Abstract
Introduction
International recommendations of the exploration of non-insulin-dependent diabetes mellitus (NIDDM) are focused on deficiency and not incapacity.
Aims
(1) To estimate the incapacity of NIDDM patients through the 6-minute walk test (6MWT) data. (2) To determine their 6-minute walk distance (6MWD) influencing factors (3) To compare data of NIDDM patient group (PG; n = 100) with those of two control groups (CG): CG1 (n = 174, healthy nonobese and nonsmoker); CG2 (n = 55, obese nondiabetic free from comorbidities).
Population and methods
The anthropometric, socioeconomic, clinical, metabolic, and 6MWT data of 100 NIDDM patients (45 females) were collected.
Results
Total sample means ± standard deviation of age, weight, and height were 54 ± 8 years, 81 ± 14 kg, and 1.64 ± 0.09 m. (1) Measured 6MWD (566 ± 81 m) was significantly lower than the theoretical 6MWD (90% ± 12%). The profile of the PG carrying the 6MWT, was as follows: 23% had an abnormal 6MWD; at the end of the 6MWT, 21% and 12% had, respectively, a low heart rate and a high dyspnea (>5/10), and 4% had desaturation during the walk. The estimated “cardiorespiratory and muscular chain” age (68 ± 16 years) was significantly higher than the chronological age. (2) The factors that significantly influenced the 6MWD (r 2 = 0.58) are included in the following equation: 6MWD (m) = −73.94 × gender (0, male; 1, female) – 3.25 × age (years) + 7.33 × leisure activity score – 35.57 × obesity (0, no; 1, yes) + 32.86 × socioeconomic level (0, low; 1, high) – 27.67 × cigarette use (0, no; 1, yes) + 8.89 × resting oxyhemoglobin saturation – 105.48. (3) Compared to the CGs, the PG had a significantly (P < 0.05) lower 6MWD (100%+9% and 100%+8%, respectively, for the CG1 and CG2).
Conclusion
NIDDM seems to accelerate the decline of the submaximal aerobic capacity evaluated through the 6MWD.
Introduction
The Maghreb (region of Northwest Africa comprising five countries: Tunisia, Morocco, Algeria, Libya, and Mauritania) is undergoing an epidemiological transition characterized by a decrease of infectious diseases and an increase in chronic noninfectious ones.Citation1 This increase is largely due to a marked change in lifestyle (sedentary lifestyle, obesity, and stress of urbanization and labor), including changes in food consumption patterns.Citation1 Among noninfectious chronic diseases, non-insulin-dependent diabetes mellitus (NIDDM), a disease marked by expansion over the past decade, is becoming a real public health emergency.Citation2 For example, its prevalence in North Africa is estimated at 10%.Citation3 NIDDM poses a major public health problem, more particularly with the cardiovascular complications it causes (myocardial infarction [MI], occlusion of arteries of lower limbs, stroke).Citation1,Citation3
To better explore this killer disease, it would be interesting to refer to the World Health Organization’s latest classification of the natural history of chronic diseases, reporting three evolutionary stages:Citation4 deficiency, incapacity, and social disadvantage. The evaluation of incapacity (clinically characterized by dyspnea, pain in the lower limbs, and intermittent claudicationCitation3,Citation5) is considered essential, because alone it can predict the future functioning of the patient.Citation6 This is the determination of exercise tolerance through, for example, data from a field test such as the 6-minute walk test (6MWT), which explores the cardiorespiratory and muscle chain.Citation6 The social disadvantage is the psychosocial impact of the disease. This is the assessment of the quality of life (QOL).
Internationally, several recommendations for NIDDM management have been developed by scientific societies.Citation5,Citation7–Citation11 These recommendations mainly focus on the exploration of deficiency (blood tests [glucose, glycated hemoglobin {HbA1c}, lipid profile, microalbuminuria, renal function], blood pressure). These explorations are conducted for static diagnostic purposes or to detect degenerative complications. However, none of these societies recommend the exploration of incapacity,Citation5,Citation7–Citation11 while two recent studiesCitation12,Citation13 have shown that NIDDM significantly alters submaximal aerobic capacity. These two studies unfortunately have methodological shortcomings: inclusion of patients with NIDDM and heart failureCitation13 or inclusion of only very elderly patients.Citation12
The assessment of functional incapacity, for example, through 6MWT data (endurance test, intensity moderately higher than daily living activitiesCitation6,Citation14), is desirable. Indeed, the skill of walking is a reflection of the ability to maintain a number of daily-life activities for patients.Citation6 Therefore, it is an important QOL component.Citation6
Hence the aims of our study, done in NIDDM patients living in Northwest Africa, are:
To estimate the incapacity of NIDDM patients by establishing their profile during the 6MWT: number of patients having an abnormal 6MWD, and/or stopping while walking, and/or having desaturation, and/or expressing dyspnea at the end of the test, and/or showing impaired chronotropic response.
To determine factors influencing their 6MWD and to compare their chronological and estimated “cardiorespiratory and muscular chain” ages.
To compare data of NIDDM patient group (PG; n = 100) with those of three control groups (CGs): CG1 (n = 174), healthy nonobese and nonsmoker; CG2 (n = 55), nondiabetic obese, free from comorbidities; CG3 (n = 59), nondiabetic “all comers.”
Population and methods
Study design
We performed this cross-sectional study over a 5-month period in Farhat HACHED Hospital’s Physiology and Functional Exploration Department and in the Basic Health Group’s Laboratory of Biochemistry in Sousse (altitude < 100 m), Tunisia.
Approval for the study was obtained from the hospital’s ethics committee, and written consent was obtained from all study participants.
NIDDM patients were recruited in three ways. We contacted general practitioners and/or endocrinology specialists. An article was published in a weekly newspaper announcing the need for recruitment of NIDDM patients. Informational letters clarifying the aims of the study were then put up at the hospital and the local medical school.
NIDDM patient group
Only patients aged over 40 years with an NIDDM status for more than 5 years were included. Noninclusion criteria were as follows: type 1 diabetes, insulin-requiring diabetes; history of orthopedic or surgical disease interfering with walking; recent infection; chronic corticoids use; inability to perform the 6MWT exactly and 6MWT counterindications;Citation6 unstable angina or myocardial infarction during the previous month; resting heart rate ≥ 120 bpm, resting systolic or diastolic pressure, ≥180 mmHg and ≥100 mmHg, respectively.
Sample sizes
NIDDM patient group
Sample size was calculated according to the following predictive equation:Citation15 n = (Z2 × p × q)/Δ2, where n was the number of required NIDDM patients, Z was the 95% confidence level (=1.96), q was equal to 1 – p, Δ was the precision (=10%), and p was the estimation of the 6MWD decline or submaximal aerobic capacity induced by NIDDM. According to studies, 48% (P = 0.48) of older non-disabled diabetic patients at baseline developed functional limitations over a 7-year follow-up.Citation16 The sample size was thus 96.
Control groups
We recruited three CGs over 40 years of age. They were tested in our department over the same period as the PG.
CG1: healthy nonobese and nonsmoker subjects (87 males and 87 females).
CG2: nondiabetic obese subjects free from comorbidities (17 males and 38 females).
These two CGs were recruited as a part of current protocols aiming to evaluate the submaximal exercise capacity of narghile smokersCitation17 and obstructive-sleep-apnea patients.Citation18
CG3: Nondiabetic “all comers” subjects (37 males and 22 females) adressed to our department for 6MWT, indicated as preoperative assessment, or faced with various diseases (especially cardiorespiratory diseases).
Medical and physical activity questionnaires
A medical questionnaire recommended for epidemiological research was used to assess subject characteristics (schooling level [SL] and occupational status, smoking, medical, surgical, and gynecologic-obstetric histories, and medication use).Citation19
Two SLs were defined: low (illiterate, primary education) and high (secondary and university education). Two socioeconomic levels (SEL) were defined according to occupational status:Citation14 low (eg, unskilled worker, jobless) and high (eg, skilled worker, farmer, manager).
Cigarette and narghile usage was evaluated, respectively, in pack-years (PY) and narghile-years (NY).Citation20 Two groups of cigarette (0, no [use <2 PY]; 1, yes [use ≥2 PY]) and narghile (0, no [use <1 NY),]; 1, yes [use ≥1 NY]) users were defined. Narghile (water pipe that enables the smoking of a tobacco preparation burned by charcoal embers; the smoke is cooled by passing through water before being inhaled) use alters lung capacity and therefore cardiorespiratory fitness.Citation21,Citation22
A translated version of the VoorripsCitation23 physical activity questionnaire was filled out by each subject, and household, sporting, and leisure activities were evaluated to yield a total physical activity score (low < 9.4, moderate 9.4–16.5, and high > 16.5).Citation23 According to the total physical activity score, two groups of subjects were defined, one as sedentary (score < 9.4) and one as active (score > 9.4).
Physical examination and parity
Gender (0, male; 1, female) was noted and age (years) was verified by identity cards. Height (±0.01 m) was measured with a height gauge with shoes removed, heels joined, and back straight. Weight (±1 kg) was measured, and the body mass index (BMI, weight/height2, kg/m2) was calculated. The following definitions were adopted:Citation24 underweight (BMI < 18.5), normal weight (BMI 18.5–24.9), overweight (BMI 25.0–29.9), and obese (BMI ≥ 30.0); with three classes: moderated (BMI 30.0–34.9), marked (BMI 35.0–39.9), and extreme (BMI ≥ 40.0). Two patient groups were defined (0, nonobese [BMI < 30]; 1, obese [BMI ≥ 30]).
Parity referred to the number of offspring. Two parity subgroups were identified: low and high (parity < 5 and ≥5, respectively).Citation14
Electrocardiogram (ECG) and absolute cardiovascular disease risk (ACVDR) score
A 12-lead resting ECG was performed at baseline. Left ventricular hypertrophy was retained when the Sokolow–Lyon index was higher than 35 mm.Citation25 The ACVDR is the summation of the risk factors, each one being regarded as binary (present or absent) and having an identical weight (). An abnormal reading was not considered as a reason for excluding patients.
Metabolic data and definitions and diagnosis of NIDDM
Glycemia (mmol/L), total cholesterol (mmol/L), and high-density-lipoprotein cholesterol (HDL-C, mmol/L) were quantified by spectrophotometry. Triglycerides (mmol/L) were quantified by the enzymatic colorimetric method. Low-density-lipoprotein cholesterol (LDL-C, mmol/L) was calculated.Citation26 HbA1c (percentage) was quantified on hemolysed total blood (turbidimetric inhibition immunoassay).
NIDDM diagnosis was done according to international criteria:Citation27 clinical signs of diabetes and randomly measured glycemia ≥ 11.11 mmol/L or glycemia 2 hours after a caused oral hyperglycemia ≥ 11.11 mmol/L or a twice fasting glycemia ≥ 7.00 mmol/L.
The following metabolic definitions were applied. A rate of HbA1c > 7% shows an unbalanced NIDDM during the last 3 months,Citation9 and two groups of patients were identified (0, unbalanced; 1, balanced). Triglycerides ≥ 1.7 mmol/L and/or HDL-C < 1 mmol/L and/or LDL-C ≥ 4.1 mmol/L diagnoses “measured” dyslipidemia,Citation26 and two groups of patients were defined (0, measured dyslipidemia; 1, no measured dyslipidemia).
6MWT procedure, dyspnea evaluation, applied definitions
The 6MWT was conducted according to a standardized protocol.Citation6 The test was conducted along a seldom-traveled, flat, straight corridor (40 m long, marked every 1 m with cones to indicate turnaround points) with a hard surface. To minimize intraday variability, temperature effects, and biological rhythms, the 6MWT was performed between 8 am and 10 am, a period characterized by a stable ambient temperature of 16°C–20°C. All subjects performed the 6MWT for the first time with no warm-up period and no encouragement. Subjects were told to avoid vigorous exercise in the 2 hours prior to testing, to wear comfortable clothes and appropriate walking shoes, and to continue their usual medication.Citation6 The subjects sat in a chair located near the starting position for at least 10 minutes before the test started. During this time, dyspnea (visual analogue scale [VAS]), heart rate, and oxyhemoglobin saturation (oxy-sat) (finger pulse oximeter; Nonin Medical, Minneapolis, MN) and systolic and diastolic pressures (SP, DP, respectively) were measured at rest (rest). The test instructions to the subjects were those recommended by the American Thoracic Society.Citation6 At the end (end) of the 6MWT, the same data, in addition to 6MWD, were measured. Recommended reasons for immediately stopping the 6MWT include the following: chest pain, intolerable dyspnea, leg cramps, staggering, diaphoresis, and pale or ashen appearance.Citation6 In addition to 6MWD (m, %), dyspnea, SP and DP (mmHg), heart rate (bpm, % of predicted maximal heart rate [= 208 – 0.7 × age]), oxy-sat, delta oxy-sat [Δoxy-sat = oxy-sat{rest–end}], and the number of stops during the 6MWT were noted/calculated. The 6MWD reference values were calculated according to local norms:Citation14 6MWD (m) = 720.50 – 160.27 × gender (0, male; 1, female) – 5.14 × age (years) – 2.23 × weight (kg) + 272.00 × height (m).
Since the 6MWT evaluates the integrated answer of the cardiorespiratory and muscular chain,Citation6 we calculated the “estimated age” of this chain:Citation14 estimated “cardiorespiratory and muscular chain” age (years) = 140.1751 – 0.1945 × measured 6MWD (m) – 31.1809 × gender (0, male; 1, female) – 0.4338 × weight (kg) + 52.9183 × height (m).
Dyspnea during the 6MWT was evaluated by VAS, which allows an easy evaluation of exercise dyspnea.Citation28 It is about an open segment whose two ends are the absence of breathlessness and the maximum breathlessness. It was built on a slate for writing with dry erasable felt. Subjects read a standardized text in Arabic explaining dyspnea (or were read to, if they were illiterate) before each 6MWT. At the beginning and right at the end of the 6MWT, the subject indicated his level of breathlessness by marking with his index finger a vertical feature on the VAS. Dyspnea was then quantified from zero (no breathlessness) to ten (maximum of breathlessness).
The following definitions were applied:
A 6MWD lower than 82% was considered a “clinically significant abnormal value” and showed walk intolerance.Citation29
Stopping during the 6MWT was regarded as an intolerance sign.Citation14
A Δoxy-sat > 5 points defines a “clinically significant desaturation.”Citation14
Any dyspneaend > 5/10 was considered as “clinically significant” and showed walk intolerance.Citation28
A heart rateend < 60% was considered a chronotropic insufficiency.Citation14
Study conduct
First visit (day 1): presentation of the patient to the Physiology Department, signature of consent, medical and physical activity questionnaires, anthropometric data, and baseline ECG.
Second visit (day 2): fasting blood sample, food intake (a cup of mineral water and some dates), VAS explanation; resting dyspnea, blood pressure, oxy-sat and heart rate, checks of the absence of 6MWT contraindications, 6MWT practice between 8 am and 10 am.
Data analysis
Expression modes of results
The Kolmogorov–Smirnov test was used to analyse distribution of variables.Citation15 When the distribution is normal and the variances are equal, the results are expressed by their means ± standards deviations (SD). If the distribution isn’t normal, the results are expressed by their medians (first–third quartiles). The chi-squared test was used to compare percentages.
NIDDM PG: comparison of 6MWT measured data, univariate and multiple regression analysis (influencing factors)
The dependent variable (6MWD) was normally distributed. Student’s t-test was used to compare measured versus theoretical 6MWD, resting versus 6MWTend data, and to evaluate the associations between measured 6MWD (m) and categorical variables (0, no; 1, yes) for cigarette or narghile use, chronic respiratory disease, arterial hypertension, dyslipidemia, cardiovascular diseases, thyroid dysfunction, diabetic retinopathy, history of abdominopelvic and/or thoracic and/or neurological surgeries, beta-blocker or diuretic use, sedentary status, obesity group, diabetes balance, measured dyslipidemia, and left ventricular hypertrophy; (0, low; 1, high) for SEL, SL, parity, and (0, male; 1, female) for gender.
Pearson product-moment correlation (r) evaluated the associations between the measured 6MWD (m) and continuous measures (physical activity score, age [years], weight [kg], height [m], BMI [kg/m2], parity [numerical], fasting glycemia [mmol/L], HbA1c [%], triglycerides [mmol/L], total cholesterol [mmol/L], HDL-C [mmol/L], LDL-C [mmol/L], ACVDR score, dyspnearest, heart raterest [bpm], SPrest [mmHg], DPrest [mmHg], and oxy-satrest [%]). The linearity of the association between the 6MWD and the continuous measures was graphically checked by plotting each regressor against 6MWD. Only significantly and linearly associated variables were entered into the model.
A linear regression model was used to evaluate the independent variables explaining the variance in 6MWD. Candidate variables were stepped into the model with a stepwise selection method. To determine entry and removal from the model, significance levels of 0.15 and 0.05, respectively, were used. No colinearity between predictors was detected with variance inflation factors. The linear regression equation model is the following: 6MWD (m) = B1 × categorical variable1 + B2 × categorical variable2 + Bn × categorical variablen + B × 1 × continuous variable1 + B × 2 × continuous variable2 + B × n × continuous variablen + constant. B is the nonstandardized regression coefficient.
Comparison of NIDDM PG versus CG data
t-tests and chi-squared tests were used to compare quantitative data and percentages, respectively. In the same way, an analysis of variance was carried out between the four groups.
Analyses were carried out using Statistica software (Statistica Kernel version 6; StatSoft, Paris, France). Significance was set at the 0.05 level.
Results
Patient group: noninclusion criteria, clinical, anthropometric, and metabolic characteristics
An initial sample of 123 volunteer adults was examined. Noninclusion criteria, presented in detail in the Appendix, were found in 23 subjects.
exposes the clinical, anthropometric, and metabolic characteristics of the NIDDM PG. Compared to males, there are significantly fewer female cigarette or narghile users, more females having thyroid dysfunction or with surgical history, or having low SEL, SL, or having sedentary status, there are fewer overweight females, but a higher percentage of obese females. Compared to males, females have a significantly higher BMI and LDL-C level, a lower ACVDR score and are significantly shorter.
Table 1 Clinical, anthropometric, and metabolic characteristics of the non-insulin-dependent diabetes mellitus patient group
The 6MWD of the 45 females and 55 males, according to age-group, is shown in . Few older patients aged 65 years and more are included (four females and four males).
Additional information about the PG total sample characteristics are detailed in the Appendix.
PG: 6MWT data and profile
The 6MWT data are shown in . The total-sample measured 6MWD (566 ± 81 m) was significantly lower than the theoretical one (90% ± 12%). This difference of about 86 m was observed only in males. For females, males, and total sample, and compared to resting data, there was a significant increase in 6MWTend SP, DP, and dyspnea. Oxy-sat significantly decreased only in males.
Table 2 Six-minute walk test (6MWT) data of the non-insulin-dependent diabetes mellitus patient group
NIDDM patient profile during the 6MWT were as follows: 2% (1% females) stopped once during the 6MWT; 4% (2% females) showed a clinically significant desaturation; 12% (7% females) expressed a clinically significant dyspneaend; 21% (10% females) had a chronotropic insufficiency; and 23% (2% females) had an abnormal 6MWD.
PG: univariate and multiple regression analysis: influencing factors
Gender significantly affected the 6MWD (). On average, the 6MWD values were 96 m greater (significant) in males when compared to females. This difference applies to patients aged between 45 and 60 years and more than 65 years ().
Univariate analysis between 6MWD and patient data is shown in the . In the total sample, the following categorical variables significantly affected the 6MWD: cigarette use, surgical history, SEL, SL, physical activity level, and obesity. In the total sample, 6MWD was significantly correlated (P < 0.05) with the following continuous variables: age; height; BMI; daily, sporting, leisure, and physical activity scores; ACVDR score; SPrest; and oxy-satrest. Several factors did not independently explain the variability of 6MWD, such as metabolic data.
presents the cumulative determination coefficient (r 2) of the independent factors included in the 6MWD forward linear stepwise multiple regressions. For the total sample, gender, age, leisure activity score, obesity, SEL, cigarette use, and oxy-satrest were independent predictors, and up to 58% of the 6MWD variability could be explained with the proposed model in .
Table 3 Independent variables included in the forward linear stepwise multiple regression model for the 6-minute walk distance (6MWD) of the non-insulin-dependent diabetes mellitus patient group
PG: “cardiorespiratory and muscular chain” estimated age
In the total sample, the “cardiorespiratory and muscular chain” estimated age was significantly higher than the chronological age (68 ± 16 years versus 54 ± 8 years, respectively; P < 0.05). This difference existed only in males (76 ± 13 years versus 54 ± 8 years, respectively; P < 0.05).
PG: characteristics of patients distributed according to the 6MWD (normal versus abnormal 6MWD)
presents the characteristics of the two groups of patients with abnormal 6MWD (21 males, 2 females) and normal 6MWD (34 males, 43 females). Compared to the group having a normal 6MWD (94% ± 10%), the group having abnormal 6MWD (76% ± 5%), is significantly younger and taller, contains a significantly higher percentage of patients using cigarettes or having measured dyslipidemia, and has a higher ACVDR score.
Table 4 Characteristics of non-insulin-dependent diabetes mellitus patients, divided according to their 6MWD (Group 1, abnormal 6MWD; Group 2: normal 6MWD)
PG: parity effect
In the entire female population (n = 45), a negative univariate linear correlation was found between parity (numerical) and 6MWD (r = −0.44; P < 0.05), and on average the 6MWD value was 61 m greater in females having low parity (). Parity also appeared to be a negative independent variable included in the forward linear stepwise multiple regression model for 6MWD ().
Comparison of NIDDM PG versus CG data
presents the characteristics of the PG and CGs. Analysis of the total samples 6MWDs revealed that compared to CG1 (636 ± 112 m, 100% ± 9%), to CG2 (100% ± 8%), and to CG3 (507 ± 129 m, 83% ± 14%), the PG (566 ± 81 m, 90% ± 12%) had a significantly lower 6MWD (m, %), lower 6MWD (%), and higher 6MWD (m, %), respectively. Detailed information appears in the Appendix.
Table 5 Comparison of patient group (PG) data with those of three control groups (CG): CG1 (healthy nonobese and nonsmoking); CG2 (nondiabetic obese free from comorbidities); and CG3 (“all comers” – nondiabetics)
Discussion
The 6MWT profile of a large group of NIDDM patients older than 40 years was evaluated. It seems that NIDDM accelerates “cardiorespiratory and muscle chain” aging, with 23% of patients having an abnormal 6MWD. Impaired submaximal aerobic capacity is more pronounced in females and/or in the elderly and/or in subjects having low leisure activity score and/or in obese patients and/or in patients having low SEL and/or in cigarette smokers and/or in subjects having low resting oxy-sat. Compared to healthy nonobese and nonsmoking or nondiabetic obese control groups, NIDDM patients group had a significantly lower 6MWD.
Study design and statistical analysis
Detailed discussion of the recruitment method, the inclusion and noninclusion criteria, the sample size, and the questionnaires used appears in the Appendix. The number of measures and comparisons (n = 36) was too large for the number of participants included in the present study, usually one variable for ten participants.
Justification of the 6MWT choice to evaluate submaximal aerobic capacity
Exercise tolerance is usually expressed in terms of maximal oxygen consumption (V̇O2max) measured during a cardiorespiratory test realized under optimal safety conditions and in the presence of a physician and a technician.Citation30 However, the cardiorespiratory test has some drawbacks. First, it uses expensive and sophisticated equipment, demanding that it be operated by highly qualified personnel.Citation6 Thus the repeated use of such a test for assessment of exercise training represents a significant financial cost.Citation6,Citation31 Second, the complexity of the examination and its interpretation does not allow the patient to have a quick and convenient representation of its progress.Citation6 Finally, this test can’t be done on a large scale.Citation6 These drawbacks lead us to turn to the tests called “low-tech,” such as the 6MWT (reliable, valid, safe, inexpensive, feasible on a large scale, can be performed by a physician, or a nurse, physiotherapist, or teacher of adapted physical activities). It is used to assess exercise tolerance not only of chronic respiratory diseases but also those with heartCitation32 or metabolicCitation12,Citation13 diseases. Another justification for our choice is that the 6MWT quantifies the ability to perform activities of daily life, familiar to subjects, and therefore supports the idea of submaximal activity. Finally, it is preferable to start as part of the assessment of exercise tolerance, by the practice of 6MWT and in case of an abnormal 6MWD, the cardiorespiratory test is largely indicated.Citation6
Precautions taken during 6MWT
The 6MWT was performed in the open air in a corridor of 40 m length.Citation6 Enright et al,Citation12 and Ingle et al,Citation13 used, respectively, corridors of 30 m and 15 m. Detailed discussion of the precautions taken during the 6MWT appears in the Appendix.
Characteristics of NIDDM PG
Our NIDDM sample can be considered as representative of the Northwest African population with NIDDM. Indeed, in our study, the frequency of risk factors and certain comorbidities observed were similar to those reported in other studies ().
Limitations of this study
In females, menopause and changes in hormonal status that may affect aerobic capacityCitation33 haven’t been evaluated. Passive smoking has not been studied despite its adverse effects on exercise capacity, particularly as it reduces the lungs’ performance.Citation34 We didn’t measure quadriceps strength or the leg length, known as 6MWD-influencing factors.Citation29 In this study, we evaluated NIDDM patient deficiency by determining fasting glycemia, HbA1c, lipid profile, blood pressure, and ACVDR score. However, there are other biological markers such as oxidative stress, inflammation, and apoptosis,Citation35–Citation40 which may cause disabilities through myopathy.Citation41 Similarly, it was desirable to measure some morphological data (lower-limb length,Citation29 muscle biopsy data,Citation41 or lung functionCitation42). As part of exploration of incapacity, it was desirable to achieve in a number of our patients a cardiorespiratory test and to evaluate the correlation between V̇O2 max and 6MWD. As part of the exploration of social disadvantage, it was desirable to explore the QOL of our patients. However, to our knowledge, there is no validated Arabic version of the QOL questionnaire specific to NIDDM patients.Citation43
Deterioration of submaximal aerobic capacity
Submaximal aerobic capacity of NIDDM patients seems to have deteriorated. Indeed, the measured 6MWD was 86 m less than the predicted one. In addition, almost one-quarter of our NIDDM patients had an abnormal 6MWD. Similarly, there were signs of walking intolerance (2% and 12% of patients stopped the walk and expressed a clinically significant dyspneaend, respectively). Finally, compared to healthy nonobese, nonsmokers and nondiabetic obese CGs, the PG had a significantly lower 6MWD.
Another key outcome of the present study is that the NIDDM accelerates the “cardiorespiratory and muscle chain” aging. It is an unwavering argument to motivate patients to better compliance with preventive and therapeutic measures. To our knowledge, this result has never been shown before.
Twenty-one percent of our patients had an impaired chronotropic heart response. This reflects the impact of NIDDM on the activity of the sinus node during the walk.Citation44 Moreover, the ACVDR score of the group with abnormal 6MWD was significantly higher than the group with normal 6MWD (). This is an important argument to encourage patients with NIDDM to start regular exercise.Citation45 Indeed, the exercise training and aerobic capacity were positively related to cardiovascular profile.Citation45
To our knowledge, only two studies have examined the submaximal aerobic capacity of NIDDM patients.Citation12,Citation13 The first study, conducted in 2003 by Enright et al,Citation12 aimed to establish 6MWD norms specific to the US population aged 68 years and more (n = 2117 subjects, 13% had NIDDM). The multiple linear regression model revealed that the NIDDM was an independent predictor that altered the 6MWD.Citation12 These authors recommended the 6MWT to assess the impact of NIDDM and other comorbidities (cardiovascular or respiratory diseases, arthritis, cognitive dysfunction, depression, etc) on elderly submaximal aerobic capacity.Citation12 The second study, a retrospective one, conducted in 2006 by Ingle et al,Citation13 compared the 6MWD of four matched groups of patients (no statistical difference in age or gender): “heart failure with NIDDM” (n = 88) versus “heart failure free from NIDDM” (n = 88), “coronary artery disease with NIDDM” (n = 50) versus “coronary heart disease free from heart failure” (n = 50). These authors found that the 6MWD of the “heart failure with NIDDM” group (238 ± 124 m) was significantly lower than the 6MWD of the “heart failure free from NIDDM” (296 ± 131 m) and that the 6MWD of the “heart failure free from NIDDM” group (231 ± 139 m) was significantly lower than the 6MWD of the “coronary heart disease free from heart failure” group (283 ± 126 m).Citation13 These authors found that NIDDM was an independent determinant of low submaximal aerobic capacity.Citation13
How can we explain the impairment of submaximal aerobic capacity of NIDDM patients?
The first important point of the present study is that classical biological data (fasting glycemia, HbA1c, lipid) often used to monitor the development of NIDDM don’t appear as indicators of incapacity ( and ). However, there is evidence that regular physical activity in NIDDM patients is associated with a significant improvement in glycemic control, particularly in HbA1c.Citation45 Moreover, evaluation of NIDDM patient physical training programs is mainly based on the HbA1c changes.Citation46–Citation49
In the total sample (), the alteration of submaximal aerobic capacity is more pronounced in females and/or in the elderly and/or in subjects having a low leisure activity score and/or in obese patients and/or in patients having low socioeconomic level and/or in cigarette smokers and/or in subjects having low oxy-satrest. It is important to note that the suppression of the eight patients aged 65 years and more doesn’t significantly confound the total sample actual results. These factors, in addition to parity, will be analyzed one by one in the following sections.
Effect of gender
As in some healthyCitation14,Citation29 or patientCitation12 adult populations, we found that females compared to males have a lower 6MWD ( and ). One plausible explanation is that muscle mass and therefore maximum leg-muscle force is lower for females than males.Citation50 Another plausible explanation is parity, known as a physiological factor, accelerating the healthy female’s 6MWD decline.Citation14 Indeed, among NIDDM females, in addition to age and SEL, parity appears to be an independent factor influencing 6MWD (). Among healthy women aged more than 40 years, the 6MWD decreased by 9.58 m when parity increased by one unit (r = −0.39, P < 0.05).Citation14 In our study, NIDDM accelerated this decline, since the 6MWD of NIDDM female subjects decreased by 13.38 m when parity increased by one unit (r = −0.44, P < 0.05).
Effect of age
As in most studies of healthyCitation14,Citation29 or patientCitation51 adult populations, we found that age is a predictor of 6MWD decline. The potential physical decrease observed with aging is partly due to reduced muscle mass, strength, and endurance, thus defining sarcopenia.Citation14 Indeed, from 40 years of age, muscle mass decreases by an average of 5% per decade.Citation50
Effect of physical inactivity
Physical inactivity significantly influences healthy subjects’ 6MWD, which decreased by 2.30 m when the physical activity score decreased by one point.Citation25 This decrease was more pronounced in NIDDM patients,Citation52 since patients with low leisure-activity scores (sedentary status) had a lower 6MWD by of 7.33 m (). This result is an important argument to encourage NIDDM patients to start regular exercise.Citation40
Effect of obesity
Obesity, especially the marked type, is predictive of 6MWD decline.Citation6,Citation29 Indeed, some authorsCitation14 have shown that healthy subjects’ 6MWD decreases by about 6 m when the BMI increases by one unit. In our study, being obese reduced 6MWD by 35.57 m (). This confirms once more the adverse effects of obesity on aerobic capacity,Citation6 and suggests that the obesity–NIDDM association accelerates 6MWD decline. This result is an important argument to encourage NIDDM patients to start a diet and/or regular exercise.Citation47
Effect of SEL
In a healthy Tunisian population, the SEL significantly influenced the 6MWD.Citation14 Indeed, having a low SEL decreases the 6MWD by 12.78 m.Citation14 Our study suggests that the onset of NIDDM in subjects having a low SEL accelerates the 6MWD decline since it reaches 32.86 m ().
Effect of smoking
It is well known that smoking causes aerobic capacity alteration.Citation53 In our study, being a cigarette smoker decreased 6MWD by 27.67 m (), and the group with abnormal 6MWD had a significantly higher percentage of cigarette smokers (). This result, which confirms once again the harmful effects of smoking,Citation54 is a very important point to encourage NIDDM patients to stop smoking.
Effect of resting oxy-sat
In our study, the greater the oxy-satrest was, the greater the 6MWD was (). In many chronic diseases, desaturation during a walk is an independent prognostic marker and is associated with a significant risk of mortality.Citation55,Citation56 For example, in pulmonary arterial hypertension, desaturation of more than 10% increased the mortality risk by 2.9.Citation56 In NIDDM, the clinically significant desaturation observed in 4% of our nonsmoking patients free from chronic respiratory diseases can be explained by the impact of diabetes on lung functionCitation42 with impaired alveolar–capillary membrane.Citation42
Effect of parity
6MWD was lower by 61 m in NIDDM females with high parity (). This result may be clinically relevant when interpreting 6MWT in females with NIDDM. A simple way to solve this problem would be to substract 61 m from the theoretical value of these females. This phenomenon may reflect the general findings about aging and parity effects on health.Citation57 In fact, repeated gestations have been found to have potentially noxious effects on health, and several hypotheses, discussed in a previous paper,Citation14 have been advanced (detailed discussion appears in the Appendix). Medical studies provide very little information on the influence of parity on exercise tolerance, however, and this may be a promising new direction for physiological and pathophysiological research, particularly for developing countries.
Other factors explaining the submaximal aerobic capacity decline
The aforementioned factors explain 58% of the total-sample 6MWD variability (), which means that 42% of the variability remains unexplained. What other factors not evaluated in the present study may affect the NIDDM patients’ 6MWD?
As was said in the sixteenth century by Paracelsus (1493–1541), who wrote that “diabetes is a systemic disease caused by the presence of an abnormal product in the blood. This would act on the kidneys and cause polyuria,”Citation58 NIDDM can be considered a general disease with a metabolic starting point, the main pathophysiological mechanism being insulin resistance.Citation27 As part of this systemic disease, we can discuss the myopathy as an altering factor of the submaximal aerobic capacity.Citation41 This could be the result of numerous alterations, the main ones being inflammation,Citation35,Citation37,Citation39 apoptosis,Citation38 oxidative stress,Citation36 abnormal glucose and lipid or oxidative enzymeCitation59 metabolisms, abnormal microcirculation,Citation60 or abnormal type of fiber.Citation52 These factors are discussed in the Appendix.
In conclusion, NIDDM seems to accelerate the decline of the submaximal aerobic capacity evaluated through 6MWT data.
Acknowledgment
The authors would like to thank Professors Bechir Saadaoui, Gouider Jeridi, Koussay Ach, Molka Chedly Chaieb, Monia Zaouali Ajina, and Sonia Rouatbi (Hospital Farhat Hached, Sousse, Tunisia) for their help.
Disclosure
The authors report no conflicts of interest in this work.
References
- Ghannem H Fredj AH Epidemiological transition and cardiovascular risk factors in Tunisia [French] Rev Epidemiol Sante Publique 1997 45 286 292 9380909
- World Health Organization non-insulin-dependent diabetes mellitus [French] Available from: http://www.who.int/entity/mediacentre/factsheets/fs138/fr Accessed January 15, 2012
- Bouguerra R The global diabetes pandemic: the Tunisian experience Eur J Clin Nutr 2007 61 160 165 16900086
- World Health Organization International Classification of Functioning, Disability and Health Geneva WHO 2001 Available from: http://www.who.int/icidh Accessed January 15, 2012
- Rydén L Standl E Bartnik M Guidelines on diabetes, pre-diabetes and cardiovascular diseases: executive summary. The Task Force on Diabetes and Cardiovascular Diseases of the European Society of Cardiology (ESC) and of the European Association for the Study of Diabetes (EASD) Eur Heart J 2007 28 88 136 17220161
- American Thoracic Society ATS statement: guidelines for the six-minute walk test Am J Respir Crit Care Med 2002 16 111 117
- Rodbard H AACE Diabetes mellitus clinical practice guidelines task force Endocr Pract 2007 13 1 31 17613449
- Ahmann A Guidelines and performance measures for diabetes Am J Manag Care 2007 13 41 46
- Home P IDF Clinical Guidelines Task Force Global Guideline for Type 2 Diabetes Brussels International Diabetes Federation 2005
- Neimanis L Paterson M Surveillance for type 2 diabetes and its complications Can Fam Physician 2000 46 72 73 10660789
- American Diabetes Association Screening for type 2 diabetes Diabetes Care 2004 27 11 14
- Enright PL McBurnie MA Bittner V The six-minute walk test: a quick measure of functional status in elderly adults Chest 2003 123 387 398 12576356
- Ingle L Reddy P Clark AL Cleland JF Diabetes lowers six-minute walk test performance in heart failure J Am Coll Cardiol 2006 47 1909 1910 16682322
- Ben Saad H Prefaut C Tabka Z 6-minute walk distance in healthy North Africans older than 40 years: influence of parity Resp Med 2009 103 74 84
- Jenicek M Cleroux R Clinical epidemiology: its evolution and role in clinical practice and research Union Med Can 1985 114 625 632 4060341
- Al Snih S Fisher M Raji M Markides K Ostir G Goodwin J Diabetes mellitus and incidence of lower body disability among older Americans J Gerontol A Biol Sci Med Sci 2005 60 1152 1156 16183955
- Ben Saad H Babba M Boukamcha R Submaximal exercise capacity and quality of life in exclusive water-pipe smokers Rev Mal Respir 2010 27 489 495 20569882
- Abdelghani A Ben Saad H Ben Hassen I Evaluation of the deficiency and the submaximal exercise capacity in obstructive sleep apnoea patients Rev Mal Respir 2010 27 266 274 20359621
- Ferris BG Epidemiology standardization project II: recommended respiratory disease questionnaires for use with adults and children in epidemiological research Am Rev Respir Dis 1978 118 7 52 354446
- Ben Saad H Khemiss M Bougmiza I Spirometric profile of narghile smokers Rev Mal Respir 2011 28 e39 e51 21943546
- Ben Saad H The narghile and its effects on health. Part I: the narghile, general description and properties Rev Pneumol Clin 2009 65 369 375 19995660
- Ben Saad H The narghile and its effects on health. Part II: the effects of the narghile on health Rev Pneumol Clin 2010 66 132 144 20413049
- Voorrips LE Ravelli AC Dongelmans PC Deurenberg P Van Staveren WA A physical activity questionnaire for the elderly Med Sci Sports Exerc 1991 23 974 979 1956274
- World Health Organization Obesity: Preventing and Managing the Global Epidemic Geneva WHO 1997 3 5
- Assmann G Cullen P Schulte H Simple scoring scheme for calculating the risk of acute coronary events based on the 10-year follow-up of the prospective cardiovascular Münster (PROCAM) study Circulation 2002 105 310 315 11804985
- Okada M Matsui H Ito Y Fujiwara A Inano K Low-density lipoprotein cholesterol can be chemically measured: a new superior method J Lab Clin Med 1998 132 195 201 9735925
- American Diabetes Association Diagnosis and classification of diabetes mellitus Diabetes Care 2005 28 Suppl 1 37 42
- Sergysels R Hayot M Evaluation of exercise-induced dyspnea Rev Pneumol Clin 1997 53 278 282 9616842
- Troosters T Gosselink R Decramer M Six minute walking distance in healthy elderly subjects Eur Respir J 1999 14 270 274 10515400
- Seyoum B Estacio RO Berhanu P Schrier RW Exercise capacity is a predictor of cardiovascular events in patients with type 2 diabetes mellitus Diab Vasc Dis Res 2006 3 197 201 17160916
- Ziegler O Filipecki J Girod I Guillemin F Development and validation of a French obesity-specific quality of life questionnaire: quality of life, obesity and dietetics (QOLOD) rating scale Diabetes Metab 2005 31 273 283 16142018
- Guyatt GH Sullivan MJ Thompson PJ The 6-minute walk: a new measure of exercise capacity in patients with chronic heart failure Can Med Assoc J 1985 132 919 923 3978515
- Altunkeser BB Ozdemir K Içli A Celik C Akyürek C Gök H Effects of long-term hormone replacement therapy on QT and corrected QT dispersion during resting and peak exercise electrocardiography in post-menopausal women Jpn Heart J 2002 43 1 7 12041885
- Frette C Barett-Connor E Clausen JL Effect of active and passive smoking on ventilatory function women Am J Epidemiol 1996 143 757 65 8610685
- Qi L Rifai N Hu FB Interleukin-6 receptor gene, plasma C-reactive protein, and diabetes risk in women Diabetes 2009 58 275 278 18852330
- Baynes JW Role of oxidative stress in development of complications in diabetes Diabetes 1991 40 405 412 2010041
- Bastard JP Maachi M Lagathu C Recent advances in the relationship between obesity, inflammation and insulin resistance Eur Cytokine Netw 2006 17 4 12 16613757
- Kusminski CM Shetty S Orci L Unger RH Scherer PE Diabetes and apoptosis: lipotoxicity Apoptosis 2009 14 1484 1495 19421860
- Remels AH Langen R Gosker HR PPARgamma inhibits NF–kappaB–dependent transcriptional activation in skeletal muscle Am J Physiol Endocrinol Metab 2009 297 174 183
- Nojima H Watanabe H Yamane K Effect of aerobic exercise training on oxidative stress in patients with type 2 diabetes mellitus Metabolism 2008 57 170 176 18191045
- Sun Z Liu L Liu N Liu Y Muscular response and adaptation to diabetes mellitus Front Biosci 2008 13 4765 4794 18508544
- Ozşahin K Tuǧrul A Mert S Yüksel M Tuǧrul G Evaluation of pulmonary alveolo-capillary permeability in type 2 diabetes mellitus: using technetium 99 mTc-DTPA aerosol scintigraphy and carbon monoxide diffusion capacity J Diabetes Complications 2006 20 205 209 16798470
- El Achhab Y Nejjari C Chikri M Lyoussi B Disease-specific health-related quality of life instruments among adults diabetic: a systematic review Diabetes Res Clin Pract 2008 80 171 184 18279993
- Brismar T Abnormal Na-currents in diabetic rat nerve nodal membrane Diabet Med 1993 10 Suppl 2 110 112 8458186
- Thomas DE Elliott EJ Naughton GA Exercise for type 2 diabetes mellitus Cochrane Database Syst Rev 2006 3 CD002968 16855995
- Baldi JC Snowling N Resistance training improves glycaemic control in obese type 2 diabetic men Int J Sports Med 2003 24 419 423 12905089
- Dunstan DW Puddey IB Burke V Stanton KG Morton AR Beilin LJ Effects of a short-term circuit weight training program on glycaemic control in NIDDM Diabetes Res Clin Pract 1998 40 53 61 9699091
- Dunstan DW Daly RM Owen N High-intensity resistance training improves glycemic control in older patients with type 2 diabetes Diabetes Care 2002 25 1729 1736 12351469
- Tessier D Ménard J Fülöp T Effects of aerobic physical exercise in the elderly with type 2 diabetes mellitus Arch Gerontol Geriatr 2000 31 121 132 11090907
- Åstrand PO Rodahl K Lacour JR Duizabo D Handbook of Exercise Physiology 3rd ed Paris Elsevier Masson 1994 245
- Guyatt GH Townsend M Keller J Singer J Nogradi S Measuring functional status in chronic lung disease: conclusions from a random control trial Respir Med 1991 85 Suppl B 17 21 1759016
- Marin P Anderson B Krotkiewski M Björntorp P Muscle fiber composition and capillary density in women and men with NIDDM Diabetes Care 1994 17 382 386 8062604
- Tchissambou BP Massamba A Babela JR Mouanou JK Mboussa J Senga P The effects of smoking and the degree of nicotine dependence on aerobic capacity in sportsmen Rev Mal Respir 2004 21 59 66 15260039
- Berlin I Smoking-induced metabolic disorders: a review Diabetes Metab 2008 34 304 314
- Lama VN Flaherty KR Toews GB Prognostic value of desaturation during a 6-minute walk test in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003 168 1084 1090 12917227
- Paciocco G Martinez FJ Bossone E Pielsticker E Gillespie B Rubenfire M Oxygen desaturation on the 6-MWT and mortality in untreated primary pulmonary hypertension Eur Respir J 2001 17 647 652 11401059
- Hart DA Reno C Pregnancy alters gene expression in normal synovium: influence of age and parity J Rheumatol 1999 26 1775 1784 10451077
- The Archidoxes of Magic by Theophrastus Paracelsus, translated by Robert Turner. Facsimile reprint of the 1656 edition with introduction by Stephen Skinner, Ibis Publishing, 2004.
- Simoneau J Kelley D Altered glycolytic and oxidative capacities of skeletal muscle contribute to insulin resistance in NIDDM J Appl Physiol 1997 83 166 171 9216960
- Mercier J Peripheral muscles and metabolic diseases [French] Rev Mal Respir 2001 18 Suppl 2 S22 S24 11480110
Appendix:
Supplementary data
Results
Noninclusion criteria were found in 23 subjects: diabetes insulin-requiring (n = 15) or evolving less than 5 years (n = 4); nondiabetic subjects (n = 3); and type 1 diabetics (n = 1).
NIDDM PG: clinical, anthropometric and metabolic characteristics
The median (first–third quartiles) of NIDDM evolution was 9 (7–12) years, and 93% of patients were treated by oral antidiabetic medication. The means ± SD of cigarette and narghile use were 20 ± 13 PY and 29 ± 41 NY, respectively. The mean ± SD of arterial hypertension evolution was 8 ± 6 years. All patients with a history of dyslipidemia, thyroid dysfunction, or diabetic retinopathy were treated. History of chronic respiratory diseases included tuberculosis (n = 5), asthma and/or atopy (n = 4), and obstructive sleep apnea (n = 1). History of chronic cardiovascular diseases included MI (n = 3), arrhythmia (n = 2), angina pectoris (n = 1), and arteritis of the lower extremities (n = 1). History of surgery included abdominopelvic (n = 22), thoracic (n = 2), and neurological (n = 1) surgery. Fifty percent and 20% of patients had low and high physical activity scores, respectively.
Comparison of NIDDM PG versus CG data
Analysis of the total-sample data revealed the following points.
Compared to CG1, the PG had significantly higher quantities of used cigarettes and narghile; had a significantly higher percentage of cigarette and narghile users; had a significantly higher physical activity score, weight and BMI; had a significantly lower percentage of sedentary subjects or subjects with low SL, and was significantly younger. The 6MWD means (m, %) of PG with cigarette use ≤2 PY (n = 62, 547 ± 86 m, 95% ± 12%) or free from dyslipidemia (n = 33, 567 ± 75 m, 93% ± 11%) were significantly (P < 0.05) lower than those of CG1 (n = 174, 636 ± 112 m, 100% ± 9%). 6MWD multiple regression analysis on CG1 shows that some variables were influencing factors only for the NIDDM PG, not the healthy CG1 (ie, obesity, SEL, cigarette use, and oxy-satrest). This means that those factors were especially important for the NIDDM PG.
Compared to CG2, the PG had a significantly higher quantities of used cigarettes and narghile; had a significantly higher percentage of cigarette and narghile users; had a significantly higher physical activity score; had a significantly lower BMI and had a significantly lower percentage of sedentary or obese subjects or subjects having low-SE. Compared to CG2, the PG was significantly taller.
Compared to CG3, the PG had significantly higher quantities of used cigarettes and narghile; had significantly higher weight; had significantly higher percentage of subjects with surgery history; had a significantly lower BMI and had significantly lower percentages of obese patients or patients with chronic respiratory disease. Compared to CG3, the PG was significantly younger.
Discussion
Study design (recruitment method, inclusion and noninclusion criteria, sample sizes, questionnaires)
Our cross-sectional study was economical, easy to apply, required less time than a longitudinal one, and provided more useful information.Citation1 In the present study, 6MWD values of NIDDM patients were compared with local 6MWD predicted norms,Citation2 and with measured 6MWD in three CGs.
As in any study on volunteers, there was possible bias in selection.Citation4 However, we limited this bias by the use of a medical questionnaire.Citation4
Patients with NIDDM status for less than 5 years weren’t included. It has been shown that NIDDM affects lung function only in the long term.Citation5 Patients aged under 40 were not included for two reasons: the average age of North African NIDDM patients is around 40 years,Citation6 and the 6MWD local norms were established in adults aged 40 and over.Citation2 To avoid potential confounding effects, we did not include patients with type 1 diabetes or with type 2 diabetes requiring insulin. As a precaution, 6MWT contraindications, which increase the risk of arrhythmia or collapse, were applied as noninclusion criteria.Citation7
The sample size of the PG (n = 100) is less important than other studies related to the 6MWT of NIDDM patients, over the age of 68 years (n = 282)Citation8 or with heart failure (n = 256).Citation9 However, our sample size was calculated using a prediction equation.Citation10
The physical activity questionnaireCitation11 – interesting physical activities performed during the last 12 months – is reproducible.
Precautions taken during 6MWT
NIDDM patients were told to continue their usual oral antidiabetic medication, since its use doesn’t affect exercise tolerance.Citation12 Sources of variability caused by the procedure of the 6MWT itself were controlled as much as possible. Indeed, the 6MWT was performed as recommended in the open air in a corridor of 40 m length. A shorter corridor reduces 6MWD, since patients take longer to return.Citation2,Citation7 To minimize intraday variability and the effects of biological rhythms, the 6MWT were made in the morning (8 am to 10 am).Citation7 Similarly, we avoided encouragement known to increase 6MWD.Citation7
Effect of parity
Effect of parity on the 6MWD can be explained by several hypotheses. First, hormonal alterations during pregnancy could generate aerobic system incapacity.Citation13 As the 6MWT solicits the aerobic system,Citation7 repeated gestations may accentuate or prolong this incapacity. Biochemical modifications were also suggested, since increased oxidative stress has been found during pregnancy.Citation14 With repeated gestations, the repeated oxidative stress could have negative effects on muscle function, explaining in part the 6MWD decline with high parity. Lastly, impaired respiratory muscle function is associated with high parity,Citation15 which may have influenced the ventilatory response in our subjects during exercise.
Other factors explaining the submaximal aerobic capacity decline
Inflammation and apoptosis
It is now well known that NIDDM patients have systemic,Citation16 adipose tissue,Citation17 and muscleCitation18 inflammation. This inflammation degenerates muscle in several ways; for example by the activation of the ubiquitin–proteasome systemCitation19 and stimulation of apoptosis.Citation20
Oxidative stress
The imbalance between pro-oxidants and antioxidants in favor of the former is an inseparable partner of inflammation. It is a factor in cell destruction, including muscle, but also induces changes in deoxyribonucleic acid.Citation21 In patients with NIDDM, oxidative stress, a consequence of a state of chronic hyperglycemia,Citation16 causes both a reduction in insulin secretion and decreases its action, adding to the state of insulin resistance. We believe that as in patients with chronic respiratory disease,Citation22 this oxidative stress increased significantly with overall exercise, resulting in muscle dysfunction.Citation22
Abnormalities of glucose and lipid metabolism
NIDDM results in morphological and functional abnormalities, including alterations in the hormonal system, enzymes, transport systems, use of energy substrates, and modulation of blood flow.Citation23 Indeed, it has been shown that the alteration in blood flow causes a reduction in the supply of glucose, which contributes to the decrease in total glucose uptake.Citation24 Abnormalities of glucose metabolism may also reflect alterations in the insulin receptor, such as a decrease in number or capacity for phosphorylationCitation25 and decreased translocation of glucose transporter insulin.Citation26 Phosphorylation of glucose-stimulated insulin is decreased as well as glycogen synthesis due to a defect in glucose uptake and reduced glycogen synthase activity.Citation27 Thus, muscle insulin–resistant patients are characterized by a decrease in oxidative enzyme activity, whereas the ability of anaerobic resynthesis of adenosine triphosphate is increased.Citation28 Similarly, there is a decrease in oxidative enzyme activity in the profits of glycolytic enzymes.Citation28 Thus, disturbances of carbohydrate metabolism can be summarized in a decrease in total glucose uptake, storage, and oxidation, and alterations in the insulin receptor.Citation29 NIDDM patients also have an alteration of lipid oxidation.Citation28 The rate of free fatty acids is increased in diabetics, but their availability and use by the muscle depends on capillarization and transport within the muscle cell, both of which are altered.Citation23,Citation29 For example, the activity of carnitine palmitoyl transferase is decreased in metabolic diseases and is negatively correlated with visceral adiposity.Citation23 Several other enzymatic mechanisms that allow the use of free fatty acids are also deficient as malate dehydrogenase and citrate synthase.Citation30
Abnormalities of the microcirculation
Abnormalities of the microcirculation are represented by the decrease in local blood flow, the ability to recruit, and capillary density.Citation23 So there is less availability of energy substances.Citation23
Abnormalities of muscle-fiber type
Changes in muscle-fiber types are characterized by a decrease in oxidative type I fibers and increased type II fibers, less insulin sensitivity, and low endurance.Citation31 This results in a “deconditioning” of the peripheral muscles.
Figure A1 The measured 6-minute walk distance (6MWD) of subgroups of non-insulin-dependent-diabetes mellitus males and females, according to age-group.
Abbreviation: NS, not significant.
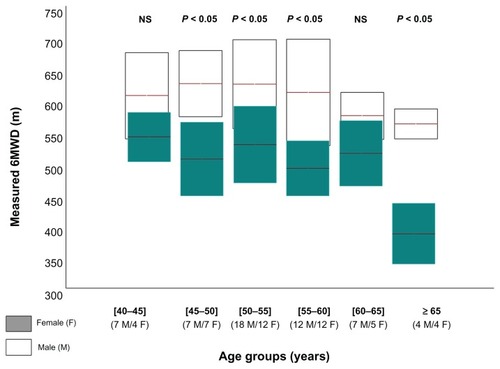
Table A1 Calculation of absolute cardiovascular disease riskCitation32
Table A2 Univariate analysis between 6-minute walk distance and the non-insulin-dependent diabetes mellitus patients’ group data
Table A3 Frequency in the present study and in the literature of risk factors and certain comorbidities in non-insulin-dependent diabetes mellitusCitation33–Citation36
References
-
Berry G
Longitudinal observations, their usefulness and limitations with special reference to the forced expiratory volume Bull Physiopathol Respir (Nancy) 1974 10 643 656 4441757
<!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}-->PubMed<!--${googleScholarLinkReplacer: %00empty%00 journal Longitudinal+observations%2C+their+usefulness+and+limitations+with+special+reference+to+the+forced+expiratory+volume author%3DG+Berry 1974 %0A%0A%0ABerry+G%0A%0A+Longitudinal+observations%2C+their+usefulness+and+limitations+with+special+reference+to+the+forced+expiratory+volume+Bull+Physiopathol+Respir+%28Nancy%29+1974+10+643+656+4441757%0A 643-656 Bull+Physiopathol+Respir+%28Nancy%29 10 %00null%00 %00empty%00 4441757 %00null%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_2_1_8_2_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Darticle%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DBerry%26rft.aufirst%3DG%26rft.atitle%3DLongitudinal%2520observations%252C%2520their%2520usefulness%2520and%2520limitations%2520with%2520special%2520reference%2520to%2520the%2520forced%2520expiratory%2520volume%26rft.jtitle%3DBull%2520Physiopathol%2520Respir%2520%2528Nancy%2529%26rft.date%3D1974%26rft.volume%3D10%26rft.spage%3D643%26rft.epage%3D656%26rft_id%3Dinfo%3Apmid%2F4441757 %00empty%00}-->
-
Ben Saad H
Prefaut C
Tabka Z
6-minute walk distance in healthy North Africans older than 40 years: influence of parity Resp Med 2009 103 74 84
<!--${if: isGetFTREnabled}-->
-
Ganguli M
Lytle ME
Reynolds MD
Dodge HH
Random versus volunteer selection for community-based study J Gerontol A Biol Sci Med Sci 1998 53 39 46
<!--${if: isGetFTREnabled}-->
-
Ferris BG
Epidemiology standardization project II: recommended respiratory disease questionnaires for use with adults and children in epidemiological research Am Rev Respir Dis 1978 118 7 52 354446
<!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}-->PubMed Web of Science ®<!--${googleScholarLinkReplacer: %00empty%00 journal Epidemiology+standardization+project+II%3A+recommended+respiratory+disease+questionnaires+for+use+with+adults+and+children+in+epidemiological+research author%3DBG+Ferris 1978 %0A%0A%0AFerris+BG%0A%0A+Epidemiology+standardization+project+II%3A+recommended+respiratory+disease+questionnaires+for+use+with+adults+and+children+in+epidemiological+research+Am+Rev+Respir+Dis+1978+118+7+52+354446%0A 7-52 Am+Rev+Respir+Dis 118 %00null%00 %00empty%00 354446 %00null%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_2_1_8_5_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Darticle%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DFerris%26rft.aufirst%3DBG%26rft.atitle%3DEpidemiology%2520standardization%2520project%2520II%253A%2520recommended%2520respiratory%2520disease%2520questionnaires%2520for%2520use%2520with%2520adults%2520and%2520children%2520in%2520epidemiological%2520research%26rft.jtitle%3DAm%2520Rev%2520Respir%2520Dis%26rft.date%3D1978%26rft.volume%3D118%26rft.spage%3D7%26rft.epage%3D52%26rft_id%3Dinfo%3Apmid%2F354446 %00empty%00}-->
-
Barrett-Connor E
Frette C
NIDDM, impaired glucose tolerance, and pulmonary function in older adults. The Rancho Bernardo Study Diabetes Care 1996 19 1441 1444 8941481
<!--${if: isGetFTREnabled}-->
-
Bouguerra R
The global diabetes pandemic: the Tunisian experience Eur J Clin Nutr 2007 61 160 165 16900086
<!--${if: isGetFTREnabled}-->
-
American Thoracic Society ATS statement: guidelines for the six-minute walk test Am J Respir Crit Care Med 2002 166 111 117 12091180
<!--${if: isGetFTREnabled}-->
-
Enright PL
McBurnie MA
Bittner V
The six-minute walk test: a quick measure of functional status in elderly adults Chest 2003 123 387 398 12576356
<!--${if: isGetFTREnabled}-->
-
Ingle L
Reddy P
Clark AL
Cleland JF
Diabetes lowers six-minute walk test performance in heart failure J Am Coll Cardiol 2006 47 1909 1910 16682322
<!--${if: isGetFTREnabled}-->
-
Jenicek M
Cleroux R
Clinical epidemiology: its evolution and role in clinical practice and research Union Med Can 1985 114 625 632 4060341
<!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}-->PubMed<!--${googleScholarLinkReplacer: %00empty%00 journal Clinical+epidemiology%3A+its+evolution+and+role+in+clinical+practice+and+research author%3DM+Jenicek%26author%3DR+Cleroux 1985 %0A%0A%0AJenicek+M%0A+%0ACleroux+R%0A%0A+Clinical+epidemiology%3A+its+evolution+and+role+in+clinical+practice+and+research+Union+Med+Can+1985+114+625+632+4060341%0A 625-632 Union+Med+Can 114 %00null%00 %00empty%00 4060341 %00null%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_2_1_8_11_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Darticle%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DJenicek%26rft.aufirst%3DM%26rft.atitle%3DClinical%2520epidemiology%253A%2520its%2520evolution%2520and%2520role%2520in%2520clinical%2520practice%2520and%2520research%26rft.jtitle%3DUnion%2520Med%2520Can%26rft.date%3D1985%26rft.volume%3D114%26rft.spage%3D625%26rft.epage%3D632%26rft_id%3Dinfo%3Apmid%2F4060341 %00empty%00}-->
-
Voorrips LE
Ravelli AC
Dongelmans PC
Deurenberg P
Van Staveren WA
A physical activity questionnaire for the elderly Med Sci Sports Exerc 1991 23 974 979 1956274
<!--${if: isGetFTREnabled}-->
-
Fang ZY
Sharman J
Prins JB
Marwick TH
Determinants of exercise capacity in patients with type 2 diabetes Diabetes Care 2005 28 1643 1648 15983314
<!--${if: isGetFTREnabled}-->
-
Bessinger RC
McMurray RG
Hackney AC
Substrate utilization and hormonal responses to moderate intensity exercise during pregnancy and after delivery Am J Obstet Gynecol 2002 186 757 764 11967503
<!--${if: isGetFTREnabled}-->
-
Jauniaux E
Poston L
Burton GJ
Placental-related diseases of pregnancy: involvement of oxidative stress and implications in human evolution Hum Reprod Update 2006 12 747 755 16682385
<!--${if: isGetFTREnabled}-->
-
Ben Saad H
Tfifha M
Harabi I
Factors influencing ventilatory variables of Tunisian women aged 45 years and more Rev Mal Respir 2006 23 324 238 17127908
<!--${if: isGetFTREnabled}-->
-
Qi L
Rifai N
Hu FB
Interleukin-6 receptor gene, plasma C-reactive protein, and diabetes risk in women Diabetes 2009 58 275 278 18852330
<!--${if: isGetFTREnabled}-->
-
Bastard JP
Maachi M
Lagathu C
Recent advances in the relationship between obesity, inflammation and insulin resistance Eur Cytokine Netw 2006 17 4 12 16613757
<!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}-->PubMed Web of Science ®<!--${googleScholarLinkReplacer: %00empty%00 journal Recent+advances+in+the+relationship+between+obesity%2C+inflammation+and+insulin+resistance author%3DJP+Bastard%26author%3DM+Maachi%26author%3DC+Lagathu 2006 %0A%0A%0ABastard+JP%0A+%0AMaachi+M%0A+%0ALagathu+C%0A%0A+Recent+advances+in+the+relationship+between+obesity%2C+inflammation+and+insulin+resistance+Eur+Cytokine+Netw+2006+17+4+12+16613757%0A 4-12 Eur+Cytokine+Netw 17 %00null%00 %00empty%00 16613757 %00null%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_2_1_8_18_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Darticle%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DBastard%26rft.aufirst%3DJP%26rft.atitle%3DRecent%2520advances%2520in%2520the%2520relationship%2520between%2520obesity%252C%2520inflammation%2520and%2520insulin%2520resistance%26rft.jtitle%3DEur%2520Cytokine%2520Netw%26rft.date%3D2006%26rft.volume%3D17%26rft.spage%3D4%26rft.epage%3D12%26rft_id%3Dinfo%3Apmid%2F16613757 %00empty%00}-->
-
Remels AH
Langen R
Gosker HR
PPARgamma inhibits NF-kappaB-dependent transcriptional activation in skeletal muscle Am J Physiol Endocrinol Metab 2009 297 174 183
<!--${if: isGetFTREnabled}-->
-
Llovera M
García-Martínez C
Agell N
López-Soriano FJ
Argilés JM
TNF can directly induce the expression of ubiquitin-dependent proteolytic system in rat soleus muscles Biochem Biophys Res Commun 1997 13 238 241 9016756
<!--${if: isGetFTREnabled}-->
-
Kusminski CM
Shetty S
Orci L
Unger RH
Scherer PE
Diabetes and apoptosis: lipotoxicity Apoptosis 2009 14 1484 1495 19421860
<!--${if: isGetFTREnabled}-->
-
Dröge W
Free radicals in the physiological control of cell function Physiol Rev 2002 82 47 95 11773609
<!--${if: isGetFTREnabled}-->
-
Barreiro E
Gea J
Corominas JM
Hussain SN
Nitric oxide synthases and protein oxidation in the quadriceps femoris of patients with chronic obstructive pulmonary disease Am J Respir Cell Mol Biol 2003 29 771 778 12816735
<!--${if: isGetFTREnabled}-->
-
Mercier J
Peripheral muscles and metabolic diseases Rev Mal Respir 2001 18 Suppl 2 22 24
<!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}-->Web of Science ®<!--${googleScholarLinkReplacer: %00empty%00 journal Peripheral+muscles+and+metabolic+diseases author%3DJ+Mercier 2001 %0A%0A%0AMercier+J%0A%0A+Peripheral+muscles+and+metabolic+diseases+Rev+Mal+Respir+2001+18+Suppl+2+22+24%0A 22-24 Rev+Mal+Respir 18 Suppl+2 %00empty%00 %00empty%00 %00null%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_2_1_8_24_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Darticle%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DMercier%26rft.aufirst%3DJ%26rft.atitle%3DPeripheral%2520muscles%2520and%2520metabolic%2520diseases%26rft.jtitle%3DRev%2520Mal%2520Respir%26rft.date%3D2001%26rft.volume%3D18%26rft.issue%3DSuppl%25202%26rft.spage%3D22%26rft.epage%3D24 %00empty%00}-->
-
Zierath JR
Handberg A
Tally M
Wallberg-Henriksson H
C-peptide stimulates glucose transport in isolated human skeletal muscle independent of insulin receptor and tyrosine kinase activation Diabetologia 1996 39 306 313 8721776
<!--${if: isGetFTREnabled}-->
-
Goodyear LJ
Giorgino F
Sherman LA
Carey RJ
Smith RJ
Dohm GL
Insulin receptor phosphorylation, insulin substrate 1 phosphorylation and phosphatidylinositol 3-kinase are decreased in intact skeletal muscle strips from obese subjects J Clin Invest 1995 95 2195 2204 7537758
<!--${if: isGetFTREnabled}-->
-
Perez MA
Raynaud E
Mercier J
Insulin resistance and associated metabolic abnormalities in muscle: effects of exercise Obesity 2001 2 47 59
<!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}--><!--${googleScholarLinkReplacer: %00empty%00 journal Insulin+resistance+and+associated+metabolic+abnormalities+in+muscle%3A+effects+of+exercise author%3DMA+Perez%26author%3DE+Raynaud%26author%3DJ+Mercier 2001 %0A%0A%0APerez+MA%0A+%0ARaynaud+E%0A+%0AMercier+J%0A%0A+Insulin+resistance+and+associated+metabolic+abnormalities+in+muscle%3A+effects+of+exercise+Obesity+2001+2+47+59%0A 47-59 Obesity 2 %00null%00 %00empty%00 %00empty%00 %00null%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_2_1_8_27_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Darticle%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DPerez%26rft.aufirst%3DMA%26rft.atitle%3DInsulin%2520resistance%2520and%2520associated%2520metabolic%2520abnormalities%2520in%2520muscle%253A%2520effects%2520of%2520exercise%26rft.jtitle%3DObesity%26rft.date%3D2001%26rft.volume%3D2%26rft.spage%3D47%26rft.epage%3D59 %00empty%00}-->
-
Felberg JP
Haesler E
Jéquier E
Metabolic origin of insulin resistance in obesity with and without type 2 (non-insulin-dependent) diabetes mellitus Diabetologia 1993 36 1221 1229 8307248
<!--${if: isGetFTREnabled}-->
-
Simoneau J
Kelley D
Altered glycolytic and oxidative capacities of skeletal muscle contribute to insulin resistance in NIDDM J Appl Physiol 1997 83 166 171 9216960
<!--${if: isGetFTREnabled}-->
-
Moulias S
Myopathies of the elderly Rev Rhum 2004 71 510 514
<!--${if: isGetFTREnabled}-->
-
Bouchard C
Tremblay A
Després JP
The response to long-term overfeeding in identical twins N Engl J Med 1990 322 1477 1482 2336074
<!--${if: isGetFTREnabled}-->
-
Marin P
Anderson B
Krotkiewski M
Björntorp P
Muscle fiber composition and capillary density in women and men with NIDDM Diabetes Care 1994 17 382 386 8062604
<!--${if: isGetFTREnabled}-->
-
Assmann G
Cullen P
Schulte H
Simple scoring scheme for calculating the risk of acute coronary events based on the 10-year follow-up of the prospective cardiovascular Münster (PROCAM) study Circulation 2002 105 310 315 11804985
<!--${if: isGetFTREnabled}-->
-
Gharbi M
Belhani A
Ben Aleya A
Epidemiology of diabetes in Tunisia Tunis Med 1995 73 235 239 9506171
<!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}-->PubMed<!--${googleScholarLinkReplacer: %00empty%00 journal Epidemiology+of+diabetes+in+Tunisia author%3DM+Gharbi%26author%3DA+Belhani%26author%3DA+Ben+Aleya 1995 %0A%0A%0AGharbi+M%0A+%0ABelhani+A%0A+%0ABen+Aleya+A%0A%0A+Epidemiology+of+diabetes+in+Tunisia+Tunis+Med+1995+73+235+239+9506171%0A 235-239 Tunis+Med 73 %00null%00 %00empty%00 9506171 %00null%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_2_1_8_34_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Darticle%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DGharbi%26rft.aufirst%3DM%26rft.atitle%3DEpidemiology%2520of%2520diabetes%2520in%2520Tunisia%26rft.jtitle%3DTunis%2520Med%26rft.date%3D1995%26rft.volume%3D73%26rft.spage%3D235%26rft.epage%3D239%26rft_id%3Dinfo%3Apmid%2F9506171 %00empty%00}-->
-
López Suárez A
Elvira González J
Beltrán Robles M
Prevalence of obesity, diabetes, hypertension, hypercholesterolemia and metabolic syndrome in over 50-year-olds in Sanlúcar de Barrameda, Spain Rev Esp Cardiol 2008 61 1150 1158 19000490
<!--${if: isGetFTREnabled}-->
-
Touré NO
Dia Kane Y
Diatta A
Tuberculosis and diabetes Rev Mal Respir 2007 24 869 875 17925669
<!--${if: isGetFTREnabled}-->
-
Ghannem H
Hadj Fredj A
Eating habits and cardiovascular risk factors. Epidemiologic study of the Tunisian Sahel [French] Presse Med 1999 28 1005 1008 10379346
<!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}-->PubMed Web of Science ®<!--${googleScholarLinkReplacer: %00empty%00 journal Eating+habits+and+cardiovascular+risk+factors.+Epidemiologic+study+of+the+Tunisian+Sahel+%5BFrench%5D author%3DH+Ghannem%26author%3DA+Hadj+Fredj 1999 %0A%0A%0AGhannem+H%0A+%0AHadj+Fredj+A%0A%0A+Eating+habits+and+cardiovascular+risk+factors.+Epidemiologic+study+of+the+Tunisian+Sahel+%5BFrench%5D+Presse+Med+1999+28+1005+1008+10379346%0A 1005-1008 Presse+Med 28 %00null%00 %00empty%00 10379346 %00null%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_2_1_8_37_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Darticle%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DGhannem%26rft.aufirst%3DH%26rft.atitle%3DEating%2520habits%2520and%2520cardiovascular%2520risk%2520factors.%2520Epidemiologic%2520study%2520of%2520the%2520Tunisian%2520Sahel%2520%255BFrench%255D%26rft.jtitle%3DPresse%2520Med%26rft.date%3D1999%26rft.volume%3D28%26rft.spage%3D1005%26rft.epage%3D1008%26rft_id%3Dinfo%3Apmid%2F10379346 %00empty%00}-->