
Abstract
Objective
Metabolic syndrome refers to a collection of risk factors associated with the development of cardiovascular disease and type 2 diabetes mellitus (T2DM). Canagliflozin, a sodium glucose co-transporter 2 inhibitor, improves glycemic control and reduces body weight and blood pressure (BP) in a broad range of patients with T2DM. This post hoc analysis assessed the effects of canagliflozin on the components of metabolic syndrome in patients with T2DM and metabolic syndrome.
Methods
This analysis was based on data from 2 head-to-head studies of canagliflozin in patients with T2DM on background metformin versus glimepiride (study 1) and background metformin plus sulfonylurea versus sitagliptin 100 mg (study 2). Changes from baseline in glycemic efficacy, anthropometric measures, BP, and lipids were evaluated with canagliflozin versus glimepiride and sitagliptin at week 52 in patients who met ≥2 of the criteria for metabolic syndrome (in addition to T2DM): triglycerides ≥1.7 mmol/L; high-density lipoprotein cholesterol (HDL-C) <1.0 mmol/L (men) or <1.3 mmol/L (women); waist circumference ≥102 cm (non-Asian men), ≥88 cm (non-Asian women), >90 cm (Asian men), or >80 cm (Asian women); diagnosis of hypertension or meeting BP-related criteria (systolic BP ≥130 mmHg or diastolic BP ≥85 mmHg). Safety was assessed based on adverse event reports.
Results
In study 1, canagliflozin 100 and 300 mg provided similar and greater HbA1c reductions versus glimepiride, respectively. In study 2, canagliflozin 300 mg provided greater HbA1c lowering versus sitagliptin 100 mg. Canagliflozin also reduced fasting plasma glucose, body weight, body mass index, waist circumference, BP, and triglycerides, and increased HDL-C and low-density lipoprotein cholesterol versus glimepiride and sitagliptin. Canagliflozin was generally well tolerated in each study.
Conclusion
Canagliflozin was associated with improvements in all components of metabolic syndrome in patients with T2DM and metabolic syndrome, whereas glimepiride and sitagliptin only improved glycemic components over 52 weeks.
Introduction
Metabolic syndrome refers to a collection of risk factors associated with the development of cardiometabolic complications and type 2 diabetes mellitus (T2DM).Citation1 Criteria for the metabolic syndrome can vary, but typically include dyslipidemia (ie, increased triglycerides, reduced high-density lipoprotein cholesterol [HDL-C]), central obesity, hypertension, and glucose intolerance.Citation1,Citation2 In the United States, the prevalence of metabolic syndrome has been estimated to be nearly 35% in adults, with a higher prevalence (~50%) in those aged ≥60 years.Citation3 Metabolic syndrome is also prevalent in Europe, affecting an estimated ~40%–80% of men and ~25%–65% of women, depending on criteria, age, and geographic region.Citation4
Canagliflozin, a sodium glucose co-transporter 2 (SGLT2) inhibitor, increases urinary glucose excretion, leading to decreased plasma glucose levels and a net caloric loss in patients with T2DM.Citation5 Across phase 3 studies, canagliflozin improved glycemic control, body weight, and blood pressure (BP), and was generally well tolerated in a broad range of patients with T2DM.Citation6–Citation23 In head-to-head trials, canagliflozin 300 mg demonstrated superiority in HbA1c lowering versus glimepiride as add-on to metforminCitation20 and versus sitagliptin 100 mg as add-on to metformin or metformin plus sulfonylurea at 52 weeks.Citation8,Citation22 Canagliflozin also provided statistically significant reductions in body weight and BP compared with glimepiride and sitagliptin.Citation8,Citation20,Citation22 The improvements in HbA1c, body weight, and BP seen with canagliflozin suggest that it may be an effective treatment for improving the components of metabolic syndrome in patients with T2DM. The present analysis evaluated the effects of canagliflozin versus glimepiride and sitagliptin in patients with T2DM and metabolic syndrome.
Methods
Study design and patient populations
This post hoc analysis was based on data from 2 randomized, double-blind, head-to-head, phase 3 studies that evaluated the efficacy and safety of canagliflozin in patients with T2DM. In study 1 (ClinicalTrials.gov identifier: NCT00968812), patients (N=1,450) received canagliflozin 100 or 300 mg or glimepiride as add-on to metformin for a 52-week core treatment period, followed by a 52-week extension period;Citation20,Citation21 the current analysis was based on data from the 52-week core treatment period. In study 2 (ClinicalTrials.gov identifier: NCT01137812), patients (N=755) received canagliflozin 300 mg or sitagliptin 100 mg as add-on to metformin plus sulfonylurea for a 52-week core treatment period.Citation22 Details of the individual study designs and results have been published previously.Citation20,Citation22
The effects of canagliflozin versus glimepiride and sitagliptin on the components of metabolic syndrome were assessed in the subset of patients from each study who met ≥2 of the following criteria for metabolic syndrome (in addition to T2DM);Citation1,Citation2 triglycerides ≥1.7 mmol/L; HDL-C <1.0 mmol/L in men or <1.3 mmol/L in women; waist circumference ≥102 cm (non-Asian men), ≥88 cm (non-Asian women), >90 cm (Asian men), or >80 cm (Asian women); diagnosis of hypertension or meeting BP-related criteria (systolic BP ≥130 mmHg or diastolic BP ≥85 mmHg).
The studies included in this analysis were conducted in accordance with the ethical principles outlined in the Declaration of Helsinki and followed Good Clinical Practice and applicable regulatory requirements. Approval was obtained from institutional review boards and independent ethics committees for each participating center. Participants provided informed written consent prior to enrollment in the studies.
Endpoints/assessments
Changes from baseline in glycemic parameters (HbA1c and fasting plasma glucose [FPG]), anthropometric parameters (body weight, body mass index [BMI], and waist circumference), BP (systolic and diastolic), and lipids (low-density lipoprotein cholesterol [LDL-C], HDL-C, and triglycerides) were assessed at week 52. Safety and tolerability were assessed based on adverse event (AE) reports in the overall population of each study (not the subset of patients with metabolic syndrome), as the majority of patients in each study had metabolic syndrome.
Statistical analyses
Data were from the modified intent-to-treat (mITT) population, which consisted of all randomized patients who received ≥1 dose of study drug. The last observation carried forward (LOCF) approach was used to impute missing data. Efficacy endpoints were analyzed using an analysis of covariance model, with treatment, stratification factor, and frequently sampled mixed-meal tolerance test (study 2 only) as fixed effects and the corresponding baseline value as a covariate. Least squares mean differences and 2-sided 95% confidence intervals were estimated for the comparisons of canagliflozin versus glimepiride or sitagliptin. Statistical comparison of canagliflozin versus glimepiride or sitagliptin was not prespecified for these post hoc analyses; therefore, P values are not reported.
Results
Patients
At baseline, 81% (n=1,169) of 1,450 randomized patients with T2DM in study 1 and 78% (n=586) of the 755 randomized patients with T2DM in study 2 met the criteria for metabolic syndrome; proportions were similar across treatment groups in each study (study 1: 82%, 82%, and 79% with canagliflozin 100 and 300 mg and glimepiride, respectively; study 2: 77% and 79% with canagliflozin 300 mg and sitagliptin 100 mg, respectively). Baseline demographic characteristics were generally balanced across groups in the subset of patients with metabolic syndrome in each study ().
Table 1 Baseline demographic characteristics of patients who met the criteria for metabolic syndrome
Efficacy
In study 1, canagliflozin 100 and 300 mg were associated with similar and greater reductions in HbA1c, respectively, and greater reductions in FPG compared with glimepiride at week 52 (). Relative to glimepiride, canagliflozin 100 and 300 mg also provided greater reductions in body weight, BMI, and waist circumference (), and systolic BP and diastolic BP (). Canagliflozin 100 and 300 mg were associated with larger increases in HDL-C and LDL-C versus glimepiride at 52 weeks; numeric reductions in triglycerides were seen with canagliflozin 100 and 300 mg relative to glimepiride (). After 52 weeks, the proportion of patients who met the criteria for metabolic syndrome diagnosis was 87%, 86%, and 93% in the canagliflozin 100 mg, canagliflozin 300 mg, and glimepiride groups, respectively.
Figure 1 Effects on glycemic efficacy at week 52 in (A) study 1 and (B) study 2.
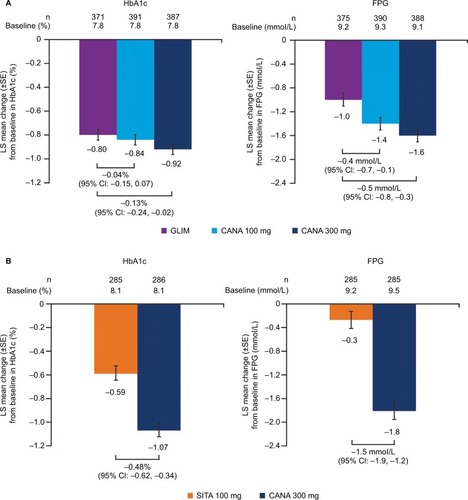
Figure 2 Effects on anthropometric measures at week 52 in (A) study 1 and (B) study 2.
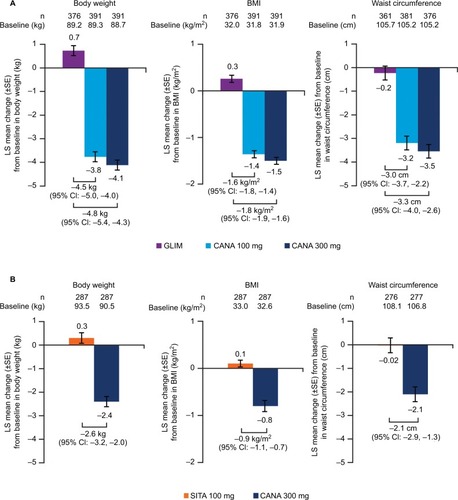
Figure 3 Effects on BP at week 52 in (A) study 1 and (B) study 2.
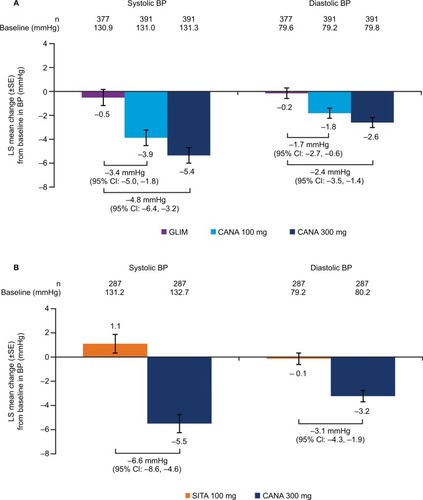
Figure 4 Effects on fasting plasma lipids at week 52 in (A) study 1 and (B) study 2.
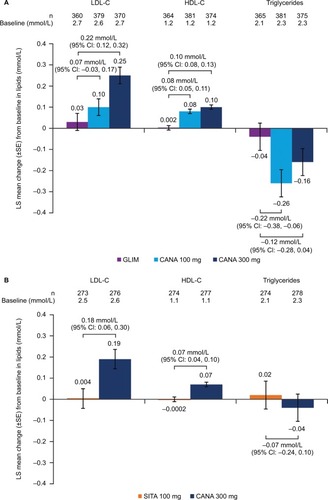
In study 2, canagliflozin 300 mg provided greater reductions in HbA1c and FPG versus sitagliptin 100 mg at 52 weeks (). Treatment with canagliflozin 300 mg versus sitagliptin 100 mg was also associated with greater reductions in body weight, BMI, and waist circumference (), and systolic BP and diastolic BP (). Increases in HDL-C and LDL-C and reductions in triglycerides were seen with canagliflozin 300 mg versus sitagliptin 100 mg (). The proportion of patients who met the criteria for metabolic syndrome at 52 weeks was 89% in the canagliflozin 300 mg group and 95% in the sitagliptin 100 mg group.
Safety
As the proportion of patients with metabolic syndrome was nearly 80% in each study, safety was assessed in the overall population of each study rather than in the subset of patients with metabolic syndrome. Canagliflozin was generally well tolerated in both studies, with a higher incidence of AEs related to the mechanism of SGLT2 inhibition (eg, genital mycotic infections, osmotic diuresis–related AEs).Citation20,Citation22 In study 1, the overall incidence of AEs was 64.4%, 68.5%, and 68.5% with canagliflozin 100 and 300 mg and glimepiride, respectively, at week 52.Citation20 Incidences of genital mycotic infections (male: 6.7% and 8.3% vs 1.1%; female: 11.3% and 13.9% vs 2.3%), urinary tract infections (6.4% and 6.4% vs 4.6%), and osmotic diuresis–related AEs (5.6% and 6.2% vs 1.7%) were higher with canagliflozin 100 and 300 mg compared with glimepiride.Citation20,Citation24 In addition, the incidence of documented hypoglycemia was significantly lower with canagliflozin 100 and 300 mg versus glimepiride (5.6% and 4.9% vs 34.2%).Citation20
In study 2, the overall incidence of AEs was 76.7% and 77.5% with canagliflozin 300 mg and sitagliptin 100 mg, respectively.Citation22 Incidences of genital mycotic infections (male: 9.2% vs 0.5%; female: 15.3% vs 4.3%) and osmotic diuresis–related AEs (5.0% vs 2.4%) were higher with canagliflozin 300 mg compared with sitagliptin 100 mg, whereas the incidence of urinary tract infections was similar between groups (4.0% vs 5.6%).Citation22 When added to a background of metformin and sulfonylurea, the incidence of documented hypoglycemia was similar with canagliflozin 300 mg and sitagliptin 100 mg (43.2% vs 40.7%), despite the larger reduction in HbA1c with canagliflozin in the overall study population.
Discussion
Canagliflozin improved all components of metabolic syndrome (glycemic control, BP, anthropometric measures, and dyslipidemia) in patients with T2DM and metabolic syndrome in both studies. Glycemic improvements were also seen with glimepiride and sitagliptin, albeit to a lesser extent than those seen with canagliflozin. Furthermore, neither glimepiride nor sitagliptin showed meaningful improvements in any of the other components of metabolic syndrome. Canagliflozin was generally well tolerated, with an increased incidence of AEs related to the mechanism of SGLT2 inhibition (ie, genital mycotic infections, osmotic diuresis–related AEs) in both studies.
The observed results are likely attributable to the mechanism of action for canagliflozin versus sitagliptin or glimepiride. By inhibiting SGLT2, canagliflozin increases urinary glucose excretion in an insulin-independent manner, thereby lowering plasma glucose levels and resulting in a mild osmotic diuresis and net caloric loss.Citation25 Consequently, canagliflozin confers multiple benefits in patients with T2DM, including glycemic improvement, weight loss, and BP reduction.Citation5 In contrast, dipeptidyl peptidase-4 inhibitors (eg, sitagliptin) have shown neutral effects on weight and BP, and sulfonylureas (eg, glimepiride) have been associated with weight gain and decreased efficacy over time.Citation26
Most patients (~80%) in each study met the criteria for metabolic syndrome diagnosis at baseline. A limitation of this analysis was its post hoc nature, as patients were not randomized based on the presence of metabolic syndrome. However, baseline characteristics were generally similar across treatment groups within each study. Changes in efficacy parameters related to metabolic syndrome were generally consistent with observations from the overall population in each study.Citation20,Citation22 Although further analyses based on patient characteristics were not done, the efficacy and safety of canagliflozin have been shown to be generally consistent in patients with T2DM in subgroups based on baseline demographic and disease characteristics (eg, sex, age, race, ethnicity, HbA1c, and T2DM duration).Citation27–Citation32 Results from this analysis are consistent with findings from preclinical studies demonstrating the beneficial effects of treatment with other SGLT2 inhibitors in the setting of metabolic syndrome.Citation33–Citation35 Despite these beneficial effects on all components of metabolic syndrome, there were small changes in the proportion of patients meeting the criteria for metabolic syndrome at week 52 in both studies. This is likely due to the continued diagnosis and treatment of T2DM, hypertension, and dyslipidemia following treatment in these studies. Furthermore, the present studies were not designed to ascertain the regression of metabolic syndrome.
The multifactorial nature of metabolic syndrome makes it a challenging condition to manage using currently available therapeutic agents.Citation36 Because canagliflozin has positive effects on multiple parameters (eg, glycemic, body weight, BP), it may be particularly beneficial for patients with metabolic syndrome and ultimately contribute to a decreased risk of cardiovascular disease. Results from the EMPA-REG OUTCOME trial have demonstrated reductions in cardiovascular risk in patients with T2DM treated with the SGLT2 inhibitor empagliflozin.Citation37 The potential benefits of canagliflozin on cardiometabolic outcomes are currently being assessed in the CANagliflozin cardio-Vascular Assessment Study (CANVAS) program, which consists of 2 ongoing trials in patients with T2DM and a history or high risk of cardiovascular disease (ie, CANVAS [ClinicalTrials.gov identifier: NCT01032629] and CANVAS-R [renal endpoints; ClinicalTrials.gov identifier: NCT01989754]).
Conclusion
These findings demonstrate that canagliflozin has beneficial effects on the multiple components of metabolic syndrome compared with glimepiride or sitagliptin in patients with T2DM and metabolic syndrome.
Acknowledgments
This analysis was funded by Janssen Scientific Affairs, LLC. Medical writing support was provided by Alaina Mitsch, PhD, of MedErgy, and was funded by Janssen Global Services, LLC.
Canagliflozin has been developed by Janssen Research & Development, LLC, in collaboration with Mitsubishi Tanabe Pharma Corporation.
Disclosure
MJD and KWM are full-time employees of Janssen Scientific Affairs, LLC. UV, DAB, and MD are full-time employees of Janssen Research & Development, LLC. The authors report no other conflicts of interest in this work.
References
- Eckel RH Grundy SM Zimmet PZ The metabolic syndrome Lancet 2005 365 9468 1415 1428 15836891
- O’Neill S O’Driscoll L Metabolic syndrome: a closer look at the growing epidemic and its associated pathologies Obes Rev 2015 16 1 1 12
- Aguilar M Bhuket T Torres S Liu B Wong RJ Prevalence of the metabolic syndrome in the United States, 2003–2012 JAMA 2015 313 19 1973 1974 25988468
- van Vliet-Ostaptchouk JV Nuotio ML Slagter SN The prevalence of metabolic syndrome and metabolically healthy obesity in Europe: a collaborative analysis of ten large cohort studies BMC Endocr Disord 2014 14 9 24484869
- Rosenthal N Meininger G Ways K Canagliflozin: a sodium glucose co-transporter 2 inhibitor for the treatment of type 2 diabetes mellitus Ann N Y Acad Sci 2015 1358 1 28 43 26305874
- Stenlöf K Cefalu WT Kim KA Efficacy and safety of canagliflozin monotherapy in subjects with type 2 diabetes mellitus inadequately controlled with diet and exercise Diabetes Obes Metab 2013 15 4 372 382 23279307
- Stenlöf K Cefalu WT Kim KA Long-term efficacy and safety of canagliflozin monotherapy in patients with type 2 diabetes inadequately controlled with diet and exercise: findings from the 52-week CANTATA-M study Curr Med Res Opin 2014 30 2 163 175 24073995
- Lavalle-González FJ Januszewicz A Davidson J Efficacy and safety of canagliflozin compared with placebo and sitagliptin in patients with type 2 diabetes on background metformin monotherapy: a randomised trial Diabetologia 2013 56 12 2582 2592 24026211
- Wilding JP Charpentier G Hollander P Efficacy and safety of canagliflozin in patients with type 2 diabetes mellitus inadequately controlled with metformin and sulphonylurea: a randomised trial Int J Clin Pract 2013 67 12 1267 1282 24118688
- Forst T Guthrie R Goldenberg R Efficacy and safety of canagliflozin over 52 weeks in patients with type 2 diabetes on background metformin and pioglitazone Diabetes Obes Metab 2014 16 5 467 477 24528605
- Neal B Perkovic V de Zeeuw D Efficacy and safety of canagliflozin, an inhibitor of sodium glucose co-transporter 2, when used in conjunction with insulin therapy in patients with type 2 diabetes Diabetes Care 2015 38 3 403 411 25468945
- Fulcher G Matthews DR Perkovic V Efficacy and safety of canagliflozin used in conjunction with sulfonylurea in patients with type 2 diabetes mellitus: a randomized, controlled trial Diabetes Ther 2015 6 3 289 302 26081793
- Fulcher G Matthews DR Perkovic V Efficacy and safety of canagliflozin when used in conjunction with incretin-mimetic therapy in patients with type 2 diabetes Diabetes Obes Metab 2016 18 1 82 91 26450639
- Rosenstock J Chuck L Gonzalez-Ortiz M Merton K Craig J Capuano G Initial combination therapy with canagliflozin plus metformin versus each component as monotherapy in drug-naive type 2 diabetes Diabetes Care 2016 39 3 353 362 26786577
- Rodbard HW Seufert J Aggarwal N Efficacy and safety of titrated canagliflozin in patients with type 2 diabetes mellitus inadequately controlled on metformin and sitagliptin Diabetes Obes Metab 2016 18 8 812 819 27160639
- Yale JF Bakris G Cariou B Efficacy and safety of canagliflozin in subjects with type 2 diabetes and chronic kidney disease Diabetes Obes Metab 2013 15 5 463 473 23464594
- Yale JF Bakris G Cariou B Efficacy and safety of canagliflozin over 52 weeks in patients with type 2 diabetes mellitus and chronic kidney disease Diabetes Obes Metab 2014 16 10 1016 1027 24965700
- Bode B Stenlöf K Sullivan D Fung A Usiskin K Efficacy and safety of canagliflozin treatment in older subjects with type 2 diabetes mellitus: a randomized trial Hosp Pract 2013 41 2 72 84
- Bode B Stenlöf K Harris S Long-term efficacy and safety of canagliflozin over 104 weeks in patients aged 55–80 years with type 2 diabetes Diabetes Obes Metab 2015 17 3 294 303 25495720
- Cefalu WT Leiter LA Yoon KH Efficacy and safety of canagliflozin versus glimepiride in patients with type 2 diabetes inadequately controlled with metformin (CANTATA-SU): 52 week results from a randomised, double-blind, phase 3 non-inferiority trial Lancet 2013 382 9896 941 950 23850055
- Leiter LA Yoon KH Arias P Canagliflozin provides durable glycemic improvements and body weight reduction over 104 weeks versus glimepiride in patients with type 2 diabetes on metformin: a randomized, double-blind, phase 3 study Diabetes Care 2015 38 3 355 364 25205142
- Schernthaner G Gross JL Rosenstock J Canagliflozin compared with sitagliptin for patients with type 2 diabetes who do not have adequate glycemic control with metformin plus sulfonylurea: a 52-week, randomized trial Diabetes Care 2013 36 9 2508 2515 23564919
- Ji L Han P Liu Y Canagliflozin in Asian patients with type 2 diabetes on metformin alone or metformin in combination with sulphonylurea Diabetes Obes Metab 2015 17 1 23 31
- Lavalle-González FJ Eliaschewitz FG Cerdas S Del Pilar CM Tong C Alba M Efficacy and safety of canagliflozin in patients with type 2 diabetes mellitus from Latin America Curr Med Res Opin 2016 32 3 427 439 26579834
- Mudaliar S Polidori D Zambrowicz B Henry RR Sodium-glucose cotransporter inhibitors: effects on renal and intestinal glucose transport: from bench to bedside Diabetes Care 2015 38 12 2344 2353 26604280
- Inzucchi SE Bergenstal RM Buse JB Management of hyperglycemia in type 2 diabetes, 2015: a patient-centered approach: update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes Diabetes Care 2015 38 1 140 149 25538310
- Sinclair A Bode B Harris S Efficacy and safety of canagliflozin compared with placebo in older patients with type 2 diabetes mellitus: a pooled analysis of clinical studies BMC Endocr Disord 2014 14 1 37 24742013
- Sinclair AJ Bode B Harris S Efficacy and safety of canagliflozin in individuals aged 75 and older with type 2 diabetes mellitus: a pooled analysis J Am Geriatr Soc 2016 64 3 543 552 27000327
- Gilbert RE Weir MW Fioretto P Impact of age and estimated glomerular filtration rate on the glycaemic efficacy and safety of canagliflozin: a pooled analysis of clinical studies Can J Diabetes 2016 40 3 247 257 27052454
- Gavin JR3rd Davies MJ Davies M Vijapurkar U Alba M Meininger G The efficacy and safety of canagliflozin across racial groups in patients with type 2 diabetes mellitus Curr Med Res Opin 2015 31 9 1693 1702 26121561
- Davidson JA Aguilar R Lavalle González FJ Efficacy and safety of canagliflozin in type 2 diabetes patients of different ethnicity Ethn Dis 2016 26 2 221 228 27103773
- Wilding JPH Blonde L Leiter LA Efficacy and safety of canagliflozin by baseline HbA1c and known duration of type 2 diabetes mellitus J Diabetes Complications 2015 29 3 438 444 25660137
- Rahman A Kittikulsuth W Fujisawa Y Effects of diuretics on sodium-dependent glucose cotransporter 2 inhibitor-induced changes in blood pressure in obese rats suffering from the metabolic syndrome J Hypertens 2016 34 5 893 906 26982381
- Tahara A Kurosaki E Yokono M Effects of SGLT2 selective inhibitor ipragliflozin on hyperglycemia, hyperlipidemia, hepatic steatosis, oxidative stress, inflammation, and obesity in type 2 diabetic mice Eur J Pharmacol 2013 715 1–3 246 255 23707905
- Thomas L Grempler R Eckhardt M Long-term treatment with empagliflozin, a novel, potent and selective SGLT-2 inhibitor, improves glycaemic control and features of metabolic syndrome in diabetic rats Diabetes Obes Metab 2012 14 1 94 96 21985693
- Matfin G Challenges in developing therapies for the metabolic syndrome Br J Diabetes Vasc Dis 2007 7 4 152 156
- Zinman B Wanner C Lachin JM Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes N Engl J Med 2015 373 22 2117 2128 26378978