
Abstract
Purpose
We aimed to analyze the relationship between handgrip strength/relative handgrip strength among older Han adults with type 2 diabetes mellitus (T2DM) by gender to determine the optimal cut-off value of grip strength for older adults.
Methods
A multi-stage sampling method was used to conduct a questionnaire survey and physical examination of 6128 older adults in Anhui Province. Chi-squares tests, t-tests, analysis of variance, and logistic regression analysis were used to analyze the association between handgrip strength/relative handgrip strength and T2DM between the sexes. The decision tree model (CRT) was used to explore the predictive value of handgrip strength /relative handgrip strength on T2DM.
Results
There was an association between handgrip strength and T2DM (P = 0.006, OR = 0.985, 95% CI = 0.975, 0.996), which was found in females (P = 0.013, OR = 0.978, 95% CI = 0.961, 0.995) but not in males (P = 0.125, OR = 0.989, 95% CI = 0.976, 1.003). Relative handgrip strength was also correlated with T2DM (P = 0.014, OR = 0.730, 95% CI = 0.568, 0.939), which was found in females (P = 0.003, OR = 0.534, 95% CI = 0.352, 0.809) but not in males (P = 0.432, OR = 0.879, 95% CI = 0.638, 1.212). The incidence of T2DM in elderly females with hypertension who were uneducated and with a handgrip strength of <17.350 kg was 24.3% (115 cases), whereas that in elderly females with hypertension and a relative handgrip strength of <0.240 was 29.0% (127 cases).
Conclusion
According to our results, handgrip strength and relative handgrip strength were associated with T2DM. People with hypertension had a higher risk of T2DM in women with a handgrip strength of ≤ 17.350kg and a relative grip strength of ≤ 0.240. Further research is needed to validate the effectiveness of this cut-off for implementing interventions and avoiding risks.
Introduction
Diabetes mellitus (DM) is a serious chronic endocrine and metabolic disease that is caused by insufficient insulin secretion and defective insulin action because of multiple pathogenic factors.Citation1 The prevalence of DM is as high as 11.2% in China, of which 90% are of type 2 diabetes mellitus (T2DM).Citation2 The prevalence of T2DM in Chinese adults 60 years and older is close to 20%, placing a heavy burden on individuals, families, and society.2
T2DM is most common in older adults (ie, aged 60 years or older),Citation3 resulting in complications such as kidney failure, amputation, vision loss, and nerve damage that directly affect quality of life.Citation4,Citation5 The problem of global aging has become increasingly prominent. The 2021 China Census reported 264 million people over the age of 60. According to the World Health Organization, the global aging population (ie, aged 60 years and older) will increase to 1.4 billion by 2030 and 2.1 billion by 2050.Citation6 Thus, T2DM has become a serious public health problem, and it is important to adopt scientific methods to evaluate and prevent diabetes.
Previous studies have shown lower muscle strength is one of the risk factors for T2DM,Citation7 as it can lead to a reduction in surface area for glucose delivery, which increases insulin resistance (ie, the inability of insulin to stimulate glucose disposal) and triggers T2DM.Citation8,Citation9 As an indicator of muscle strength, handgrip strength has been proposed and used to screen T2DM,Citation10 with decreased handgrip strength being associated with an increased prevalence of T2DM.Citation11 Meanwhile, studies have found that muscle strength is higher among males than among females at any age.Citation12 Furthermore, abdominal fat can lead to a greater loss of muscle strength through neuroendocrine dysregulation and may result in different rates of muscle strength decline in older adults of different genders.Citation13 Another major cause of T2DM is obesity, as obese populations demonstrate a higher risk of T2DM,Citation13,Citation14 with body mass index (BMI) being the most commonly used indicator of obesity.Citation15
In summary, the relationship between obesity, muscle strength, and T2DM is complex. At present, some scholars have explored the relationship between grip strength or relative grip strength normalized according to BMI and hypertension.Citation16 However, we have not found a study that explores the relationship between BMI-standardized handgrip strength and T2DM. Hence, this study proposed that the effect of handgrip strength on T2DM may be influenced by BMI and gender. We explored the relationship between grip strength or relative grip strength and T2DM in terms of gender to determine the optimal cut-off value of grip strength or relative grip strength for older adults.
Materials and Methods
Study Population
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Anhui Medical University. The data came from the Anhui Healthy Longevity Survey (AHLS), the details of which have been reported elsewhere.Citation17 The multi-stage sampling method and the principle of randomization were used in this survey. In the first stage, according to geographical location, cities were selected from the east, west, south, and north of Anhui Province. In the second stage, three to five urban communities were randomly selected among all others in each sample city, and three to five rural communities were selected in each sample city following the same principle. In the third stage, within the selected communities, a face-to-face questionnaire survey with 750 samples each in urban and rural areas was completed following the principle of random and voluntary participation. The study population was adults aged 60 or over, living in Anhui Province for at least half a year, with good cognitive ability to cooperate with the investigation. A questionnaire was conducted among 6128 older adults of the Chinese Han population, and the investigators were recruited from teachers and students at Anhui Medical University. After excluding individuals with missing demographic characteristics or handgrip strength values, the final sample size was 5864 (95.7%).
Questionnaire Survey
A face-to-face questionnaire survey was conducted by investigators who had been uniformly trained and passed an assessment. The inspector checked each questionnaire on the same day it was taken to ensure its quality. The questionnaire included questions about age, gender (male or female), education level (uneducated, primary school, junior school, high school, and above), income (<6500, 6500–15,000, 15,000–24,000, >24,000 RMB),Citation18 smoking history (yes or no), alcohol history (yes or no), hypertension (yes or no), and T2DM (yes or no) (diagnosis by medical institutions at or above the county level).
Physical Measurements
Handgrip strength was measured using an electronic dynamometer, whose usage was demonstrated to the participants by the investigator before the measurement. All participants were asked to stand upright with their feet apart, their elbows bent at right angles, and their wrists in a neutral position. The participants were asked to squeeze the dynamometer handle with a maximum force for 2–3 seconds, with three measurements each for the left and right hands in turn. The study used the maximum handgrip strength value of the dominant hand for statistical analysis. The dynamometer was calibrated prior to measurement to ensure that the error was within 0.1 kg.Citation19 The investigators gave verbal encouragement during the measurements to elicit the maximum performance of the participants. Relative grip strength was used for assessment, which is the patient’s grip strength divided by their BMI.
Height was measured with a steel tape measure. The participants were asked to take off their shoes and caps. During the measurement, the patient’s torso was naturally straight, the head was straight, and both eyes were looking straight ahead. The heel, sacrum, and shoulder blades were in contact with an upright post, and the patient assumed a “three-point, one-line” standing posture. The investigator’s eyes were at the same height as the horizontal pressure plate when taking the height measurement.
Body weight was measured using an electronic weight meter. The weight meter was corrected before measurement to ensure that the error was not greater than 0.1 kg. During the measurement, the weight meter was placed on level ground, and the participant was asked to stand barefoot in its center. The participants were then grouped into the following BMI categories: thin (BMI < 18.5 kg/m2), normal (18.5 ≤ BMI ≤ 24.9 kg/m2), overweight (25.0 ≤ BMI ≤ 29.9 kg/m2), and obese (BMI ≥ 30.0 kg/m2).
Statistical Analysis
Epi Data software (version 3.1) was used for data entry and double check. Statistical analyses were performed using SPSS software (version 25.0). Continuous variables were presented as means ± standard deviations, and categorical variables were expressed as proportions. The distribution differences of gender, age, education level, smoking history, drinking history, hypertension history, BMI, handgrip strength, and relative handgrip strength between the diabetic group and the non-diabetic group were analyzed by chi-squared tests or t-tests. The distribution differences of gender, age, education level, smoking history, drinking history, hypertension history, and BMI in handgrip strength or relative handgrip strength were analyzed by variance analyses (ANOVA) and t-tests. The relationship between T2DM and handgrip strength or relative handgrip strength was analyzed using binary logistic regression. The dependent variable was T2DM, and the covariates were age, gender, education level, annual average personal income, smoking history, drinking history, and hypertension. Handgrip strength and age were continuous variable data, and the other variables were categorical variable data. Based on single-factor and multi-factor studies, the decision tree model (CRT) was further used to explore the influence of different factors and the prediction of T2DM. The significant level was set at 0.05 (α = 0.05).
Results
General Characteristics of the Study Population
A total of 5864 individuals were included in this study. Of these, 45.5% (2666) were male (mean age: 70.96±6.99 years, mean BMI: 23.87±3.45 kg/m2) and 54.5% (3198) were female (mean age: 70.97±7.15 years, mean BMI: 24.47±3.81 kg/m2). The prevalence of T2DM was 15.59%. There were statistical differences in education level, income, smoking, hypertension, and BMI (P<0.05), whereas there were no statistical differences in gender, age, and alcohol use (P>0.05) ().
Table 1 General Characteristics of Participants [n (%)]
Handgrip Strength with Different Demographic Characteristics
There were statistical differences in handgrip strength and relative handgrip strength between different genders (all P < 0.001). Similarly, handgrip strength and relative handgrip strength showed statistical differences among different education level, income, alcohol use, smoking, hypertension, and BMI groups (all P < 0.001) ().
Table 2 Handgrip Strength with Different Demographic Characteristics
Association Between Handgrip Strength/Relative Handgrip Strength and T2DM
The data showed an association between handgrip strength/relative handgrip strength and T2DM (OR=0.985, 95% CI=0.975, 0.996; OR=0.730, 95% CI=0.568, 0.939). The results showed that in the older adult population, highly educated, high-income, and hypertensive patients were at higher risk of T2DM. Sex-stratified analyses showed that the association between handgrip strength and T2DM had statistical differences in women (OR=0.978, 95% CI=0.961, 0.995; OR=0.534, 95% CI=0.352, 0.809) but not in men (OR=0.989, 95% CI=0.976, 1.003/ OR=0.879, 95% CI=0.638, 1.212) ( and ).
Table 3 Binary Logistic Regression Analysis of Handgrip Strength and T2DM
Table 4 Binary Logistic Regression Analysis of Relative Handgrip Strength and T2DM
Prediction of Handgrip Strength/Relative Handgrip Strength on T2DM
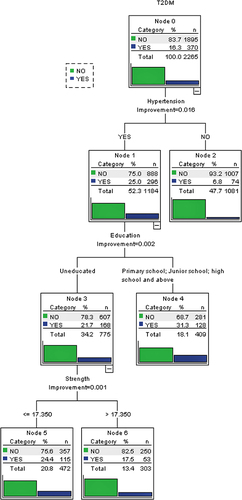
A predictive decision tree model of handgrip strength toward T2DM in females is shown in , which showed an average accuracy of 84.0%. The proportion of T2DM in those with hypertension was 25.0% (296 cases). Among those with hypertension, 21.7% (168 cases) were uneducated, and 24.3% (115 cases) were uneducated and with a handgrip strength of ≤ 17.350 kg.
Figure 1 The predictive decision tree model of handgrip strength to T2DM in females.
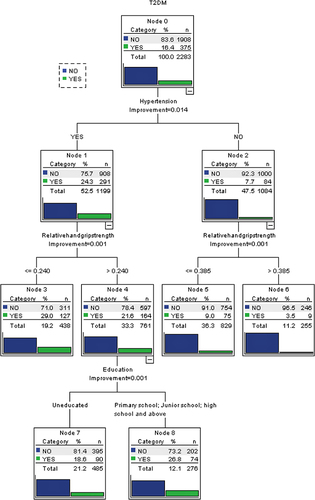
A predictive decision tree model of relative handgrip strength toward T2DM in females is shown in , which showed an average accuracy of 84.3%. Among those with hypertension, 24.3% (291 cases) had T2DM, and 29.0% (127 cases) had a relative handgrip strength of ≤ 0.240 kg. Handgrip strength/relative grip strength had no significant predictive value in the male decision tree model. Thus, hypertension, education level, income, and grip strength/relative grip strength were important influencing factors. We can also conclude from the results that high-income people are at greater risk of T2DM than low-income people, and hypertensive patients are at greater risk than non-hypertensive patients. Among the female patients with hypertension, those with a grip strength of ≤ 17.250 kg and a relative grip strength of < 0.296 kg are at greater risk of T2DM.
Figure 2 The predictive decision tree model of relative handgrip strength to T2DM in females.
Discussion
According to previous research, obesity affects muscle strength, which is an important risk factor for T2DM.Citation20–23 More importantly, BMI is related to handgrip strength and T2DM.Citation24,Citation25 Therefore, we considered that BMI may be a confounding factor in the relationship between handgrip strength and T2DM and used BMI to standardize handgrip strength to explore this effect. The results of the study showed the following: first, the grip strength of the Han elderly was related to T2DM, similar to the results of previous studies of other races. Second, there was also a correlation between relative grip strength and T2DM. Third, there were obvious gender differences in the above correlation.
The results showed that the risk of T2DM was negatively correlated with handgrip strength or relative handgrip strength, consistent with Merchant RA’s research results.Citation20 In our study, the risk of T2DM decreased by 1.5% for each unit increase in handgrip strength, and by 27.0% with each unit increase in relative handgrip strength. Possible causes for this relationship are decreased muscle strength, which may lead to impaired glucose tolerance and inflammation, affecting glucose metabolism and insulin resistance.Citation26,Citation27 Furthermore, reduced insulin signaling could lead to decreased protein synthesis and increased activation of protein degradation pathways, leading to muscle strength loss.Citation28 Therefore, the increased risk of T2DM was not only the outcome of muscle strength loss but also its cause.Citation29
Interestingly, being overweight and obese are not only risk factors for T2DM but also consequences of T2DM. First, being overweight and obese will cause a low-grade chronic inflammatory state and mitochondrial dysfunction in the human body in response to overnutrition, which produces insulin resistance and promotes the development of T2DM.Citation22 Second, weight gain may result if T2DM patients are treated with insulin therapy, which may be the result of insulin inhibiting protein metabolism and stimulating lipid production to increase fat accumulation.Citation30 Third, overweight and obese older adult diabetes patients often lack daily activity, which can lead to a reduction in muscle strength, deterioration in glycemic control, and may further exacerbate physical inactivity.Citation28 Meanwhile, the logistics results of this study show that highly educated, high-income, and hypertensive patients were at higher risk of diabetes. It may be that people with high levels of education and income have better medical treatment levels, stronger health awareness, and higher treatment rates for chronic diseases than others.Citation2 Moreover, patients with hypertension often exhibit insulin resistance, so they are at greater risk of developing diabetes than normotensive individuals.Citation31
As there was an association between gender and handgrip strength, a categorical analysis of gender in older adults was performed.Citation32 It was found that the association between handgrip strength or relative handgrip strength and T2DM in women was not found in men. In women, the risk of T2DM decreased by 2.2% for every unit increase in handgrip strength, and 46.6% for every unit increase in relative handgrip strength. This gender difference may be related to factors such as sex hormones, glucose balance, and body composition.Citation33,Citation34 First, in older adults, Fetuin-A (a protein primarily secreted by the liver that regulates insulin signaling) levels are higher in women than in men, increasing the former’s risk of T2DM.Citation35 Second, a decline in sex hormone levels can aggravate the impaired glucose metabolism of women as they age.Citation33 Third, higher androgen activity may be present after menopause in women, resulting in impaired glucose tolerance and the promotion of insulin resistance.Citation36 Finally, older men have high concentrations of anabolic hormones, which stimulate muscle protein synthesis by increasing lean muscle mass, leading to greater strength than in women.Citation37 Other studies have found that increasing muscle strength to reduce the risk of death from various causes seems to be more important for older women than for men.Citation37 Therefore, it is necessary to consider the effect of gender when analyzing the association between handgrip strength and T2DM.
T2DM has become a serious threat with increasingly aging populations. Therefore, taking appropriate measures to prevent, screen, and control the occurrence and development of diabetes can promote healthy aging. At the same time, it is also conducive to promote the combination of health management and medical services for old adults, establish a medical and health service system, promote the prevention and treatment of chronic diseases, and improve the health level of older adults. From the results of this study, we recommend that elderly women with hypertension, especially uneducated women, should pay attention to control blood glucose when their grip strength is less than 17.350 kg or their relative grip strength is less than 0.296.
Our study has several strengths, such as a large sample size obtained by multi-stage stratified sampling. Second, income in our study differs from classifications in general research. Instead, it was classified according to the average income and expenditure in the Survey Report on the Living Conditions of China’s Urban and Rural Older Persons (2018), which can better meet the particularity of the research object for the old adults. However, there were still some limitations that should be considered. This study was cross-sectional and could not explore the causal association between handgrip strength and T2DM. Meanwhile, a history of hypertension may affect an individual’s metabolic levels, which can affect the results. However, combined with the results of previous studies, we can conclude that handgrip strength is related to the prevention and control of T2DM. Gender factors should be considered when using handgrip strength to screen for T2DM. Future studies could adopt a prospective cohort study to explore the causal relationship between handgrip strength and T2DM.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Statement
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Anhui Medical University, Hefei, China (no. 2020H011).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
Acknowledgments
Thanks to all participants who voluntarily participated in the study. We would like to thank the editors of this manuscript and Charlesworth for English language editing. Qian Huang and Xing Chen are co-first authors for this study. Dong Mei Zhang and Gui Mei Chen are co-correspondence authors for this study.
Additional information
Funding
References
- Alberti KG, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med. 1998;15(7):539–553. doi:10.1002/(SICI)1096-9136(199807)15:7<539::AID-DIA668>3.0.CO;2-S
- Chinese Diabetes Society. Guideline for the prevention and treatment of type 2 diabetes mellitus in China (2020 edition). Chin J Pract Intern Med. 2021;41(8):668–695. doi:10.19538/j.nk2021080106
- de Carvalho DHT, Scholes S, Santos JLF, de Oliveira C, Alexandre TDS. Does abdominal obesity accelerate muscle strength decline in older adults? Evidence from the English longitudinal study of ageing. J Gerontol a Biol Sci Med Sci. 2019;74(7):1105–1111. doi:10.1093/gerona/gly178
- International Diabetes Federation. Type 2 Diabetes. International Diabetes Federation; 2020.
- World Health Organization. Diabetes. World Health Organization; 2021.
- World Health Organization. Ageing. World Health Organization; 2021.
- Tarp J, Støle AP, Blond K, Grøntved A. Cardiorespiratory fitness, muscular strength and risk of type 2 diabetes: a systematic review and meta-analysis. Diabetologia. 2019;62(7):1129–1142. doi:10.1007/s00125-019-4867-4
- Ma RCW. Epidemiology of diabetes and diabetic complications in China [published correction appears in Diabetologia. 2018 Apr 18;]. Diabetologia. 2018;61(6):1249–1260. doi:10.1007/s00125-018-4557-7
- Rohm TV, Meier DT, Olefsky JM, Donath MY. Inflammation in obesity, diabetes, and related disorders. Immunity. 2022;55(1):31–55. doi:10.1016/j.immuni.2021.12.013
- Bohannon RW. Grip strength: an indispensable biomarker for older adults. Clin Interv Aging. 2019;14:1681–1691. doi:10.2147/CIA.S194543
- Tan NC, Sankari U, Ng CE, Koh YLE. Longitudinal study on the progression of muscle status among community-dwelling ambulatory older multiethnic Asians with type 2 diabetes mellitus. BMC Geriatr. 2022;22(1):446. doi:10.1186/s12877-022-03098-0
- Benfica PDA, Aguiar LT, Brito SAF, Bernardino LHN, Teixeira-Salmela LF, Faria CDCM. Reference values for muscle strength: a systematic review with a descriptive meta-analysis [published correction appears in Braz J Phys Ther. 2019 Nov - Dec; 23(6): 549]. Braz J Phys Ther. 2018;22(5):355–369. doi:10.1016/j.bjpt.2018.02.006
- Galicia-Garcia U, Benito-Vicente A, Jebari S, et al. Pathophysiology of Type 2 Diabetes Mellitus. Int J Mol Sci. 2020;21(17):6275. doi:10.3390/ijms21176275
- La Sala L, Pontiroli AE. Prevention of diabetes and cardiovascular disease in obesity. Int J Mol Sci. 2020;21(21):8178. doi:10.3390/ijms21218178
- Toplak H, Leitner DR, Harreiter J, et al. “Diabesity” – adipositas und typ-2-diabetes (update 2019) [“Diabesity”-Obesity and type 2 diabetes (update 2019)]. Wien Klin Wochenschr. 2019;131(Suppl1):71–76. doi:10.1007/s00508-018-1418-9
- Chon D, Shin J, Kim JH, Mogi M. Consideration of body mass index (BMI) in the association between hand grip strength and hypertension: Korean Longitudinal Study of Ageing (KLoSA). PLoS One. 2020;15(10):e0241360. doi:10.1371/journal.pone.0241360
- Fangfang H, Xiao H, Shuai Z, et al. Living environment, built environment and cognitive function among older Chinese adults: results from a cross-sectional study. J Prev Alzheimers Dis. 2022;9(1):126–135. doi:10.14283/jpad.2021.59
- Junwu D, Yanyan W, Nina L, editors. Blue Book of Aging: A Survey Report on the Living Conditions of China’s Urban and Rural Older Persons (2018). Beijing, China: Social Sciences Academic Press; 2018:21–96.
- Bobos P, Nazari G, Lu Z, MacDermid JC. Measurement properties of the hand grip strength assessment: a systematic review with meta-analysis. Arch Phys Med Rehabil. 2020;101(3):553–565. doi:10.1016/j.apmr.2019.10.183
- Merchant RA, Chan YH, Lim JY, Morley JE. Prevalence of metabolic syndrome and association with grip strength in older adults: findings from the HOPE study. Diabetes Metab Syndr Obes. 2020;13:2677–2686. doi:10.2147/DMSO.S260544
- Jeon YJ, Lee SK, Shin C. Normalized hand grip and back muscle strength as risk factors for incident type 2 diabetes mellitus: 16 years of follow-up in a population-based cohort study. Diabetes Metab Syndr Obes. 2021;14:741–750. doi:10.2147/DMSO.S283853
- Kuryłowicz A, Koźniewski K. Anti-inflammatory strategies targeting metaflammation in type 2 diabetes. Molecules. 2020;25(9):2224. doi:10.3390/molecules25092224
- McGrath R, Vincent BM, Al Snih S, Markides KS, Peterson MD. The association between muscle weakness and incident diabetes in older Mexican Americans. J Am Med Dir Assoc. 2017;18(5):452.e7–452.e12. doi:10.1016/j.jamda.2017.01.017
- Zhao Y, Qie R, Han M, et al. Association of BMI with cardiovascular disease incidence and mortality in patients with type 2 diabetes mellitus: a systematic review and dose-response meta-analysis of cohort studies. Nutr Metab Cardiovasc Dis. 2021;31(7):1976–1984. doi:10.1016/j.numecd.2021.03.003
- Parra-Soto S, Pell JP, Celis-Morales C, Ho FK. Absolute and relative grip strength as predictors of cancer: prospective cohort study of 445 552 participants in UK Biobank. J Cachexia Sarcopenia Muscle. 2022;13(1):325–332. doi:10.1002/jcsm.12863
- Li S, Zhang R, Pan G, Zheng L, Li C. Handgrip strength is associated with insulin resistance and glucose metabolism in adolescents: evidence from National Health and Nutrition Examination Survey 2011 to 2014. Pediatr Diabetes. 2018;19(3):375–380. doi:10.1111/pedi.12596
- Jang BN, Nari F, Kim S, Park EC, Lombardo M. Association between relative handgrip strength and prediabetes among South Korean adults. PLoS One. 2020;15(10):e0240027. doi:10.1371/journal.pone.0240027
- Nomura T, Kawae T, Kataoka H, Ikeda Y. Assessment of lower extremity muscle mass, muscle strength, and exercise therapy in elderly patients with diabetes mellitus. Environ Health Prev Med. 2018;23(1):20. doi:10.1186/s12199-018-0710-7
- Bawadi H, Alkhatib D, Abu-Hijleh H, Alalwani J, Majed L, Shi Z. Muscle strength and glycaemic control among patients with type 2 diabetes. Nutrients. 2020;12(3):771. doi:10.3390/nu12030771
- Mottalib A, Kasetty M, Mar JY, Elseaidy T, Ashrafzadeh S, Hamdy O. Weight management in patients with type 1 diabetes and obesity. Curr Diab Rep. 2017;17(10):92. doi:10.1007/s11892-017-0918-8
- Petrie JR, Guzik TJ, Touyz RM. Diabetes, hypertension, and cardiovascular disease: clinical insights and vascular mechanisms. Can J Cardiol. 2018;34(5):575–584. doi:10.1016/j.cjca.2017.12.005
- Agnew PJ, Maas F. Hand function related to age and sex. Arch Phys Med Rehabil. 1982;63(6):269–271.
- Enikuomehin A, Kolawole BA, Soyoye OD, Adebayo JO, Ikem RT. Influence of gender on the distribution of type 2 diabetic complications at the Obafemi Awolowo teaching hospital, Ile-Ife, Nigeria. Afr Health Sci. 2020;20(1):294–307. doi:10.4314/ahs.v20i1.35
- Kunutsor SK, Voutilainen A, Laukkanen JA. Handgrip strength improves prediction of type 2 diabetes: a prospective cohort study. Ann Med. 2020;52(8):471–478. doi:10.1080/07853890.2020.1815078
- Ochieng J, Nangami G, Sakwe A, et al. Impact of Fetuin-A (AHSG) on tumor progression and type 2 diabetes. Int J Mol Sci. 2018;19(8):2211. doi:10.3390/ijms19082211
- Astapova O, Minor BMN, Hammes SR. Physiological and pathological androgen actions in the ovary. Endocrinology. 2019;160(5):1166–1174. doi:10.1210/en.2019-0010
- Damayanthi HDWT, Moy FM, Abdullah KL, Dharmaratne SD. Handgrip strength and its associated factors among community-dwelling elderly in Sri Lanka: a cross-sectional study. Asian Nurs Res. 2018;12(3):231–236. doi:10.1016/j.anr.2018.08.008