Abstract
Purpose
This report examines the blood chemistry and blood pressure (BP) results from the Lifestyle Education for Activity and Nutrition (LEAN) study, a randomized weight loss trial. A primary purpose of the study was to evaluate the effects of real-time self-monitoring of energy balance (using the SenseWear™ Armband, BodyMedia, Inc Pittsburgh, PA) on these health factors.
Methods
164 sedentary overweight or obese adults (46.8 ± 10.8 years; BMI 33.3 ± 5.2 kg/m2; 80% women) took part in the 9-month study. Participants were randomized into 4 conditions: a standard care condition with an evidence-based weight loss manual (n = 40), a group-based behavioral weight loss program (n = 44), an armband alone condition (n = 41), and a group plus armband (n = 39) condition. BP, fasting blood lipids and glucose were measured at baseline and 9 months.
Results
99 participants (60%) completed both baseline and follow-up measurements for BP and blood chemistry analysis. Missing data were handled by baseline carried forward. None of the intervention groups had significant changes in blood lipids or BP when compared to standard care after adjustment for covariates, though within-group lowering was found for systolic BP in group and group + armband conditions, a rise in total cholesterol and LDL were found in standard care and group conditions, and a lowering of triglycerides was found in the two armband conditions. Compared with the standard care condition, fasting glucose decreased significantly for participants in the group, armband, and group + armband conditions (all P < 0.05), respectively.
Conclusion
Our results suggest that using an armband program is an effective strategy to decrease fasting blood glucose. This indicates that devices, such as the armband, can be a successful way to disseminate programs that can improve health risk factors. This can be accomplished without group-based behavioral programs, thereby potentially reducing costs.
Introduction
Prior reports of participation in physical activity (PA) interventionsCitation1–Citation5 have observed favorable changes in physiological risk factors. These reports led to the 2008 publication of the “Physical Activity Guidelines for Americans,” which documents that most health benefits result from at least 150 minutes of moderate activity a week, 75 minutes of vigorous activity a week, or a combination of the two along with two or more days of muscle-strengthening activities that work all major muscle groups.Citation6 Risk factors such as elevated levels of blood pressure (BP), blood lipids, and glucose play an important role in determining risk of developing chronic diseases or death.Citation7–Citation11 Prior PA intervention studies using technology tools (eg, pedometers) have used paper-based materials, such as in the First Step Program,Citation12 or have used groups to teach cognitive and behavioral strategies to increase PA.Citation13 Fewer studies have utilized technology-based approaches to promote weight loss and PA.Citation14–Citation18 It is important to examine new methods using the latest technology to provide feedback to participants in a study that is readily available, and flexible to their goals. The ability to use real-time feedback monitoring of energy expenditure may be a useful strategy to enable success in a wide variety of populations through its interactive nature, and must be studied more closely.
To our knowledge, relatively few randomized controlled trials (RCT) have examined technology-based weight loss approaches to improve BP, blood lipids, and glucose.Citation12,Citation14,Citation16,Citation17,Citation19,Citation20 The Lifestyle Education for Activity and Nutrition (LEAN) study was a 9 month RCT to determine the effectiveness of using the SenseWear™ Armband (BodyMedia, Inc Pittsburgh, PA) for weight loss among 164 sedentary and overweight or obese individuals. While weight loss was the primary outcome of LEAN, BP, blood lipids, and fasting glucose were a priori secondary outcomes.Citation21 The LEAN study provided an opportunity to examine the effects of various weight loss approaches on these selected cardiometabolic factors. Therefore, the primary aim of this report was to examine changes in BP, fasting blood lipids, and fasting glucose across different intervention conditions. Findings from this study will further our understanding of utilizing real-time self-monitoring devices on physiological outcomes.Citation19
Methods
Study design
A complete description of the LEAN study design and methods appears elsewhere.Citation21 In brief, the study was a RCT with a standard care control condition and 3 treatment conditions. The treatment conditions consisted of a group behavioral change intervention based on the transtheoretical model and social cognitive theoryCitation22 (group), an armband alone condition (armband), and a combined group-based weight loss intervention and armband condition (group + armband). The research protocol was reviewed and approved annually by the University of South Carolina Institutional Review Board. Written informed consent was obtained from all participants.
Study participants
Thorough descriptions of the recruiting and screening processes, as well as the methods are available.Citation21 Briefly, the study was limited to men and women aged 18 to 65 years who were sedentary (not accumulating 150 minutes of moderate to vigorous PA throughout the week in bouts ≥10 minutes), overweight or obese (body mass index [BMI] between 25.0–45.0 kg/m2), and with access to the internet. Exclusion criteria included significant weight loss (>20 lbs) in the prior 6 months; elevated BP (≥160/95 mm Hg); current participation in a formal weight loss program; using medications that affect weight; and ailments, medical conditions or other issues (eg, pregnancy) that limit PA or would prevent participants from adhering to the protocol. Individuals with a score of 16 or more on the Center for Epidemiological Studies Depression scale were excluded based on data from other studies demonstrating that depressed mood is associated with attrition from weight loss programs.Citation23 Participants were recruited from the greater Columbia, South Carolina area from February 2008 to January 2009.
Outcomes
All LEAN study staff were trained by the same supervisor to minimize inter-technician variability. Blood lipids and glucose were measured at baseline and 9-month assessment visits. Participants were instructed to fast (ie, no food or drink after midnight, besides water) for these assessments. All blood draws occurred between 7.00 am and 9.30 am and were taken from the antecubital vein. Serum samples were processed and analyzed using standardized procedures by a Versamax microplate reader (Molecular Devices, Inc, Sunnyvale, CA) using Pointe Scientific, Inc (Canton, MI) reagents and standards, to measure total cholesterol (TC), high-density lipoprotein (HDL), and triglycerides. Very-low-density lipoprotein (VLDL) was first calculated by dividing the triglyceride count by 5. Then the following equation was used to calculate low-density lipoprotein (LDL):
Other measures
Body weight to the nearest 0.25 lbs was assessed using a calibrated balance-beam scale. Height to the nearest 16th of an inch was assessed using a wall-mounted stadiometer. Smoking history and medication use were assessed by responses on detailed medical history questionnaires and reviewed by a physician.
Intervention
Participants were randomly assigned to either the standard care control condition or to one of the intervention conditions: group, armband, or group + armband.
Standard Care
These participants received a self-directed weight loss manual based on two evidence-based programs, Active Living Every Day (ALED)Citation25 and Healthy Eating Every Day (HEED).Citation26 The manual’s focus was to help individuals adopt healthful eating patterns and increase their PA levels. Cognitive and behavioral strategies consistent with the transtheoretical model and social cognitive theory were emphasized.Citation27,Citation28 All study participants received this manual.
Group
During the 9-month intervention, participants received 14 group sessions during the first 4 months, then 6 one-on-one telephone counseling sessions over the final 5 months. Each group session followed the ALED and HEED curriculum format from the manual, with the addition of a weekly weigh-in and more content directly related to weight loss. The one-on-one telephone counseling sessions were designed to promote the maintenance of behavior change.
Armband
The armband condition received the SenseWear™ platform consisting of the SenseWear™ Armband, a wrist watch with real-time display, and access to a personalized Weight Management Solutions web account. While wearing the armband and wrist watch display, participants received real-time feedback on several outcomes (ie, energy expenditure, minutes spent in moderate and vigorous PA, steps per day, progress towards goals). Feedback could be reviewed graphically (eg, energy intake, energy balance, and weight loss) as participants regularly downloaded their PA data and recorded daily energy intake and body weight to the Weight Management Solutions web account. Participants were asked to wear the armband at least 16 hours a day, 7 days a week.
Group + Armband
These participants received all components of the group condition with the addition of the SenseWear™ platform in the armband condition.
Participant retention, adherence, blinded assessment, and randomization
To facilitate retention and adherence, participants completed a 2-week pre-randomization run-in period and received a printed list of study requirements and expectations. Participants were compensated for completion of the baseline and month 4 assessment (US $10) and month 9 assessment (US $15), totaling US $25. Assessment personnel were blinded to intervention assignment. Participants were reminded not to discuss their condition assignment with the assessment team. Randomization assignment was computer generated and conducted by the statistician.
Statistical analysis
Descriptive baseline characteristics for conditions were tabulated as means and standard deviations (SD) or as percentages. Differences in blood chemistry and BP changes within and across conditions were tested by analysis of covariance with adjustment for baseline age, gender, race, education, recruitment wave, and baseline lipid values. Furthermore, BP and lipid measures were adjusted for baseline medications affecting the respective outcomes. An α level of 0.05 was used because it was an a priori intention to compare only the differences between the intervention conditions and the standard care condition.Citation21 Results are presented as adjusted means with standard error (SE) or 95% confidence intervals (CI).
For comparison, all outcomes were tested using only available data, without using baseline values carried forward for missing follow-up data. The results from these analyses did not differ substantially from the analyses with baseline values carried forward. For presentation herein, we report the baseline observation carried forward analyses using SAS statistical software, version 9.2 (SAS Inc, Cary, North Carolina).
Results
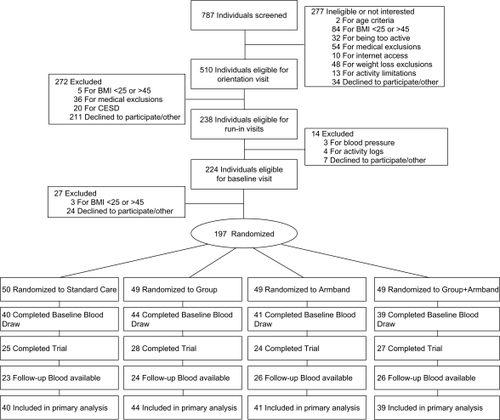
A total of 787 telephone screening calls were completed. Based on exclusion and inclusion criteria, 590 potential participants (75%) were ineligible (). After giving informed consent, 197 (25%) were randomized, of whom 164 (83%) had complete data at baseline. One hundred and four (63%) completed the study with 99 providing usable follow-up data (60%). Baseline values were carried forward for missing data or dropouts, so data from 164 of 197 participants (83%) were included in the primary analyses.
Figure 1 Consolidated Standards of Reporting Trials (CONSORT) diagram describing recruitment and retention of participants. If follow-up blood chemistry were missing, baseline values were carried forward.
The mean age was 47.6 ± 10.7 (SD) years and mean BMI 33.2 ± 5.3 (SD) kg/m2 for the participants in the study population, with 31.1% being African American (). About a third (31.1%) of the participants took medication for hypertension, and 26.8% were currently prescribed lipid lowering medication. Very few participants were taking medication for high blood glucose (7.3%). Only 4.9% of participants were current smokers, and a high percentage of participants (77.4%) were college graduates. Cardiovascular risk factors were within normal ranges.
Table 1 Baseline characteristicsTable Footnote*
presents the changes in BP and lipid variables. Compared with the standard care condition, none of the intervention conditions had significant changes in BP or lipids in analyses adjusted for baseline value, age, gender, race, education, medication, and recruitment wave. When groups were stratified by medication, these results did not differ (data not shown). Lower systolic blood pressures were found within the group (−2.96 mm Hg) and group + armband (−3.48 mm Hg) conditions (all P < 0.05). Significant within-group increases of TC and LDL were found in standard care (TC change, 18.32 mg/dL; LDL change, 15.84 mg/dL) and group (TC change, 15.58 mg/dL; LDL change, 13.71 mg/dL) conditions, respectively (all P < 0.05). There were also significant within-group decreases in triglycerides in both the armband (−13.07 mg/dL) and group + armband (−19.87 mg/dL) conditions (all P < 0.05).
Table 2 Change in blood pressure and lipidsTable Footnote*
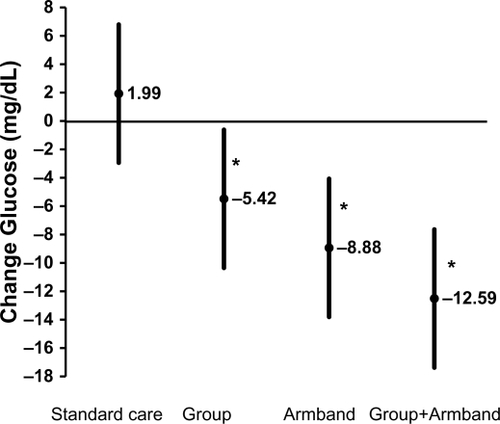
shows the mean change for fasting glucose for all conditions. Due to the low number of participants taking medication for blood glucose (n = 12), those persons were excluded, leaving 152 in the analysis. All values represent the least-squares means adjusted for age, gender, race, education, recruitment wave, and baseline glucose level. Compared with the standard care condition, mean glucose decreased by 5.42 mg/dL in the group condition, 8.88 mg/dL in the armband condition, and 12.59 mg/dL in the group + armband condition. Pairwise comparisons between standard care and group, armband, and group + armband conditions were significant (P < 0.05).
Figure 2 Mean change (least-squares mean ± 95% confidence interval) in fasting glucose for the standard care and intervention groups. Difference across groups were tested by analysis of covariance (ANCOVA) with adjustment for prespecified covariates (baseline age, gender, race, education, recruitment wave, and baseline glucose) among 152 participants not taking glucose medication. Significant ANCOVAs (P < 0.05) were followed by pair-wise comparisons to test whether intervention groups differed significantly from the standard care group.
Discussion
The primary finding from this RCT was a favorable reduction in fasting glucose in the treatment conditions. All treatment conditions showed a significant reduction when compared with the standard care condition. Only within-group conditions for group and group + armband were found for lower blood pressure. Other changes included within group lowering of triglycerides for the armband and group + armband treatments. Though not anticipated, the standard care and group treatments had unexpected higher TC and LDL values after 9 months. We speculate that this may have resulted from a change or discontinuation of medications, not following the fasting procedures, body weight changes, or other unknown causes. No differences were found between the group intervention, the armband alone, or a combination of the two on glucose. Overall, these findings suggest that a technology-based intervention with an armband, used as a real-time self-monitoring device, is a sufficient behavior change strategy for reducing fasting blood glucose after 9 months.
Comparison to other studies
Several studies incorporating technology-based devices using real-time feedback in their behavioral change strategies have focused on PA and weight changes in their designs.Citation15,Citation18 Few studies have included cardiometabolic changes.Citation12,Citation14,Citation16,Citation17,Citation19,Citation20 Of these, an internet-based RCT using Active Living Every Day (ALED) and pedometers found reductions in triglycerides (P = 0.01) and slight reductions in LDL and TC, resulting in a lower coronary risk ratio (CRR). Fasting glucose in this 16 week study did not change (P = 0.92).Citation14 Our study followed participants for a substantially longer time period, which could account for the reduction in blood glucose measures. In the First Step Program (FSP), a pedometer-based intervention, 47 overweight/obese sedentary individuals increased their activity at 16 and 24 weeks, but no significant changes were noted for glycemia, BP, or cholesterol values.Citation12 In a study by de Greef et al,Citation16 41 type 2 diabetics were randomized to a control group or an intervention group consisting of 5 group sessions in 12 weeks, and a booster session at 22 weeks plus a pedometer. At the 1-year follow up, results indicated no significant changes in TC or BP, but there was a significant decrease in HbA1c within both groups,Citation16 which agrees with our findings. Lastly, in the “Walking for Wellbeing in the West” study, while triglycerides and glucose were not measured, no differences were found for TC, HDL, or BP between or within the intervention or control groups.Citation17 Overall, our findings are comparable with the existing literature.Citation12,Citation14,Citation16,Citation17,Citation19,Citation20 Most studies found no changes to cholesterol levels.Citation12,Citation16,Citation17,Citation19,Citation20 Our findings for glycemic values agreed with one study we reviewed that dealt with technology,Citation16 but not with findings of other studies.Citation12,Citation14,Citation17,Citation19 Even so, it is recognized that being physically active is associated with reducing glucose levels.Citation29 We found very little change in BP values, which was consistent with the studies presented.Citation12,Citation14,Citation16,Citation17
The technology-based real-time monitoring used in LEAN is an example of a new type of self-monitoring. Traditional paper-based PA self-monitoring has demonstrated benefits in the past.Citation12,Citation30 With the advent of technological resources and the widespread availability of computers and web-based cell phones, the shift from paper to more advanced devices can provide flexibility in how data such as PA measures and energy expenditure are displayed and used for reinforcement of behavior change. Augmenting weight-loss interventions with real-time measurements and increased accessibility to PA history supports cognitive restraint from sedentary behaviors or improper food consumption by integrating constant reinforcement toward program goals.Citation30 The value and success of using technology-based methods may be attributable to the interactive experience associated with accessing information. This methodology can support users via tailored feedback and cues to assess and enhance their PA levels while tracking progress toward personalized goals. Further study on this tailoring is needed to enhance PA behavior change and maintain adherence to healthy lifestyle programs.
Physiological mechanisms
PA is known to influence several factors that may lower the levels of fasting blood glucose. Of primary importance is increasing insulin sensitivity and decreasing insulin resistance, resulting in improved metabolic responses when shuttling nutrients for glucose storage and usage.Citation31,Citation32 Habitual exercise has also been shown to increase citrate synthase and cellular GLUT-4 protein expression, each of which increases the uptake of glucose into the skeletal muscle.Citation33,Citation34 This can directly clear glucose more effectively from the blood stream. Weight loss itself has also been linked to lower glucose levels in the blood.Citation35 These physiologic responses together can explain why lower levels of fasting glucose were found. Modest blood pressure reduction has been found with those participating in regular exercise, though persons who are in stage 1 or 2 hypertension may benefit more than those who are normotensive.Citation36 Due to our population being in the latter category, we did not find great reductions in BP values. Greater improvements in these cardiometabolic risk factors may be more likely seen in those with either consistent or higher levels of energy expenditure in combination with diet interventions such as those in the HEED program materials.Citation26
Strengths and limitations
This study had several strengths, including the randomized design, the blinding of assessment staff to group assignments, the moderate length of follow-up, the quantitative measures used to assess the outcomes, and the large proportion of African Americans, lending diversity to our study population. This study was structured to allow comparisons with 4 different conditions, allowing detailed comparisons among different treatment modalities, including historically successful and future strategies. These results have probable implications for future commercialization and community interest in a minimal contact, widely dispersible alternative to group-based weight loss campaigns, which are relatively expensive. Our results may stimulate new intervention approaches to increase PA, with the result of lowering fasting glucose.
Limitations include large attrition rates in the standard care group (48% attrition rate), though this was similar in all groups. Most of the participants in the LEAN study were female (82%), and had a high level of education (college or above, 77%). This limits our results to similar populations. Information on changes or end of study prescription medication for BP, lipids, or glucose was not available. This may present a concern from internal validity threats due to the confounding nature of these substances on our outcome measures. However, assumptions were made that few persons on medication would enter or exit medication therapy or have their prescription changed dramatically. Due to costs, we only measured the cardiometabolic risk factors at baseline and month 9. We were not able to examine the relationship of the glucose, or the other values, with time. We suggest that future studies allow for several measurement points to investigate this relationship when using technology-based methods.
Conclusions
In this study of sedentary, overweight or obese men and women, all three treatments using group or armband conditions reduced fasting glucose levels when compared with standard care. No changes were found for BP or blood lipids between the standard care and treatment conditions. Our study suggests that the incorporation of armband technology into weight loss interventions can be an effective strategy to lower fasting glucose. This illustrates the value of utilizing real-time self-monitoring systems for measuring energy expenditure in future programs. Automated devices, such as the armband, can be a successful way to disseminate healthy lifestyle programs that can improve important health risk factors. This can be accomplished without group-based behavioral programs, thereby potentially reducing costs.
Funding source/trial registration
This study was funded by an unrestricted research grant provided by BodyMedia. This trial was registered at www.clinicaltrials.gov (No. NCT00957008).
Acknowledgments
We thank the study participants for their dedication to advancing science. We thank the University of South Carolina student researchers, Deidre Burch, Katelyn Tambellini, and Mia Taylor, for their dedication to participant recruitment and retention. We thank GO Christmus for editorial assistance. We also thank the University of South Carolina’s Clinical Exercise Research Director, Patrick Crowley; without his assistance, participant recruitment and data collection would not have been possible.
Disclosure
The authors report no conflict of interest in this work.
References
- Proper KI Hildebrandt VH Van der Beek AJ Twisk JW Van Mechelen W Effect of individual counseling on physical activity fitness and health: a randomized controlled trial in a workplace setting Am J Prev Med 4 2003 24 3 218 226 12657339
- Church TS Martin CK Thompson AM Earnest CP Mikus CR Blair SN Changes in weight, waist circumference and compensatory responses with different doses of exercise among sedentary, overweight postmenopausal women PLoS One 2009 4 2 e4515 19223984
- Fairey AS Courneya KS Field CJ Effect of exercise training on C-reactive protein in postmenopausal breast cancer survivors: a randomized controlled trial Brain Behav Immun 2005 19 5 381 388 15922556
- Kasapis C Thompson PD The effects of physical activity on serum C-reactive protein and inflammatory markers: a systematic review J Am Coll Cardiol 2005 45 10 1563 1569 15893167
- Lokey EA Tran ZV Effects of exercise training on serum lipid and lipoprotein concentrations in women: a meta-analysis Int J Sports Med 1989 10 6 424 429 2628361
- US Department of Health and Human Services 2008 physical activity guidelines for Americans [Updated 4 November 2009]. Available from: http://www.health.gov/PAGuidelines.
- Greenland P Knoll MD Stamler J Major risk factors as antecedents of fatal and nonfatal coronary heart disease events JAMA 2003 290 7 891 897 12928465
- Bild DE Folsom AR Lowe LP Prevalence and correlates of coronary calcification in black and white young adults: the Coronary Artery Risk Development in Young Adults (CARDIA) Study Arterioscler Thromb Vasc Biol 2001 21 5 852 857 11348886
- Blair SN Kampert JB Kohl HW Influences of cardiorespiratory fitness and other precursors on cardiovascular disease and all-cause mortality in men and women JAMA 1996 276 3 205 210 8667564
- Tuomilehto J Rastenyte D Jousilahti P Sarti C Vartiainen E Diabetes mellitus as a risk factor for death from stroke. Prospective study of the middle-aged Finnish population Stroke 1996 27 2 210 215 8571411
- Wolf PA D’Agostino RB Belanger AJ Kannel WB Probability of stroke: a risk profile from the Framingham Study Stroke 1991 22 3 312 318 2003301
- Tudor-Locke C Bell RC Myers AM Controlled outcome evaluation of the First Step Program: a daily physical activity intervention for individuals with type II diabetes Int J Obes Relat Metab Disord 2004 28 1 113 119 14569279
- Ash S Reeves M Bauer J A randomised control trial comparing lifestyle groups, individual counselling and written information in the management of weight and health outcomes over 12 months Int J Obes(Lond) 2006 30 10 1557 1564 16534529
- Carr LJ Bartee RT Dorozynski C Broomfield JF Smith ML Smith DT Internet-delivered behavior change program increases physical activity and improves cardiometabolic disease risk factors in sedentary adults: results of a randomized controlled trial Prev Med 2008 46 5 431 438 18207228
- Norman GJ Zabinski MF Adams MA Rosenberg DE Yaroch AL Atienza AA A review of eHealth interventions for physical activity and dietary behavior change Am J Prev Med 2007 33 4 336 345 17888860
- De Greef K Deforche B Tudor-Locke C De Bourdeaudhuij I A cognitive-behavioural pedometer-based group intervention on physical activity and sedentary behaviour in individuals with type 2 diabetes Health Educ Res 2010 25 5 724 736 20338978
- Baker G Gray SR Wright A The effect of a pedometer-based community walking intervention “Walking for Wellbeing in the West” on physical activity levels and health outcomes: a 12-week randomized controlled trial Int J Behav Nutr Phys Act 2010 7 1 51 20507592
- Polzien KM Jakicic JM Tate DF Otto AD The efficacy of a technology-based system in a short-term behavioral weight loss intervention Obesity 2007 15 4 825 830 17426316
- Bravata DM Smith-Spangler C Sundaram V Using pedometers to increase physical activity and improve health: a systematic review JAMA 2007 298 19 2296 2304 18029834
- Stefanick ML Physical activity for preventing and treating obesity-related dyslipoproteinemias Med Sci Sports Exerc 1999 31 11 Suppl S609 S618 10593536
- Barry VW McClain AC Shuger S Using a technology-based intervention to promote weight loss in sedentary overweight or obese adults: a randomized controlled trial study design Diabetes Metab Syndr Obes 2011 4 67 77 21448324
- Sharma M Behavioural interventions for preventing and treating obesity in adults Obes Rev 2007 8 5 441 449 17716301
- Clark MM Niaura R King TK Pera V Depression, smoking, activity level, and health status: pretreatment predictors of attrition in obesity treatment Addict Behav 1996 21 4 509 513 8830908
- Chobanian AV Bakris GL Black HR The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report JAMA 2003 289 19 2560 2572 12748199
- Blair S Dunn A Marcus B Carpenter R Active Living Every Day: 20 weeks to lifelong vitality Champaign Human Kinetics 2001
- Carpenter R Finley C Healthy Eating Every Day Champaign Human Kinetics 2005
- Prochaska JO Norcross JC DiClemente CC Changing for good: A revolutionary six-stage program for overcoming bad habits and moving your life positively forward New York, NY Avon Books Inc. 1994
- Bandura A Social foundations of thought and action: A social cognitive theory Englewood Cliffs, NJ Prentice Hall 1986
- Albright A Franz M Hornsby G American College of Sports Medicine position stand. Exercise and type 2 diabetes Med Sci Sports Exerc 2000 32 7 1345 1360 10912903
- Butryn ML Phelan S Hill JO Wing RR Consistent self-monitoring of weight: a key component of successful weight loss maintenance Obesity(Silver Spring) 2007 15 12 3091 3096 18198319
- van Baak MA Borghouts LB Relationships with physical activity Nutr Rev 2000 58 3 Pt 2 S16 S18 10812930
- Borghouts LB Keizer HA Exercise and insulin sensitivity: a review Int J Sports Med 2000 21 1 1 12 10683091
- Kraniou GN Cameron-Smith D Hargreaves M Effect of short-term training on GLUT-4 mRNA and protein expression in human skeletal muscle Exp Physiol 2004 89 5 559 563 15184360
- Ren JM Semenkovich CF Gulve EA Gao J Holloszy JO Exercise induces rapid increases in GLUT4 expression, glucose transport capacity, and insulin-stimulated glycogen storage in muscle J Biol Chem 1994 269 20 14396 14401 8182045
- Anderson JW Konz EC Obesity and disease management: effects of weight loss on comorbid conditions Obes Res 2001 9 Suppl 4 326S 334S 11707561
- Blumenthal JA Sherwood A Gullette ECD Exercise and weight loss reduce blood pressure in men and women with mild hypertension: effects on cardiovascular, metabolic, and hemodynamic functioning Arch Intern Med 2000 160 13 1947 1958 10888969