
Abstract
Introduction
Hypertension is among the first five causes of mortality, globally contributing more than 40% to cardiac related deaths worldwide, with almost 70% cardiovascular deaths in the low- and middle-income countries. Its burden is projected to be 150 million by 2025 based on epidemiological data within the Sub-Saharan Africa regions, with Ghana experiencing 505,180 increases in 2007. It is currently among the leading cause of death in the country, with prevalence ranging from 19% to 48%. There is limited data concerning hypertension on Ghanaian youth. Particularly, on those at the Senior High School (SHS) level that represents the immediate workforce of the country on the depth of prevalence, knowledge as well as the risk factors that may predispose them into having prehypertension and hypertension for proper records and interventional measures and that is what this study pursues to do.
Materials and methods
A cross-sectional study was employed in five different SHSs in the Ashanti region of Ghana from December 2018 to February 2019 with structured questionnaires and physical screening of participants. Logistic regression analysis was performed to test for relation knowledge and riskfactors on HTN.
Results
The overall prevalence of pre-HTN within the group was 33.8%, with stages 1 and 2 HTN prevalence of 5.4%. Sixty-three percent do not have an idea of what HTN is, and positive associations were found between no physical exercises, no addition of extra salt, type of food often eaten and family history.
Conclusion
This study establishes prevalence in pre-HTN within students at the SHS level with low knowledge and high risk factors on the disease. This indication is beneficial to target the interventional programs on this population at this early stage by inculcating education on HTN prevalence and its risks in the educational curricular by the government.
Introduction
Hypertension(HTN) still remains one of the five leading cause of mortality globally, with more than 40% of deaths related to cardiac diseases.Citation1 This accounts for 9.4 million deaths and a minimum of 45–51% cardiovascular diseases (CVDs). With nearly 70% deaths related to CVDs in the low- and middle-income countries (LMICs), the WHO data predict a 1.56 billion (60%) increase in the global burden by the year 2025,Citation2 while almost 3 of every 4 hypertensive patients would be living in the LMICs.Citation3 Hypertension prevalence has increased from almost 80 million adults in Sub-Saharan Africa from the year 2000 to an estimated increase of 150 million in 2025 based on current epidemiological data.Citation3 Again in Sub-Saharan Africa, a study of four regions reveals a burden of 25.9% with associated risks factors such as older age, body mass index (BMI), level of education among others.Citation4
Over the past few years, Ghana has witnessed more than a ten-fold increase from 49,087 in 1988 to 505,180 in 2007, with an increase in outpatient disease from 1.7% to 4.0% in all ages.Citation5 As an important cause of heart and renal failure in Ghana, HTN and stroke have been among the leading cause of admission and death in the country.Citation6 Prevalence of HTN in Ghana ranges between 19% and 48% within rural and urban communities, and studies have shown a fraction of 21.4% and higher in men of all age groups in this country,Citation7 though another study discloses a 13% prevalence of HTN among people within the ages of 15–49 in Ghana with low awareness.Citation8 The above-mentioned statistics all relate to adult populations. However, the prevalence of hypertension is estimated to be 1–2% and is reported to be on the increasing trend among adolescents largely due to the current obesity epidemic in children.Citation9
Knowledge gaps are key obstructions in the effective avoidance and treatment of HTN.Citation10 Knowledge in the form of health literacy allows individuals to progress on their health outcomes. Although this does not rest solely on the capability of skills of the individual,Citation11 research has shown a positive relationship on the proportion of knowledge, with persons with blood pressure under control.Citation12 It has been reported that knowledge and understanding of possible risks related to HTN and probable effects of lifestyle changes are insufficient in Ghana as the country still experiences misconceptions and gaps on knowledge on HTN in its rural communities. Official education, communication gaps and unreachability to routine health instruction programs among others have been well-known to impede on the knowledge on HTN.Citation7 The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents, published as far back in 2004, also established the condition “prehypertension” in parallel with adult hypertension guidelines. The long-term health risks for hypertension in children and adolescents can be extensive.Citation13 It is actually estimated that the presence of high blood pressure in children with normal weight is highly overlooked.Citation14 A proper record of the depth of knowledge and its risks of HTN among a population, which represents the immediate workforce of the country, is necessary to effectively monitor and draw health campaign programs as far as HTN is concerned. This study, therefore, conveys evidence on the prevalence, knowledge as well as risk factors of HTN in students in Ghana at the Senior High School (SHS) Level who are the representation of the immediate workforce of the country.
Materials and methods
Study settings and participants
This cross-sectional study engaged a convenience sampling at five SHSs in the Ashanti Region of Ghana from November 2018 to February 2019. Due to the current rotational shift method employed by the Ghana education Services on its curricular, students who were immediately available at the scheduled time of any particular school and gave approval were recruited to partake in this study. Public SHSs which were directly under the education directorate were targeted. The Ashanti Region was chosen because of its location in the middle belt of the country and the fact that permission had been granted by the Service Directorate (Reference No. 14/90/33) to conduct the study.
Procedure for collection of data and data collection tool
Measurement of blood pressures of participants was taken in accordance with the “Pan-African Society of Cardiology” (PASCAR) recommendations in 2014,Citation15 by using automatic (MOTECH TrueScan, Germany blood pressure monitors) and a mercury sphygmomanometer. Due to resource and logistical constraints, multiple measurements for all participants were not done. However, participants with high readings were asked to sit for 30 mins after which readings were repeated and an average reading was recorded to the nearest mmHg.
The (Detecto Stainless steel 437) was used to measure weights of participants while heights were measured by the height rod and stadiometers. BMI was calculated by dividing the weight (kg) by the height (m2) and categorized under standard approvals by the WHO. Waist circumference was taken and recorded in centimeters; for females it was grouped as <70c cm as very low, 70–89 cm as low, 90–109 as high and ≥110 as very high while that for males it was grouped as <80 cm as very low, 80–99 cm as low and 110–120 as high.
All individual information on a participant was written on their respective coded questionnaire, which they filled after they were through with the screening exercise, and submitted to the group performing the screening. The questionnaire contained three parts, with part one measuring the sociodemographic characteristics of participants. Part two focused on knowledge of hypertension among the participants, whereas the last part focused on the possible risk factors of hypertension among the participants. Particularly, risk factors focused on physical activities, salt intake and general diet of participants. Professional nurses and a professional medical doctor were engaged throughout the screening period. Blood pressure readings were classified according to the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7), 2003.Citation16 Categories were normal with systolic blood pressure (SBP) ≥120 and diastolic blood pressure (DSB) 80; pre-HTN as SBP 120–139 and DBP 80–89; stage 1 as SBP 140–159 and DBP 90–99 and stage 2 with SBP ≥160 and DBP ≥100.
Ethical consideration
This study was approved by Zhengzhou university’s ethical committee and permission was granted by the Service Directorate with (Reference no. 14/90/33). Official letters were also dispersed to heads of schools. Heads of schools were asked to introduce the study to parents of students during a Parent Teacher Association (PTA) meeting. Parents who did not want their children to participate in the study were asked to identify themselves and also inform their children not to report at the study grounds. Therefore, researchers assumed that parents had given their consent if students reported at the study grounds. Again, verbal approval was sought from partakers before registering them into the study. For purposes of secrecy, the names of participants or schools are not contained in this study.
Data analysis
Data were imputed and analyzed by using SPSS version 24, and multinomial logistic regression was used to test for the strength of associations between variables, while a P-value of ≤0.05 was set as significant.
Results
Background characteristics and anthropometric measurements
Respondents were all SHS students within the study area. As depicted in , the mainstream (571) of them were between the ages of 15–17 years representing 49.2%, while the lesser (128) representing 11% were less than 15 years. Females formed 61.2% of the population studied, and 462 signifying almost 40% of participants had their heights between 151 and 160 cm, while (29) which 2.5% were less than 140 cm.
Table 1 Background characteristics and anthropometric measurements and its relationship between HTN of respondents
Four hundred and seventy representing 40.5% weighed between 51 and 60 kg and formed the majority, whereas 20 representing 1.7% weighed less than 40 kg. Most of the femaleparticipants (37%) were within the normal hip circumference range, 4% had very high and 2.9% had very low, while their male counterparts had 61.3%, 0.9% and 8.5% of them with normal, very high and very low hip circumferences ranges, respectively. On BMI classification, 58.9% were within the normal range, while 0.3% were class 3 obesity.
Prevalence of hypertension
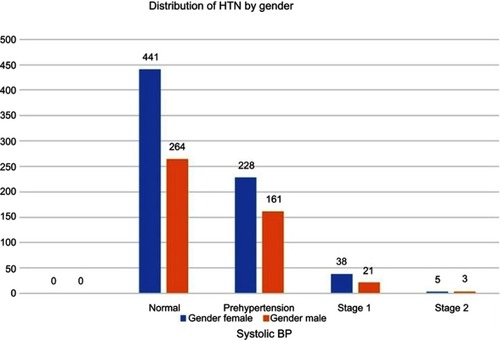
Among the 1,161 students who fully participated in this study, 705 representing 60.7% were within the normal ranges of HTN. The study realized a 33.5%, 5.1% and 0.7% prevalence of pre-HTN, stage 1 and stage 2 HTN within its participants. The distribution of HTN with age and gender is presented in and , respectively. A total of 200 representing 51.4% with pre-HTN were within the age ranges of 15–17 years followed by the age group of ≥18 with n=161 (41.4%) and n=28 representing 7.2% for respondents who were <15 years. However, 61% of respondents with stage 1 HTN were ≥18, followed by ages 15–17 years with 30.5%. Distribution of hypertension by gender revealed more female 441 (62.6%) with normal reading than males as well as female having a higher proportion 58.6% with pre-HTN. Female were also more than males in stages one and two with 64.4% and 62.5% correspondingly.
Figure 1 Distribution of HTN by age of respondents.
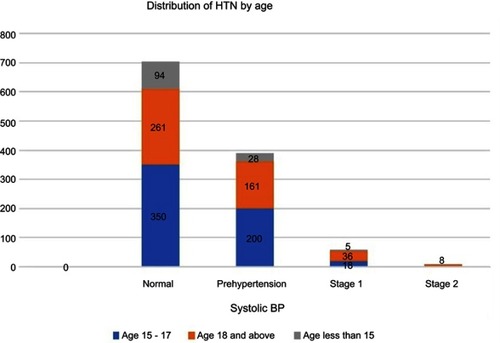
Figure 2 Distribution of HTN by gender of respondents.
shows the knowledge of HTN within respondents. Overall, 63% of respondents do not have an idea of what HTN is, while 52.3% do not know whether a family member has the disease or not. A few 3.0% have been diagnosed with HTN before and 40.9% do not know the causes of HTN.
Table 2 Knowledge on hypertension
a, presents the associations between age and gender on knowledge on HTN and 3b, is on associations between risk factors and knowledge on HTN. The study finds a positive association between the age ranges of 15–17 years, as well as ≥18 years with CI of (0.255–0.638) and (0.266–0.675) correspondingly. It also found possitive association with being female and hypertension with CI: (1.056–1.729). Again, there were positive associations on those who do not engage in any physical exercises at all (CI: 1.048–1.932), who said “NO” to add extra salt to cooked foods (CI: 1.106–1.897) and the type of foods regularly eaten by respondents. Additionally, this study also found positive associations between participants who responded “Don’t know“ and “NO” to whether their family member is hypertensive or not.
Table 3 Association between Hypertension and other variables
Discussion
This study included a total sample of 1,161 students from SHS. There were more females than males as shown in , and were all at the SHS level, which represents adolescent respondents. Due to resource challenges, multiple readings were conducted for only participants who recorded higher BP at first reading. This current study on SHS students reveals a high prevalence of hypertension on the future generation of Ghana, with almost 40% with pre-HTN and a little over 5% with stages 1 and 2 HTN. This corresponds to the already existed literature of a 26.1% prevalence of pre-HTN in students of the Kwame Nkrumah University of Science and Technology (KNUST).Citation17 Although their study may differ a bit by the age range of their sample, it depicts a future speedy increase of the disease among indigenes of this country if measures are not put in place. It also serves as a guide to perhaps why the adult HTN prevalence ranges within 19–48%Citation7 and denotes focusing more interventional measures on primary disease prevention at an earlier age rather than on adults where tertiary preventive measures normally become the option especially within the African communities and in the Sub-Saharan African where Ghana is located. This study also found positive associations between the background characteristics and anthropometric measurements such as age, height, weight, BMI and hip circumferences of both male and female with HTN as elaborated in .
Additionally, age and gender (female) were also found to have positive associations on knowledge of HTN as well. Age and gender have been recognized as causal factors for HTN and CVDs in general and has been a central part of virtually all currently recognized risk algorithms for cardiac ailments,Citation18,Citation19 and this study conforms to those existing literature. This study gives a clear and concise background on the knowledge of people who could be classified as “the future of the nation” toward HTN and depicts a high gap on knowledge. Majority, 63.1%, have “No idea” and 40.9% of participants “Don’t know” what HTN is and the causes of HTN respectively. Studies have shown that gaps in knowledge in the form of health literacy are key hindrances to effectively avoid and treat HTN, as these permits individuals to progress on outcomes of their health.Citation10,Citation11 Having access to excellent information on health also improves knowledge on its management and control and this is on HTN as well.Citation20 High knowledge on HTN at this stage in the lives of participants may go a long way to help decrease the future prevalence within Ghana and Africa as a whole since situations may not be very different in other parts of the continent.
This study, however, further found age, gender (female), not doing physical exercises at all, not adding extra salt, fast and homemade foods as risks factors with positive associations to knowledge on HTN among its respondents. There were no positive associations on HTN and BMI, HTN and male gender and hip circumference on Knowledge of HTN. Interestingly, though dietary salt is related to HTN,Citation21 this study rather demonstrated otherwise disputing association of salt and hypertension, suggesting a probable relation of salt and hypertension in older ages rather than in the adolescents. It also found a positive association between both fast and homemade foods regularly consumed by participants. Ghanaian youths have the habits of consuming more carbohydrates, proteins and fats, and this can alter blood pressure.Citation22 Although BMI and hip circumferences have been found as predictors to HTN,Citation23 this current study did not find such an association though it is not disputing the facts of existing literature. Also, the study realized a positive relation between no physical activity and hypertension, which confirms existing literature of recommending physical reduction of HTN among risk population and hypertensive patients.Citation24,Citation25
Conclusion
The study has unveiled the prevalence of hypertension in its different stages. As well as knowledge, and risk factors of pre-HTN and HTN in an adolescent population that had not been targeted. This study indicates an educational intervention program on HTN, its prevalence and risks in the educational curriculum. Educating Domestic Bursars and Matrons who oversee feeding students in various schools in the Ghana education services on such topics is also warranted.
The major limitation of the study was first, the Blood Pressure measured was performed one’s to confirm the diagnosis, whereas standard practice is to do it in at least three instances. Second, the sample location was mainly in Ashanti, a region in Ghana in public schools. This may not be a true representation of the country’s population. Third, Field S2019 which we undertook had no probing questions but with yes or no type of questions.
Availability of data
All data analyzed for this article are included in the published paper. All other documents and data are available with the corresponding author and can be released on reasonable request.
Author contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Acknowledgments
The authors wish to recognize the Ashanti Regional Director of Education (Mrs. Mary Owusu Achiaw) and workers of the Ghana Education Services in the Ashanti region for their support. The authors also wish to thank nurses and doctors of Akomaa Memorial Hospital, Bekwai-Kortwia especially Mr. Stephen Kwarteng Frimpong and Mr. James Govina of Center for Scientific Institute of Research (CSIR) KNUST for their immense contribution to the script and collection of data.
Disclosure
The authors report no conflicts of interest in this work.
References
- Nahimana M-R , Nyandwi A , Muhimpundu AM , et al. A population-based national estimate of the prevalence and risk factors associated with hypertension in Rwanda: implications for prevention and control. BMC Public Health . 2017;18:2. doi:10.1186/s12889-017-4536-9 28693458
- Hien HA , Tam NM , Tam V , Derese A , Devroey D . Prevalence, awareness, treatment, and control of hypertension and its risk factors in (Central) vietnam. Int J Hypertens . 2018;2018:1–12. doi:10.1155/2018/6326984
- van de Vijver SJM , Oti SO , Agyemang C , Gomez GB , Kyobutungi C . Prevalence, awareness, treatment and control of hypertension among slum dwellers in Nairobi, Kenya. J Hypertens . 2013;31:1018–1024. doi:10.1097/HJH.0b013e32835e3a56 23425703
- Guwatudde D , Mutungi G , Wesonga R , et al. The epidemiology of hypertension in Uganda: findings from the national non-communicable diseases risk factor survey. PLoS One . 2015;10:e0138991. doi:10.1371/journal.pone.0138991 26406462
- Yeboah EA . Dietary Factors Associated with Hypertension among Adults in Asesewa in the Upper Manya Krobo District . Available from: http://ugspace.ug.edu.gh/browse?type=author&value=Yeboah%2C+E.A. Accessed 15 July, 2019.
- Agyemang, C. , Attah-Adjepong, G , Ewusu-Dabo, E , et al. Stroke in Ashanti region of Ghana. Ghana Med J . 2012;46:12–17.23661812
- Agyei-Baffour P , Tetteh G , Quansah DY , Boateng D . Prevalence and knowledge of hypertension among people living in rural communities in Ghana: a mixed method study. Afr Health Sci . 2018;18:931–941. doi:10.4314/ahs.v18i4.12 30766557
- Sanuade OA , Boatemaa S , Kushitor MK . Hypertension prevalence, awareness, treatment and control in Ghanaian population: evidence from the Ghana demographic and health survey. PLoS One . 2018;13:e0205985. doi:10.1371/journal.pone.0205985 30403686
- Falkner B . Prehypertension in adolescents: how high is the risk for hypertension? J Pediatr . 2012;160:7–9. doi:10.1016/j.jpeds.2011.08.050 21982301
- Jolles EP , Clark AM , Braam B . Getting the message across. J Hypertens . 2012;30:1500–1510. doi:10.1097/HJH.0b013e32835476e1 22635137
- Poureslami I , Nimmon L , Rootman I , Fitzgerald MJ . Health literacy and chronic disease management: drawing from expert knowledge to set an agenda. Health Promot Int . 2016;32:daw003. doi:10.1093/heapro/daw003
- Kilic M , Uzunçakmak T , Ede H . The effect of knowledge about hypertension on the control of high blood pressure. Int J Cardiovasc Acad . 2016;2:27–32. doi:10.1016/j.ijcac.2016.01.003
- [No authors listed]. Report of the second task force on blood pressure control in children–1987. Task force on blood pressure control in children. National Heart, Lung, and Blood Institute, Bethesda, Maryland. Pediatrics . 1987;79:1–25.3797155
- Anyaegbu EI , Dharnidharka VR . Hypertension in the teenager. Pediatr Clin North Am . 2014;61:131–151. doi:10.1016/j.pcl.2013.09.011 24267462
- Dzudie A , Rayner B , Ojji D , et al. Roadmap to achieve 25% hypertension control in Africa by 2025. Cardiovasc J Afr . 2017;28:262–272. doi:10.5830/CVJA-2017-040 28906541
- Cuddy MLS . Treatment of hypertension: guidelines from JNC 7 (the seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure 1). J Pract Nurs . 2005;55:17–21; quiz 22–3.
- Gyamfi D , Obirikorang C , Acheampong E , et al. Prevalence of pre-hypertension and hypertension and its related risk factors among undergraduate students in a Tertiary institution, Ghana. Alexandria J Med . 2018;54:475–480. doi:10.1016/j.ajme.2018.02.002
- Agyemang C . Rural and urban differences in blood pressure and hypertension in Ghana, West Africa. Public Health . 2006;120:525–533. doi:10.1016/j.puhe.2006.02.002 16684547
- Agyemang C , Redekop WK , Owusu-Dabo E , Bruijnzeels MA . Blood pressure patterns in rural, semi-urban and urban children in the Ashanti region of Ghana, West Africa. BMC Public Health . 2005;5:114. doi:10.1186/1471-2458-5-49 16262905
- Bigi, M. A. B. , Zibaeenezhad, MJ , Aghasadeghi K , Jokar A , Shekarforoush S , Khazraei H . The effect of educational programs on hypertension management. Int Cardiovasc Res J . 2017;8;1.
- Frisoli TM , Schmieder RE , Grodzicki T , Messerli FH . Salt and hypertension: is salt dietary reduction worth the effort? Am J Med . 2012;125:433–439. doi:10.1016/j.amjmed.2011.10.023 22482843
- Hodges RE , Rebello T . Carbohydrates and blood pressure. Ann Intern Med . 1983;98:838–841. doi:10.7326/0003-4819-98-5-838 6405669
- Roka R , Michimi A , Macy G . High blood press. Cardiovasc Prev . 2015.23(3);265.
- Diaz KM , Shimbo D . Physical activity and the prevention of hypertension. Curr Hypertens Rep . 2013;15:659–668. doi:10.1007/s11906-013-0386-8 24052212
- Börjesson M , Onerup A , Lundqvist S , Dahlöf B . Physical activity and exercise lower blood pressure in individuals with hypertension: narrative review of 27 RCTs. Br J Sports Med . 2016;50:356–361. doi:10.1136/bjsports-2016-096014 26787705