
Abstract
Background
Duodenal–jejunal bypass (DJB) is an important component of many types of current bariatric surgery including Roux-en-Y gastric bypass, mini-gastric bypass, biliopancreatic diversion, duodenal switch, and DJB plus sleeve gastrectomy. Surgery is often observed to ameliorate nonalcoholic steatohepatitis (NASH), but without a clearly delineated mechanism. In this study, we investigated the effects of DJB in diet-induced obese rats with NASH.
Materials and methods
Male Wistar rats were divided into four groups and fed the following diets over 6 months: A) normal chow (NC group, n=6); B) methionine–choline-deficient (MCD)–high-fat (HF) diet (HF group, n=6); C) MCD–HF diet for 3 months followed by DJB and MCD–HF diet for subsequent 3 months (DJB group, n=6); and D) MCD–HF diet for 3 months followed by treatment with pioglitazone (PGZ) with MCD–HF diet for subsequent 3 months (PGZ group, n=6). Body weight, glucose tolerance, the homeostatic model assessment-insulin resistance index, and lipid profiles were compared. Liver and visceral adipose tissue histology, inflammatory marker and hepatic stellate cell (HSC) activity, and hepatocyte autophagy were assessed.
Results
Compared with the HF group, the DJB group showed improved body weight, insulin sensitivity, lipid metabolism, and steatosis severity. The DJB group exhibited a significantly lower nonalcoholic fatty liver disease activity score than the HF and PGZ group (P<0.001 and P=0.003, respectively). Furthermore, DJB significantly reduced fat mass and adipocyte size. These effects were also observed in the PGZ group. Therefore, we speculated that the improvements induced by DJB are closely related to an alteration in insulin sensitivity. Moreover, DJB reduced HSC activity and TNF-α expression and enhanced hepatocyte autophagy.
Conclusion
DJB improves NASH through several mechanisms, particularly by altering insulin sensitivity, inflammatory responses, HSC activity, and hepatocyte autophagy.
Introduction
Nonalcoholic fatty liver disease (NAFLD), a clinically important chronic liver disease, affects 20%–30% of the general population.Citation1 Nonalcoholic steatohepatitis (NASH) is an advanced histological form of NAFLD, with a prevalence of 5.7%–17%.Citation2 Nearly 20% of NAFLD patients with NASH may develop liver cirrhosis, and 30%–40% of these patients die because of liver-related complications, such as hepatocellular carcinoma. NASH has also been predicted to become the leading indication for liver transplantation in the USA within a decade.Citation3 Based on these observations, understanding the pathophysiology of NASH and further development of effectively therapeutic interventions is becoming imperative. The current management of NAFLD and NASH typically includes a low-fat, low-calorie or Mediterranean diet, regular exercise, weight loss (if necessary), vitamin E, or pioglitazone (PGZ).Citation4 Several novel therapeutic agents are undergoing clinical trials, such as the PPAR family PPARα/δ ligand (elafibranor), bile acid-derived ligand for the nuclear hormone receptor (farnesoid X-activated receptor), obeticholic acid, and the glucagon-like peptide-1 (GLP-1) pathway activating agents.Citation5–Citation7 However, the US Food and Drug Association has not approved any drugs for NASH to date.
Most patients undergoing Roux-en-Y gastric bypass (RYGB) for morbid obesity experience a rapid improvement in glucose tolerance within the first month before marked weight loss. Approximately 83.7% and 98.9% of patients with type 2 diabetes mellitus (T2DM) experienced diabetic resolution after RYGB and biliopancreatic diversion (BPD), respectively.Citation8,Citation9 Lassailly et al demonstrated that bariatric surgery successfully treated NASH in nearly 85% of patients in 1 year.Citation10 Moreover, Furuya et al indicated that RYGB reduced hepatic steatosis and liver fibrosis by 84% and 75%, respectively, after 2 years of surgery.Citation11 These findings illustrate the potential role of bypass surgery in ameliorating NASH in patients.
Duodenal–jejunal bypass (DJB) is an important component of not only RYGB and BPD but also other current bariatric surgery practices including mini-gastric bypass, duodenal switch, and DJB plus sleeve gastrectomy. Only a few studies with small sample sizes have indicated that DJB surgery or endoscopic DJB linear devices can improve glucose intolerance and NAFLD-related parameters.Citation12–Citation14 However, there is no study focusing on the effects and mechanism of DJB for resolution of NASH. This study hypothesized that the reduction of hepatic steatosis and NASH following DJB is associated with many benefits originating from a proximal intestinal diversion. We analyzed the alterations in insulin sensitivity, liver and visceral fat histology, inflammatory responses, hepatic stellate cell (HSC) activity, and hepatocyte autophagy in diet-induced obese rats with NASH undergoing DJB. Understanding the underlying metabolic and molecular changes from DJB may provide a useful therapeutic target for NASH resolution.
Materials and methods
Animal model and experimental design
All experiments were performed in accordance with relevant guidelines and regulations of Laboratory Animal Center of National Cheng-Kung University, Taiwan. The research was also approved by the ethical committee of National Cheng-Kung University, Taiwan. A total of 24 male Wistar rats at 20 weeks of age were used. The rats were divided into four groups and fed the following diets plus specific intervention over a 6-month period: 1) normal chow for 6 months (NC group, n=6); 2) a methionine–choline-deficient (MCD)–high-fat (HF) diet (High Fat Diet Modified & Methionine/Choline Deficient Diet Pelleted; MP Biomedicals, Santa Ana, CA, USA) for 6 months (HF group, n=6); 3) a MCD–HF diet for 3 months followed by DJB (from the middle point of the study period onward), and MCD–HF diet for subsequent 3 months (DJB group, n=6); and 4) a MCD–HF diet for 3 months followed by treatment with PGZ at 5 mg/kg per day (Actos; Takeda Pharmaceutical Company Limited, Osaka, Japan) and MCD–HF diet for subsequent 3 months (PGZ group, n=6) (). The content of MCD–HF diet includes cotton seed oil, which contains 70% unsaturated fatty acids: 18% monounsaturated (oleic), 52% polyunsaturated (linoleic), and 26% saturated (primarily palmitic and stearic) fatty acids. The HF diet was used to induce obesity and insulin resistance in experimental rats. The MCD diet was used to develop an animal model of NASH through the induction of liver CYP2E1 and CYP4A, as described in previous studies.Citation15–Citation17 In the present study, we used both HF and MCD diets to mimic human dietary insulin resistance and NASH.
Figure 1 Experimental design and oral glucose tolerance test.
Abbreviations: DJB, duodenal–jejunal bypass; DJB group, MCD–HF diet for 3 months followed by DJB and MCD–HF diet for subsequent 3 months; HF, high fat; HFD, high fat diet; HF group, MCD–HF diet; MCD, methionine–choline-deficient; NC group, normal chow; PGZ group, MCD–HF diet for 3 months followed by treatment with PGZ with MCD–HF diet for subsequent 3 months; PGZ, pioglitazone.
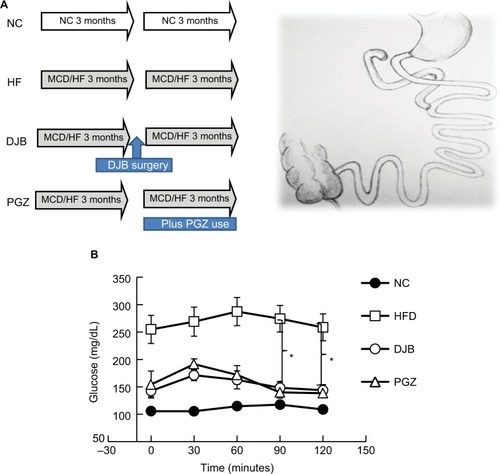
DJB was performed after 3 months of MCD–HF diet treatment. The DJB surgery included an end-to-end gastrojejunostomy and end-to-side jejunojejunostomy (). The biliopancreatic limb was 10 cm from the ligament of Treitz and the alimentary limb was 15 cm from the gastrojejunal anastomosis (Roux-en-Y reconstruction). The duodenal stump and two anastomoses were sutured in a one-layer manner by using microscopic surgical instruments and 6–0 Prolene under assistance from a surgical telescope. The rats were fed only glucose water in the first three postoperative days, and subsequently were allowed ad libitum access to water and the MCD–HF diet for further 3 months. PGZ, a PPAR-γ agonist, can ameliorate insulin resistance and improve glucose and lipid metabolism in patients with T2DM. It reverses the insulin resistance in the liver, adipose tissues, and muscles. PGZ was reported to improve liver histological findings by reducing steatosis, ballooning necrosis, and inflammation.Citation18 The use of PGZ group was to emphasize the effects of improved insulin sensitivity on NASH reduction.
Metabolic parameters and blood sampling
After 6 months, an oral glucose tolerance test (OGTT) with 2 g/kg glucose administered orally was performed after a 12-hour fast. Blood was drawn from the tail vein at 0, 30, 60, 90, and 120 minutes. The glucose level was determined using OneTouch Ultra (Johnson & Johnson, New Brunswick, NJ, USA). Three days after the OGTT, the rats were sacrificed. The alanine aminotransferase (ALT), triglyceride (TG), total cholesterol, insulin, IL-6, and TNF-α levels were measured. Liver function was determined using an ALT assay kit (Sigma Diagnostics, Livonia, MI, USA). TG was measured using ELISA kit of glycerol-3-phosphate oxidase and a photometric system (DiaSys Diagnostic Systems GmgH, Holzheim, Germany). Serum cholesterol levels were determined using the ELISA kit and CHOD–PAP enzymatic test on the photometric system. Insulin, IL-6, and TNF-α levels were measured using enzyme immunoassay kits (R&D Systems, Inc., Minneapolis, MN, USA). Insulin resistance was calculated through the formula of homeostasis model assessment-insulin resistance (HOME-IR) index: insulin (μU/mL) × glucose (mg/dL)/405.
Morphological examinations
Visceral epididymal fat pads were procured, and the weight was measured. H&E staining of liver and visceral fat was performed following standard procedures. The severity of fat accumulation, ballooning degeneration of hepatocytes, inflammation of acinar and portal tissues, and liver fibrosis were recorded. The NAFLD activity score (NAS) system was used to represent the quantitative severity of NAFLD and NASH.Citation19 The score was calculated as the unweighted sum of the scores for steatosis (0–3; <5%, 5%–33%, 34%–66%, and >66%), lobular inflammation (0–3; none, <2, 2–4, and >4 foci), and ballooning (0–2; none, few, and many cells). Thus, the score ranged from 0 to 8. The NAS was interpreted by clinical pathologist who is familiar to liver disease. Furthermore, the size of adipocytes in visceral fat was compared under the same degree field for each study group. Liver tissues were immunostained with monoclonal mouse antihuman α-smooth muscle actin (α-SMA; United States Biological, Salem, MA, USA) and Masson’s trichrome following the manufacturer’s instructions.
Lipogenic and fibrogenic gene expression
Real-time quantitative polymerase chain reaction (RT-qPCR) of liver tissues was performed to determine the mRNA expression of the most important fibrogenic gene transforming growth factor (TGF)-β1 and the lipogenic gene sterol regulatory element-binding factor-1 (SREBF-1). The liver total RNA content was extracted using the Trizol method and RNeasy mini kit (Qiagen NV, Venlo, the Netherlands). The cDNA was collected after reaction in a PCR machine for 5 minutes at 25°C, 60 minutes at 50°C, and 15 minutes at 70°C, and it was subsequently stored at −20°C. The primers were TGF-β1, forward: 5′-gAgCAACATgTggAACTCTAC-CAg-3′ and reverse: 5′-AAgCCCTgTATTCCgTCTCCT-3′ and SREBF-1, forward: 5′-TTCCATTgACAAggCCATgC-3′ and reverse: 5′-gCCTCATgTAggAATACCCTCCTC-3′. The sample cDNA was diluted, and RT-qPCR was subsequently performed using a Lightcycler TaqMan master kit (Hoffman-La Roche Ltd., Basel, Switzerland) under the following PCR conditions: preincubation at 95°C for 10 minutes, one cycle; amplification at 95°C for 10 seconds, 60°C for 30 seconds, and 72°C for 5 seconds, 50 cycles; cooling at 40°C for 30 seconds, one cycle.
Hepatocyte autophagy and endoplasmic reticulum stress
Cell autophagy is an intracellular pathway that targets cellular components, including organelles and proteins, to lysosomes for degradation. Both macroautophagy and chaperone-mediated autophagy in hepatic lipid metabolism, insulin sensitivity, and cellular injury were reported to have potential mechanistic roles for autophagy in hepatic steatosis and NASH.Citation20 Therefore, we examined the effects of DJB on the alterations in hepatocyte autophagy by determining the expression of microtubule-associated protein 1 light chain 3 (LC3), a cell macroautophagy marker, in a Western blot. We also measured the expression of glucose-regulated protein 78, the key chaperone protein mediating the endoplasmic reticulum stress response to prevent cell death.
Statistical analyses
Parametric data are expressed as means ± standard error of mean. The study groups were statistically analyzed using one-way ANOVA with Bonferroni multiple comparisons procedure among groups, such as for comparing NAS in each group. Significance was set at P<0.05. Statistical analyses were performed using SPSS, version 19.0 (IBM, Corporation, Armonk, NY, USA).
Results
DJB-ameliorated metabolic parameters in diet-induced obese rats with NASH
To define the metabolic changes resulted from DJB or PGZ under MCD–HF diet, we checked the weight of body, liver and visceral fat (net and adjusted to body weight), food intake, liver function, glucose level and insulin sensitivity, lipid profile, and inflammatory markers after 6 months (). We found that the postoperative food intake had no significant difference. DJB and PGZ both reduced body and liver weights (DJB and PGZ vs HF, body weight: P=0.003 and 0.005; liver weight: P=0.006 and <0.001), but there is no difference in body weight and liver weight between DJB and PGZ groups. Above data implicated that hepatic fat content could be reduced by both DJB and PGZ with comparable ability. DJB, but no PGZ, improved ALT value (DJB and PGZ vs HF, P=0.017 and 0.979). Compared with normal chow, the MCD–HF diet successfully induced glucose intolerance. This intolerance was improved both by DJB or PGZ (, DJB and PGZ vs HF, P=0.007 and 0.003 at 90 minutes; P=0.014 and 0.006 at 120 minutes). Insulin level was reduced by PGZ, but not by DJB (DJB and PGZ vs HF, P=0.830 and 0.002). It could be expected because GLP-1 is a well-known incretin hormone. HOMA-IR showed equivalent improvements in the DJB and PGZ groups (DJB and PGZ vs HF, P=0.035 and 0.002, group DJB vs PGZ P=0.990). The TG level was significantly reduced in the DJB and PGZ groups (groups C and D vs B, P=0.01 and 0.001; DJB vs PGZ, P=0.990). The progression of hepatic steatosis to inflammation is associated with proinflammatory cytokines. In this study, DJB and PGZ reduced the inflammatory cytokine TNF-α (DJB and PGZ vs HF, P=0.037 and 0.002; DJB vs PGZ, P=0.06).
Table 1 Effects of DJB and PGZ on metabolic parameters in MCD and HF diet-induced rats of nonalcoholic steatohepatitis
DJB reduced hepatic steatosis, inflammatory cell infiltration, and visceral fat mass
To define the hepatic morphological alteration caused by DJB and PGZ, we performed the H&E stain of liver and visceral tissue. In HF group, we observed a marked hepatic steatosis and lipid droplet accumulation (). Both DJB and PGZ attenuated the hepatic steatosis and inflammatory cell infiltration and the morphological improvement was more prominent in the DJB group. To quantify the severity of NAFLD, we calculated the NAS of each sample. The MCD–HF diet successfully induced NASH (NAS=6.83). DJB and PGZ groups exhibited lower NAS, and the effect was rendered more prominent by DJB (F(3,20) = 86.08, P<0.001; DJB and PGZ vs HF, P<0.001 and 0.003; DJB vs PGZ, P=0.003; ) (). The NAS of the DJB and PGZ groups were 1.33 and 3.17, which indicated non-NASH and borderline NASH statuses, respectively.
Figure 2 H&E staining of liver tissue after the 6-month protocol.
Abbreviations: DJB, duodenal–jejunal bypass; DJB group, MCD–HF diet for 3 months followed by DJB and MCD–HF diet for subsequent 3 months; HF, high fat; HF group, MCD–HF diet; MCD, methionine–choline-deficient; NC group, normal chow; PGZ group, MCD–HF diet for 3 months followed by treatment with PGZ with MCD–HF diet for subsequent 3 months; PGZ, pioglitazone.
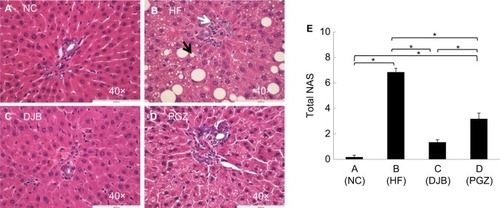
Table 2 NAFLD activity score (NAS) in each group
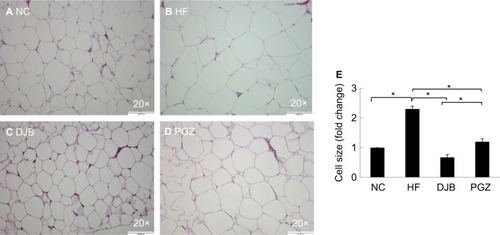
Excessive visceral fat is clinically an important risk factor for many metabolic syndrome-related disorders, such as obesity, diabetes, stroke, and coronary heart disease. In the present study, we measured the weight of epididymal fat pads and size of their adipocyte. Histologically, DJB significantly reduced epididymal fat mass and adipocyte size. The effects of DJB were also stronger than those of PGZ in microscopically observation ().
Figure 3 H&E staining of visceral epididymal fat tissue after 6 months.
Abbreviations: DJB, duodenal–jejunal bypass; DJB group, MCD–HF diet for 3 months followed by DJB and MCD–HF diet for subsequent 3 months; HF, high fat; HF group, MCD–HF diet; MCD, methionine–choline-deficient; NC group, normal chow; PGZ group, MCD–HF diet for 3 months followed by treatment with PGZ with MCD–HF diet for subsequent 3 months; PGZ, pioglitazone.
DJB improved NASH and fibrotic reaction
Advanced NASH may progress to a cirrhotic liver. Therefore, it is also worth noting whether DJB can prevent the progression of NASH to an irreversible fibrotic stage. Since we did not find the obvious fibrotic bundles in our liver tissues, probably due to insufficient time for the development of liver fibrosis, we observed the activity of HSCs by the expression of α-SMA and collagen bundle instead. The immunohistochemical staining revealed high α-SMA expression in HF group, but significantly lower in DJB and PGZ group (). These results suggest that DJB might prevent liver fibrosis through reducing HSC activity. The Masson’s trichrome stain also showed increased collagen bundle in HF group, but DJB and PGZ attenuated its formation (). In addition, the progression of hepatic steatosis to hepatic fibrosis is related to the upregulation of fibrogenic and lipogenic genes. In this study, the mRNA expression of fibrogenic gene, TGF-b1, and lipogenic gene, SREBF-1, was determined by RT-qPCR. The mRNA expression of TGF-β1 was significantly downregulated in the DJB and PGZ groups (). However, the expression of lipogenic gene, SREBF-1, seemed not to be influenced by DJB ().
Figure 4 α-SMA expression after 6 months.
Abbreviations: DJB, duodenal–jejunal bypass; DJB group, MCD–HF diet for 3 months followed by DJB and MCD–HF diet for subsequent 3 months; HF, high fat; HF group, MCD–HF diet; MCD, methionine–choline-deficient; NC group, normal chow; PGZ group, MCD–HF diet for 3 months followed by treatment with PGZ with MCD–HF diet for subsequent 3 months; PGZ, pioglitazone.
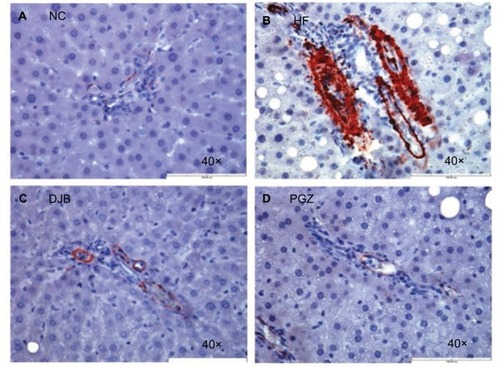
Figure 5 Masson’s trichrome stain for collagen bundle.
Abbreviations: DJB, duodenal–jejunal bypass; DJB group, MCD–HF diet for 3 months followed by DJB and MCD–HF diet for subsequent 3 months; HF, high fat; HF group, MCD–HF diet; MCD, methionine–choline-deficient; NC group, normal chow; PGZ group, MCD–HF diet for 3 months followed by treatment with PGZ with MCD-HF diet for subsequent 3 months; PGZ, pioglitazone.
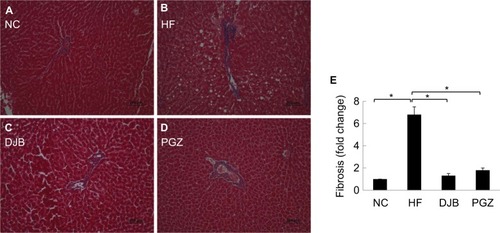
Figure 6 (A) mRNA expression of fibrogenesis gene. TGF-β1 was significantly downregulated by DJB and PGZ. (B) mRNA expression of lipogenesis gene. SREBF-1 was not improved by DJB or PGZ. Each value is expressed as mean ± standard error of the mean (n=6). *P<0.05. (C) DJB increased LC3 expression (lane 1: NC group; lanes 2 and 3: DJB group; lane 4: HF group). The presenting grouping blots [LC3 or β-actin] were cropped from the same field of the same gel. (D) Quantitative evaluation of LC3 expression by fold change. *P<0.05.
![Figure 6 (A) mRNA expression of fibrogenesis gene. TGF-β1 was significantly downregulated by DJB and PGZ. (B) mRNA expression of lipogenesis gene. SREBF-1 was not improved by DJB or PGZ. Each value is expressed as mean ± standard error of the mean (n=6). *P<0.05. (C) DJB increased LC3 expression (lane 1: NC group; lanes 2 and 3: DJB group; lane 4: HF group). The presenting grouping blots [LC3 or β-actin] were cropped from the same field of the same gel. (D) Quantitative evaluation of LC3 expression by fold change. *P<0.05.](/cms/asset/ad73625e-4a2f-4a47-b7bf-091c06a8a023/dmso_a_190631_f0006_b.jpg)
DJB enhanced hepatocyte autophagy
Recently, the role of autophagy in hepatic lipid metabolism has been noticed and the NAFLD may be related to the defects of hepatic cell autophagy.Citation20 It has not yet known whether DJB can modify the function of hepatic cell autophagy. We then observe the expression of LC3 in different groups. During the insult of the MCD–HF diet, hepatocyte autophagy was activated as a protective reaction to increase lipophagy (, lane 4). DJB increased the LC3 activity; that is, DJB can consolidate or strengthen the hepatic cell autophagy (, lanes 2 and 3). DJB significantly enhanced the LC3 expression compared to PGZ (P=0.02 and<0.001) ().
Discussion
The initial “two-hit hypothesis” was proposed for NASH pathogenesis by Day and James in 1998.Citation21 Accumulating evidence demonstrates that NASH is a multifactorial disease comprising genetic predisposition, gut-derived endotoxin and ethanol, intestinal microbiota, environmental factors, cell apoptosis, and hepatic autophagy.Citation22 In this study, we discovered multiple benefits from DJB for resolution of NASH.
Though PGZ sometimes induce weight gain due to water retention of body composition in human use, our rat model did not show this effect. Other rat models also demonstrated an equal or even a decrease in body weight while using PGZ.Citation23,Citation24 Based on our results and these reports, whether PGZ can also induce weight gain in different species needs further investigation. We also observed the decrease in body weight in DJB group. Therefore, body weight loss may be a confounding factor when explaining the metabolic improvement from DJB or just body weight loss. We could not identify the time point at which NASH completely developed before the occurrence of the significant body weight difference in the experimental period; instead, we emphasized the clinical observation of early improvements before large body weight loss in a short period after RYGB. In real world, body weight loss after bypass bariatric surgery is an expected beneficial effect in clinical practice. In future, additional studies with checkups at different intervals during the experimental period should be considered.
Currently, many methods and indices are available for the estimation of insulin resistance. Gutch et al have tested and validated the reliability of these methods and indices, including HOMA-IR, the quantitative insulin sensitivity check index, the hyperinsulinemic euglycemic clamp, and intravenous glucose tolerance test.Citation25 Although HOMA-IR has been proposed as a more simple method of evaluating insulin sensitivity, it is less accurate than the hyperinsulinemic euglycemic clamp test. This was a limitation of the present study. Furthermore, it is worth to mention that insulin level was reduced by PGZ with improvement of insulin sensitivity, but not in DJB. In many studies of human subjects after bariatric surgery, the secretion of GLP-1 after meals was enhanced. As we know, GLP-1 is an incretin factor, and it function is to promote the secretion of insulin from pancreatic β cells.
DJB improved liver function and ALT level, but PGZ did not. This finding was compatible with clinical reported temporary hepatotoxicity caused by use of thiazolidinediones such as troglitazone. These results seem to contradict the benefits of PGZ reported in a clinical placebo-controlled study conducted by Belfort et alCitation18 ALT is often included as an outcome in NASH trials; however, its clinical implications are limited, because the changes in ALT reflect acute changes in necroinflammatory activity but are not necessarily parallel to histological disease activity and stage.Citation26 In addition, we observed the lower expression of IL-6 in the DJB group than in the MCD–HF and PGZ groups; however, the results did not reach statistical significance, possibly because of the small sample size (n=6) and wide variation among the individual animals. Nevertheless, we cannot neglect the crucial role of inflammatory cytokines in insulin resistance and NASH.
In this study, no severe fibrotic bundles were found in liver tissues although Masson’s trichrome staining was performed, probably because of the lack of adequate time for the development of liver fibrosis. Xu et al reported a significant development of liver fibrosis from NASH only after 6 months of an HF diet;Citation27 however, we observed the activity of HSCs instead. We observed that DJB inhibited the activity of HSCs to prevent the progression of diet-induced NASH. An MCD diet was reported to upregulate the mRNA expression of TGF-b1 and its downstream molecules, α1 (I) procollagen (collagen I) and plasminogen activator inhibitor-1, in rat livers.Citation17 In this study, the mRNA expression of TGF-b1 was decreased by both DJB and PGZ. About the lipogenic pathway, no differences were observed in SREBF-1 expression regardless of DJB. The influence of DJB on the lipogenesis pathway still needs to be clarified.
Autophagy, the autodigestion of cellular proteins and organelles within a cell, has recently been shown to play an important role in the pathogenesis of insulin resistance, obesity, and NAFLD. Autophagy is also involved in hepatic lipid homeostasis and innate immune response to harmful oxidants and cytokines.Citation28,Citation29 A study reported that autophagic flux was impaired in the livers of mice fed with an MCD diet. Activation of autophagy using rapamycin can attenuate steatosis, fibrosis, inflammation, mitochondrial dysfunction, and ER stress.Citation30 Thus, the pharmacological agents of promoting cell autophagy may provide a novel therapeutic strategy for NASH treatment. By observing the expression of LC3, we found that DJB may improve hepatocyte autophagy. GLP-1 was ever reported to ameliorate NAFLD by enhancing the mitochondrial structure and promoting autophagy via the sirtuin 1 (SIRT1)–SIRT3–forkhead box O3A pathway.Citation31 Liu Y et al have also demonstrated the role of GLP-1 on resolution of NAFLD by promoting hepatic autophagy, fatty acids oxidation or reducing fatty acids synthesis.Citation32 Therefore, the benefit from DJB may be related to the increased secretion of incretin factors following bypass.
Therapeutic options for NAFLD and NASH include diet modification, increased physical activity, weight loss, vitamin E, or PGZ. Several novel therapeutic agents are emerging in clinical trials. It is worth noting that a bile acid-derived ligand for farnesoid X-activated receptor, obeticholic acid, has shown effective results. Bile acids are no longer considered solely for lipid absorption but have diverse effects on regulating host immunity and inflammation. Recently, the role of microbiota in NASH progression and liver carcinogenesis has also been noticed. PK Jena and YJ Wan have further investigated the interaction of microbiota and FXR in Western diet-induced liver injury through FXR knockout (KO) mice. They found that male Western diet-fed FXR KO mice had the most severe steatohepatitis. Hepatic inflammation can be reduced by antibiotics. The improvement was accompanied by decreased free and conjugated secondary bile acids as well as changes in gut microbiota. The results revealed that Lactococcus, Lactobacillus, and Coprococcus protect the liver from inflammation.Citation33 Not only for therapeutic medicine or probiotics, PK Jena and YJ Wan also examined the application of prebiotics in treating NASH. They found that both synbiotics Bifidobacterium infantis and milk oligosaccharides are effective in reversing cancer-prone NASH using Western diet-fed FXR KO mice.Citation34
In this study, we did not assess the effects of DJB on the alterations of incretin hormones and genetic expression. Clinically, there is strong evidence stating that bariatric surgery can cure T2DM in most morbidly obese patients by improving incretin factors. Another critical point is the possible discrepancies between humans and rats in relation to DJB surgery. Whether this concept from the rat model can be applied to humans is questionable. Regarding NASH induction in rats and naturally developed NASH in humans, previous studies have shown a different distribution of bile acid metabolomics and amino acid metabolomics related to entering the citrate cycle and undergoing glycolysis or gluconeogenesis in hepa-tocytes.Citation35 Evidence has also indicated that metabolic alterations after RYGB in rodents might be different from those in humans. The total energy expenditure increase in rodents after RYGB is not observed in humans. In rodent RYGB models, incretins increase not only postprandially but also in the fasting state; however, in humans, an incretin increase occurs only in response to meals. In RYGB rats, the wet weight of the small intestine increases markedly, indicating the hypertrophy of the intestinal mucosa with the increased release of GLP-1 and PYY from L-cells.Citation36 Arora et al observed decreases in rat-specific Lactobacillus animalis and L. reuteri in the small intestine of diabetic fa/fa rats after RYGB and found that the decrease was related to glucose tolerance.Citation37 These findings are critical because the mechanisms have a secondary beneficial effect on liver histology. Therefore, not all results of rodent NASH models can be incorporated into the discussion of the mechanisms in humans. Despite these limitations, we revealed the various mechanisms underlying the potential therapeutic role of DJB for NASH. DJB can be used as an alternative therapeutic option for NASH patients who fail to respond to life modifications and medical interventions.
Conclusion
DJB has a potential role of reducing NAFLD severity and preventing NASH progression. The multifactorial mechanism might be related to the modulation of insulin sensitivity, reduction of TNF-α expression, activity of HSCs, and autophagy of hepatocytes.
Disclosure
The authors report no conflicts of interest in this work.
References
- Dowman JK Tomlinson JW Newsome PN Pathogenesis of nonalcoholic fatty liver disease QJM 2010 103 2 71 83 19914930
- Matteoni CA Younossi ZM Gramlich T Boparai N Liu YC Mccullough AJ Nonalcoholic fatty liver disease: a spectrum of clinical and pathological severity Gastroenterology 1999 116 6 1413 1419 10348825
- Wong RJ Aguilar M Cheung R Nonalcoholic steatohepatitis is the second leading etiology of liver disease among adults awaiting liver transplantation in the United States Gastroenterology 2015 148 3 547 555 25461851
- Sanyal AJ Chalasani N Kowdley KV Pioglitazone, vitamin E, or placebo for nonalcoholic steatohepatitis N Engl J Med 2010 362 18 1675 1685 20427778
- Ratziu V Harrison SA Francque S Elafibranor, an agonist of the peroxisome proliferator-activated receptor-α and -δ, induces resolution of nonalcoholic steatohepatitis without fibrosis worsening Gastroenterology 2016 150 5 1147 1159 26874076
- Neuschwander-Tetri BA Loomba R Sanyal AJ Farnesoid X nuclear receptor ligand obeticholic acid for non-cirrhotic, non-alcoholic steatohepatitis (FLINT): a multicentre, randomised, placebo-controlled trial Lancet 2015 385 9972 956 965 25468160
- Armstrong MJ Gaunt P Aithal GP Liraglutide safety and efficacy in patients with non-alcoholic steatohepatitis (LEAN): a multicentre, double-blind, randomised, placebo-controlled phase 2 study The Lancet 2016 387 10019 679 690
- Buchwald H Avidor Y Braunwald E Bariatric surgery: a systematic review and meta-analysis JAMA 2004 292 14 1724 1737 15479938
- Rubino F R’bibo SL del Genio F Mazumdar M McGraw TE Metabolic surgery: the role of the gastrointestinal tract in diabetes mellitus Nat Rev Endocrinol 2010 6 2 102 109 20098450
- Lassailly G Caiazzo R Buob D Bariatric surgery reduces features of nonalcoholic steatohepatitis in morbidly obese patients Gastroenterology 2015 149 2 379 388 25917783
- Furuya CK de Oliveira CP de Mello ES Effects of bariatric surgery on nonalcoholic fatty liver disease: preliminary findings after 2 years J Gastroenterol Hepatol 2007 22 4 510 514 17376042
- Petry TZ Fabbrini E Otoch JP Effect of duodenal-jejunal bypass surgery on glycemic control in Type 2 diabetes: a randomized controlled trial Obesity 2015 23 10 1973 1979 26414562
- Koehestanie P de Jonge C Berends FJ Janssen IM Bouvy ND Greve JW The effect of the endoscopic duodenal-jejunal bypass liner on obesity and type 2 diabetes mellitus, a multicenter randomized controlled trial Ann Surg 2014 260 6 984 992 25072436
- de Jonge C Rensen SS Koek GH Endoscopic duodenal-jejunal bypass liner rapidly improves plasma parameters of nonalcoholic fatty liver disease Clin Gastroenterol Hepatol 2013 11 11 1517 1520 23920034
- Leclercq IA Farrell GC Field J Bell DR Gonzalez FJ Robertson GR CYP2E1 and CYP4A as microsomal catalysts of lipid peroxides in murine nonalcoholic steatohepatitis J Clin Invest 2000 105 8 1067 1075 10772651
- George J Pera N Phung N Leclercq I Yun Hou J Farrell G Lipid peroxidation, stellate cell activation and hepatic fibrogenesis in a rat model of chronic steatohepatitis J Hepatol 2003 39 5 756 764 14568258
- Ota T Takamura T Kurita S Insulin resistance accelerates a dietary rat model of nonalcoholic steatohepatitis Gastroenterology 2007 132 1 282 293 17241878
- Belfort R Harrison SA Brown K A placebo-controlled trial of pioglitazone in subjects with nonalcoholic steatohepatitis N Engl J Med 2006 355 22 2297 2307 17135584
- Kleiner DE Brunt EM Van Natta M Design and validation of a histological scoring system for nonalcoholic fatty liver disease Hepatology 2005 41 6 1313 1321 15915461
- Amir M Czaja MJ Autophagy in nonalcoholic steatohepatitis Expert Rev Gastroenterol Hepatol 2011 5 2 159 166 21476911
- Day CP James OF Steatohepatitis: a tale of two “hits”? Gastroenterology 1998 114 4 842 845 9547102
- Liu W Baker RD Bhatia T Zhu L Baker SS Pathogenesis of nonalcoholic steatohepatitis Cell Mol Life Sci 2016 73 10 1969 1987 26894897
- Ding SY Shen ZF Chen YT Sun SJ Liu Q Xie MZ Pioglitazone can ameliorate insulin resistance in low-dose streptozotocin and high sucrose-fat diet induced obese rats Acta Pharmacol Sin 2005 26 5 575 580 15842776
- Gad MZ Ehssan NA Ghiet MH Wahman LF Pioglitazone versus metformin in two rat models of glucose intolerance and diabetes Pak J Pharm Sci 2010 23 3 305 312 20566445
- Gutch M Kumar S Razi SM Gupta KK Gupta A Assessment of insulin sensitivity/resistance Indian J Endocrinol Metab 2015 19 1 160 25593845
- Mahady SE Webster AC Walker S Sanyal A George J The role of thiazolidinediones in non-alcoholic steatohepatitis – a systematic review and meta analysis J Hepatol 2011 55 6 1383 1390 21703200
- Xu ZJ Fan JG Ding XD Qiao L Wang GL Characterization of high-fat, diet-induced, non-alcoholic steatohepatitis with fibrosis in rats Dig Dis Sci 2010 55 4 931 940 19459046
- Lavallard VJ Gual P Autophagy and non-alcoholic fatty liver disease BioMed Res Int 2014 2014 4 1 13
- Torres DM Williams CD Harrison SA Features, diagnosis, and treatment of nonalcoholic fatty liver disease Clin Gastroenterol Hepatol 2012 10 8 837 858 22446927
- Chen R Wang Q Song S Liu F He B Gao X Protective role of autoph-agy in methionine-choline deficient diet-induced advanced nonalcoholic steatohepatitis in mice Eur J Pharmacol 2016 770 C 126 133 26593434
- Tong W Ju L Qiu M Liraglutide ameliorates non-alcoholic fatty liver disease by enhancing mitochondrial architecture and promoting autophagy through the SIRT1/SIRT3-FOXO3a pathway Hepatol Res 2016 46 9 933 943 26666995
- Liu Y Wei R Hong TP Potential roles of glucagon-like peptide-1-based therapies in treating non-alcoholic fatty liver disease World J Gastroenterol 2014 20 27 9090 9097 25083081
- Jena PK Sheng L Liu HX Western diet-induced dysbiosis in farnesoid X receptor knockout mice causes persistent hepatic inflammation after antibiotic treatment Am J Pathol 2017 187 8 1800 1813 28711154
- Jena PK Sheng L Nagar N Synbiotics Bifidobacterium infantis and milk oligosaccharides are effective in reversing cancer-prone nonalcoholic steatohepatitis using Western diet-fed FXR knockout mouse models J Nutr Biochem 2018 57 246 254 29800811
- Han J Dzierlenga AL Lu Z Metabolomic profiling distinction of human nonalcoholic fatty liver disease progression from a common rat model Obesity 2017 25 6 1069 1076 28452429
- Lutz TA Bueter M The physiology underlying Roux-en-Y gastric bypass: a status report Am J Physiol Regul Integr Comp Physiol 2014 307 11 R1275 R1291 25253084
- Arora T Seyfried F Docherty NG Diabetes-associated micro-biota in fa/fa rats is modified by Roux-en-Y gastric bypass ISME J 2017 11 9 2035 2046 28524868