi:10.1164/rccm.201201-0164OC
- van der Bruggen CEE, Tedford RJ, Handoko ML, van der Velden J, de Man FS. RV pressure overload: from hypertrophy to failure. Cardiovasc Res. 2017;113(12):1423–1432. doi:10.1093/cvr/cvx145
- Thenappan T, Ormiston ML, Ryan JJ, Archer SL. Pulmonary arterial hypertension: pathogenesis and clinical management. BMJ. 2018;360:j5492. doi:10.1136/bmj.j5492
- Piccari L, Allwood B, Antoniou K, et al. Pathogenesis, clinical features, and phenotypes of pulmonary hypertension associated with interstitial lung disease: a consensus statement from the pulmonary vascular research institute’s innovative drug development initiative - group 3 pulmonary hypertension. Pulm Circ. 2023;13(2):e12213. doi:10.1002/pul2.12213
- Medarov BI, Judson MA. The role of calcium channel blockers for the treatment of pulmonary arterial hypertension: how much do we actually know and how could they be positioned today? Respir Med. 2015;109(5):557–564. doi:10.1016/j.rmed.2015.01.004
- Waxman A, Restrepo-Jaramillo R, Thenappan T, et al. Inhaled treprostinil in pulmonary hypertension due to interstitial lung disease. N Engl J Med. 2021;384(4):325–334. doi:10.1056/NEJMoa2008470
- Farber HW, Gin-Sing W. Practical considerations for therapies targeting the prostacyclin pathway. Eur Respir Rev. 2016;25(142):418–430. doi:10.1183/16000617.0083-2016
- Gomberg-Maitland M, Olschewski H. Prostacyclin therapies for the treatment of pulmonary arterial hypertension. Eur Respir J. 2008;31(4):891–901. doi:10.1183/09031936.00097107
- Rubin LJ. Primary pulmonary hypertension. N Engl J Med. 1997;336(2):111–117. doi:10.1056/NEJM199701093360207
- Rubin LJ, Groves BM, Reeves JT, Frosolono M, Handel F, Cato AE. Prostacyclin-induced acute pulmonary vasodilation in primary pulmonary hypertension. Circulation. 1982;66(2):334–338. doi:10.1161/01.CIR.66.2.334
- Sitbon O, Vonk Noordegraaf A. Epoprostenol and pulmonary arterial hypertension: 20 years of clinical experience. Eur Respir Rev. 2017;26(143). doi:10.1183/16000617.0055-2016
- Burger CD, D’Albini L, Raspa S, Pruett JA. The evolution of prostacyclins in pulmonary arterial hypertension: from classical treatment to modern management. Am J Manag Care. 2016;22(1 Suppl):S3–15.
- Olschewski H, Simonneau G, Galie N, et al. Inhaled iloprost for severe pulmonary hypertension. N Engl J Med. 2002;347(5):322–329. doi:10.1056/NEJMoa020204
- Voswinckel R, Enke B, Reichenberger F, et al. Favorable effects of inhaled treprostinil in severe pulmonary hypertension: results from randomized controlled pilot studies. J Am Coll Cardiol. 2006;48(8):1672–1681. doi:10.1016/j.jacc.2006.06.062
- McLaughlin VV, Benza RL, Rubin LJ, et al. Addition of inhaled treprostinil to oral therapy for pulmonary arterial hypertension: a randomized controlled clinical trial. J Am Coll Cardiol. 2010;55(18):1915–1922. doi:10.1016/j.jacc.2010.01.027
- Benza RL, Seeger W, McLaughlin VV, et al. Long-term effects of inhaled treprostinil in patients with pulmonary arterial hypertension: the Treprostinil Sodium Inhalation Used in the Management of Pulmonary Arterial Hypertension (TRIUMPH) study open-label extension. J Heart Lung Transplant. 2011;30(12):1327–1333. doi:10.1016/j.healun.2011.08.019
- LeVarge BL, Channick RN. Inhaled treprostinil for the treatment of pulmonary arterial hypertension. Expert Rev Respir Med. 2012;6(3):255–265. doi:10.1586/ers.12.23
- King CS, Brown AW, Shlobin OA, et al. Prevalence and impact of WHO group 3 pulmonary hypertension in advanced idiopathic nonspecific interstitial pneumonia. Eur Respir J. 2018;52(1):1800545. doi:10.1183/13993003.00545-2018
- Olschewski H, Ghofrani HA, Walmrath D, et al. Inhaled prostacyclin and iloprost in severe pulmonary hypertension secondary to lung fibrosis. Am J Respir Crit Care Med. 1999;160(2):600–607. doi:10.1164/ajrccm.160.2.9810008
- Ghofrani HA, Wiedemann R, Rose F, et al. Sildenafil for treatment of lung fibrosis and pulmonary hypertension: a randomised controlled trial. Lancet. 2002;360(9337):895–900. doi:10.1016/S0140-6736(02)11024-5
- Krowka MJA, Frost A, Glassberg MK, et al. A randomized, double-blind, placebo-controlled study to evaluate the safety and efficacy of iloprost inhalation in adults with abnormal pulmonary arterial pressure and exercise limitation associated with idiopathic pulmonary fibrosis. Chest. 2007;132(4):633a. doi:10.1378/chest.132.4_MeetingAbstracts.633a
- Research N, Zisman DA, Schwarz M, et al.; Idiopathic Pulmonary Fibrosis Clinical. A controlled trial of sildenafil in advanced idiopathic pulmonary fibrosis. N Engl J Med. 2010;363(7):620–628.
- Nathan SD, Behr J, Collard HR, et al. Riociguat for idiopathic interstitial pneumonia-associated pulmonary hypertension (RISE-IIP): a randomised, placebo-controlled phase 2b study. Lancet Respir Med. 2019;7(9):780–790. doi:10.1016/S2213-2600(19)30250-4
- Waxman A, Restrepo-Jaramillo R, Thenappan T, et al. Long-term inhaled treprostinil for pulmonary hypertension due to interstitial lung disease: INCREASE open-label extension study. Eur Respir J. 2023;61(6):2202414. doi:10.1183/13993003.02414-2022
- Nathan SD, Tapson VF, Elwing J, et al. Efficacy of inhaled treprostinil on multiple disease progression events in patients with pulmonary hypertension due to parenchymal lung disease in the INCREASE trial. Am J Respir Crit Care Med. 2022;205(2):198–207. doi:10.1164/rccm.202107-1766OC
- Nathan SD, Waxman A, Rajagopal S, et al. Inhaled treprostinil and forced vital capacity in patients with interstitial lung disease and associated pulmonary hypertension: a post-hoc analysis of the INCREASE study. Lancet Respir Med. 2021;9(11):1266–1274. doi:10.1016/S2213-2600(21)00165-X
- Anderson JWR, Meadows C. Tapit treatment of pulmonary hypertension associated COPD with inhaled treprostinil: an open label, pilot study. Am J Respir Crit Care Med. 2017;195:A6906.
- Corporation UT. Package Insert for Tyvaso (treprostinil). Administration FD; 2022.
- Kolb M, Orfanos SE, Lambers C, et al. The antifibrotic effects of inhaled treprostinil: an emerging option for ILD. Adv Ther. 2022;39(9):3881–3895. doi:10.1007/s12325-022-02229-8
- Spikes LA, Bajwa AA, Burger CD, et al. BREEZE: open-label clinical study to evaluate the safety and tolerability of treprostinil inhalation powder as Tyvaso DPI in patients with pulmonary arterial hypertension. Pulm Circ. 2022;12(2):e12063. doi:10.1002/pul2.12063
- Smith PW, Kraft C, Grant K. A phase 1, single-center, open-label, dose-rising clinical trial to evaluate the pharmacokinetics, safety and tolerability of treprostinil inhalation powder (TreT) in healthy normal volunteers. Eur Respir J. 2019;54:PA4749.
- Hill NS, Feldman JP, Sahay S, et al. INSPIRE: safety and tolerability of inhaled Yutrepia (treprostinil) in pulmonary arterial hypertension (PAH). Pulm Circ. 2022;12(3):e12119. doi:10.1002/pul2.12119
- Plaunt AJ, Islam S, Macaluso T, et al. Development and characterization of treprostinil palmitil inhalation aerosol for the investigational treatment of pulmonary arterial hypertension. Int J Mol Sci. 2021;22(2):548. doi:10.3390/ijms22020548
- Corboz MR, Plaunt AJ, Malinin VS, et al. Assessment of inhaled treprostinil palmitil, inhaled and intravenous treprostinil, and oral selexipag in a sugen/hypoxia rat model of pulmonary arterial hypertension. J Pharmacol Exp Ther. 2022;383(1):103–116. doi:10.1124/jpet.122.001174
- Corboz MR, Plaunt AJ, Malinin V, et al. Treprostinil palmitil inhibits the hemodynamic and histopathological changes in the pulmonary vasculature and heart in an animal model of pulmonary arterial hypertension. Eur J Pharmacol. 2022;916:174484. doi:10.1016/j.ejphar.2021.174484
- Chapman RW, Corboz MR, Fernandez C, et al. Characterisation of cough evoked by inhaled treprostinil and treprostinil palmitil. ERJ Open Res. 2021;7(1):00592–2020. doi:10.1183/23120541.00592-2020
- Ismat FA, Usansky HH, Villa R, Zou J, Safety TA. Tolerability, and pharmacokinetics of treprostinil palmitil inhalation powder for pulmonary hypertension: a phase 1, randomized, double-blind, single- and multiple-dose study. Adv Ther. 2022;39(11):5144–5157. doi:10.1007/s12325-022-02296-x
- Gauani HB, Sullivan E, Cipolla D. Evaluation and selection of the inhaler device for treprostinil palmitil inhalation powder. Front Drug Deliv. 2022;1:2.
- Roscigno RF, Vaughn T, Parsley E, Hunt T, Eldon MA, Rubin LJ. Comparative bioavailability of inhaled treprostinil administered as LIQ861 and Tyvaso(R) in healthy subjects. Vascul Pharmacol. 2021;138:106840. doi:10.1016/j.vph.2021.106840
- Taylor NP United Therapeutics lands blow in inhaled drug patent dispute, pushing back approval of generic rival. Pharma Web site; 2022.
- Yasiejko C UTC sues liquidia to block FDA approval of yutrepia until 2026. 2023. Available from: https://news.bloomberglaw.com/ip-law/utc-sues-liquidia-to-block-fda-approval-of-yutrepia-until-2026.; Accessed December 29, 2023, 2023.