
Abstract
Background
Previous studies suggested protective effects of bilirubin against cardiovascular disease, with a possible gender difference. However, the relationship between serum total bilirubin (TBIL) with diabetic macro- and microvascular complications remains unknown. We aimed to examine the association of macro- and microvascular complications with serum TBIL levels.
Methods
Serum TBIL was measured in 648 patients with T2DM. Demographic and clinical data were obtained from the inpatient medical record system. Serum TBIL was measured with an automatic biochemistry analyzer according to routine protocols. Parameters of vascular complications, including ankle-brachial index, carotid intima-media thickness, estimated glomerular filtration rate and the urinary albumin to creatinine ratio, were measured and calculated. The association between TBIL and diabetic macro- and microvascular complications was analyzed.
Results
In multivariable logistic regression, after adjustment for age, sex, body mass index and diabetic duration, higher serum TBIL levels were significantly associated with decreased odds of microalbuminuria (OR = 0.31, [95% CI] 0.16–0.61, P = 0.003) and chronic kidney disease (OR = 0.19, [95% CI] 0.09–0.41, P < 0.001). These associations were only found in male but not in female patients. However, no significant relationship was found between TBIL and peripheral arterial disease or carotid hypertrophy.
Conclusion
Our findings suggest that physiological higher TBIL level might be a protective factor for diabetic microvascular complications.
Introduction
Diabetes mellitus (DM) is one of the most prominent chronic diseases; its prevalence is increasing and estimated to be 10.2% for 2030 among adults.Citation1 Macrovascular complications (cardiovascular disease, stroke and peripheral arterial disease (PAD)) and microvascular complications (nephropathy, retinopathy and neuropathy) are the main causes of morbidity and mortality in patients with DM.Citation2 Therefore, exploring the modifiable risk factors that are related to diabetic vascular complications is of most importance. Previous basic and clinical research data indicated that increased oxidative stress and inflammation played pivotal roles in the development of diabetic vascular complications.Citation3,Citation4
Bilirubin, as the final product of heme catabolism, includes total bilirubin (TBIL), indirect bilirubin (IBIL), and direct bilirubin (DBIL).Citation5 Recent studies have shown that bilirubin might be a possible candidate biomarker for DMCitation6 and diabetic complicationsCitation7–9 due to its potent antioxidant and anti-inflammatory properties. To date, there are few studies investigating the relationship between serum TBIL and diabetic vascular complications. We found one study that reported an association between decreased TBIL and major diabetic complications among Chinese senile diabetic patients.Citation10 However, in their study, the definition of diabetic vascular complications was obtained from the medical record, resulting in inaccurate results. On the other hand, gender differences in diabetic vascular complications have been recognized.Citation11 However, research to date has not yet investigated the gender differences in the relationship between TBIL and diabetic vascular complications in Chinese people with type 2 diabetes mellitus (T2DM).
Therefore, in this paper, we aimed to examine (1) whether serum TBIL levels are associated with diabetic macrovascular (PAD and carotid hypertrophy) and microvascular complications (microalbuminuria (MAU) and chronic kidney disease (CKD)) in Chinese people with T2DM and (2) whether gender differences exist in the association.
Methods
Study Participants
Patients with T2DM, consecutively attending the inpatient department of Geriatrics at the Second Xiangya Hospital of Central South University, Changsha, China, from January 2019 to January 2022, were initially recruited. All patients had a diagnosis of T2DM based on fasting plasma glucose (FPG) ≥7.0 mmol/l and/or 2-h plasma glucose ≥11.0 mmol/l, according to the World Health Organization criteria,Citation12 or having self-reported doctor-diagnosed T2DM. Subject inclusion criteria were as follows: (1) confirmed of newly diagnosed T2DM; (2) normal liver function tests (defined as alanine aminotransferase (ALT) <120 U/L, aspartate aminotransferase (AST) <120 U/L, TBIL < 34.2 μmol/L, and DBIL < 12.0 μmol/L). Exclusion criteria were as follows: (1) under 18 years old; (2) type 1 diabetes or other special types of diabetes; (3) diabetic acute complications, biliary obstruction disease, acute inflammatory disease, or malignant tumors; (4) missing data. A final total of 648 patients were eligible and included in this study. This study was performed according to the guidelines of the Declaration of Helsinki and was approved by the Ethics Committees of the Second Xiangya Hospital of Central South University, Changsha, Hunan Province, China (ethical approval number: 2018085). Written informed consent was obtained from all participants or their family members.
Anthropometric and Biochemical Measurements
Demographic and clinical characteristics, including age, sex, diabetic duration, medical history, and history of hypertension, stroke, coronary heart disease (CHD) were collected from the inpatient medical record system of the Second Xiangya Hospital of Central South University. Body weight and body height were measured by professionals, and body mass index (BMI) was calculated. Venous blood and urine samples were obtained in the morning after a 12-hour overnight fast. Serum total cholesterol (TC), triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), FPG, TBIL, DBIL, ALT, AST, creatinine (Crea), cystatin C (CysC) and glycated hemoglobin A1c (HbA1c) were measured by an automatic biochemistry analyzer according to routine protocols in the hospital medical laboratory. The estimated glomerular filtration rate (eGFR) was calculated using the following formulas published by the Japanese Society of Nephrology, eGFR = (104 × CysC−1.019 × 0.996age (years)) - 8 (male); eGFR = (104 × CysC−1.019 × 0.996age (years) × 0.929) - 8 (female).Citation13
Assessment of Macro- or Microvascular Complications
The Omron Non-Invasive Vascular Screening Device (BP-203RPEIII) was used to measure ankle-brachial index (ABI). Carotid intima-media thickness (CMT) was determined by a Siemens Acuson S3000 US scanner (Mountain View, CA, USA). These examinations were performed by senior clinical physicians and ultrasound doctors, respectively. In the present study, macrovascular complications included PAD (ABI < 0.90 in either leg)Citation14 and carotid hypertrophy (CMT > 0.9 mm).Citation15 Urinary albumin and creatinine concentrations were measured by turbidimetric immunoassay and enzymatic assay, respectively. For microvascular complications, CKD was defined as eGFR ≤60mL/min per 1.73 m2, MAU was defined as urinary albumin to creatinine ratio (UACR) ≥30 mg/g.
Statistical Analysis
Quantitative parameters were shown as the mean ± standard deviation (SD), and qualitative parameters were expressed as number (percentage). The quantitative parameters were compared using the Student’s t-test and one-way analysis of variance, and qualitative parameters were compared by the Chi square test. The association between serum TBIL and clinical parameters was assessed by Pearson or Spearman bivariate correlation analysis; the partial correlation coefficient was used to control for the effects of age, sex, BMI and diabetic duration. The univariate and multivariable logistic regression analyses were performed to determine the association of serum TBIL and other variables with risk of diabetic macro- and microvascular complications. A two-sided P < 0.05 was considered significant. All statistical analyses were performed using SPSS, version 26.0 (SPSS Inc, Chicago, Illinois).
Results
Participant Characteristics
The characteristics of the participants are listed in . The mean age was 65.46 ± 11.19 years, and mean TBIL level was 10.11 ± 4.63 µmol/L; male/female 395/253. The mean HbA1c was 8.27 ± 1.95%. Compared with men, women were older (67.62 ± 10.17 vs 64.09 ± 11.60 years, P < 0.001), had lower BMI (23.75 ± 3.76 vs 24.71 ± 3.19 kg/m2, P < 0.001), Crea (77.24 ± 74.05 vs 102.35 ± 74.04 μmol/L, P < 0.001), TG (1.78 ± 1.10 vs 1.98 ± 1.64 mmol/L, P = 0.044) and higher HDL-C (1.15 ± 0.31 vs 1.02 ± 0.35 mmol/L, P < 0.001). In terms of vascular complications, women showed lower CMT (0.90 ± 0.20 vs 0.94 ± 0.18 mm, P = 0.033) but higher incidence of PAD (31.62% vs 21.27%, P = 0.003).
Table 1 Characteristics of Participants
Association of Serum TBIL with Anthropometric, Biochemical and Clinical Parameters
Next, we analyzed the relationship of serum TBIL with other parameters. Serum TBIL levels were positively associated liver enzymes, DBIL, TC, HDL-C, LDL-C, and eGFR, and negatively with age, diabetic duration, Crea, TG, and UACR (P < 0.001 or P < 0.05; ). With adjustment for age, sex, BMI, and diabetic duration, serum TBIL levels correlated significantly and positively with liver enzymes, DBIL and eGFR (P < 0.001 or P < 0.05; ). A negative correlation of serum TBIL with FPG, Crea, TG, and UACR was observed (P < 0.01 or P < 0.05; ).
Table 2 Correlation Between TBIL and Clinical Parameters in All Participants
Logistic Regression According to the Quartiles of TBIL
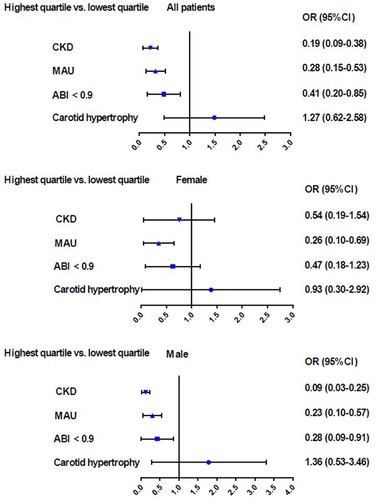
The patients were then divided into four groups (Q1, Q2, Q3, and Q4) according to the quartiles of their TBIL levels. There were significant differences among the four groups in terms of age, diabetic duration, Crea, ALT, DBIL, TG, HDL-C, CMT, eGFR, UACR, and history of stroke (P < 0.001 or P < 0.05), and no significant difference was found in the other indicators (Supplementary Table S1). As shown in and , with Q1 (first quartile) serving as the reference, TBIL levels in Q4 (fourth quartile) were associated with a decreased OR (odds ratio) for MAU (OR = 0.28, [95% CI] 0.15–0.53, P < 0.001) and CKD (OR = 0.19, [95% CI] 0.09–0.38, P < 0.001) but not for carotid hypertrophy (OR = 1.27, [95% CI] 0.62–2.58, P = 0.180) or PAD (OR = 0.41, [95% CI] 0.20–0.85, P = 0.061).
Table 3 Univariate Logistic Regression for Risk of Macro and Microvascular Complications According to the Quartiles of TBIL
Figure 1 Q4 (highest quartile) vs Q1 (first quartile) odds ratio (OR) of TBIL for macro- and microvascular complications.
In the age, sex, BMI and diabetic duration-adjusted model, the TBIL levels in Q4 were correlated with 0.31 (95% CI = 0.16–0.61, P = 0.003) odds for MAU, and 0.19 (0.09–0.41, P < 0.001) odds for CKD ( and ).
Table 4 Multivariate Logistic Regression for Risk of Macro and Microvascular Complications According to the Quartiles of TBIL
Figure 2 Q4 (highest quartile) vs Q1 (first quartile) odds ratio (OR) of TBIL for macro- and microvascular complications after adjustment for age, sex (only for overall participants), BMI and diabetic duration.
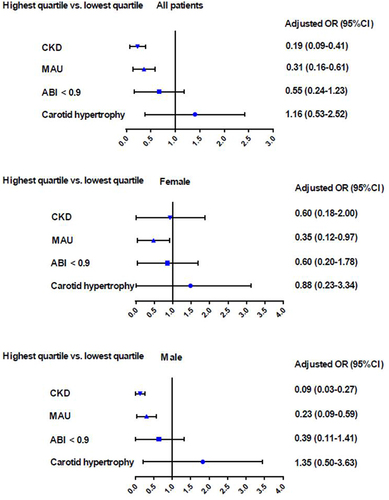
Gender-based disparities are shown in and . In the fully adjusted model, TBIL levels were significantly associated with MAU and CKD in males, with OR 0.23 and 0.09, respectively, but not in females.
Discussion
The primary finding of the present study is that a higher TBIL level was significantly associated with a lower risk of MAU and CKD in T2DM patients but not PAD or carotid hypertrophy. We further showed that the association of TBIL levels with MAU and CKD was only found in male but not in female patients. These results indicated that TBIL might be an independent protective factor against diabetic microvascular complications in male T2DM patients.
Bilirubin possessed antioxidant and anti-inflammatory activities, reported to attenuate atherosclerosis in vivo.Citation16 Atherosclerosis is the pathological basis for cardiovascular disease (CVD).Citation17 A cross-sectional study analyzed 1156 symptomatic intracranial atherosclerotic stenoses patients. The results showed that lower bilirubin levels may indicate severe intracranial atherosclerotic stenoses.Citation18 Shi et alCitation19 conducted a cross-sectional study that included 10,900 participants with hypertension. The results showed that TBIL was U-shaped associated with PAD. Zuo et alCitation20 reported a U-shaped relationship between bilirubin and CVD in the general population. However, these studies did not examine the relationship between serum TBIL levels and diabetic macro- and microvascular complications.
Macrovascular complications remain the leading cause of morbidity and mortality in individuals with T2DM. Nevertheless, we found no relationship between TBIL and PAD or carotid hypertrophy. However, those with lower TBIL levels were significantly more likely to have a history of stroke in our study. The relationship between serum TBIL levels and macrovascular complications is still controversial. A previous study among patients with hypertension showed that serum TBIL levels were negatively associated with the prevalence of PAD.Citation21 Meanwhile, a U-shaped relationship was found between TBIL and CVD in the general population.Citation20 The reasons for these contradictory results might be the different study population and health status.
Most of studies focus on the relationship between TBIL and macrovascular complications. Due to the differences in cell content between macro- and microvessels, we then explored the association between serum TBIL levels and diabetic microvascular complications. We found that serum TBIL levels were independently and negatively associated with UACR and eGFR. Additionally, multivariate logistic regression analysis indicated that TBIL may have important protective effects on MAU and CKD. Fukui et alCitation22 investigated 633 Japanese T2DM patients and reported that serum bilirubin was positively associated with eGFR and negatively associated with albuminuria. A cross-sectional study of 509 Japanese diabetic patients reported a positive association between serum bilirubin and eGFR.Citation23 Our findings were consistent with previous study, which imply an important protective effects of bilirubin on the progression of diabetic nephropathy.
Oxidative stress, inflammation and endothelial dysfunction are involved in the pathogenesis of diabetic nephropathy.Citation24,Citation25 Supplementation of antioxidants and anti-inflammatory products such as resveratrol and alpha-lipoic acid has been reported to alleviate renal injury in rats with diabetes,Citation26,Citation27 although there is limited evidence supporting their use in clinic. The mechanisms by which bilirubin functions in diabetic nephropathy remain unclear, but previous studies indicate that bilirubin could inhibit the development of diabetic nephropathy in several ways. First, Bilirubin has been shown to be a major physiologic antioxidant that can protect cells from a 10,000-fold excess of oxidants.Citation28 Fujii et alCitation29 found that bilirubin appeared to inhibit oxidative stress, thereby reducing the progression of diabetic nephropathy. Second, experimental findings have shown the anti-inflammatory properties of bilirubin.Citation30 It has been demonstrated that milder elevation of bilirubin concentrations could reduce the levels of inflammatory cytokines, such as interleukin-6 and tumor necrosis factor alpha, which might inhibit the inflammatory process of diabetic nephropathy.Citation30 Third, it was found that experimental hyperbilirubinemia may alleviate high glucose-induced endothelial dysfunction.Citation31 Serum TBIL levels can be measured easily and quickly in clinic, offering a method to identify patients at high risk of diabetic microvascular complications.
Tissue-specific effect of TBIL might partly explain why we found strong associations for microvascular and not for macrovascular complications. In addition, microvascular complications are unique to diabetic patients with long-standing hyperglycemia. Besides diabetes-induced hyperglycemia, dyslipidemia and obesity are also factors that contribute to pathogenesis of macrovascular complications.Citation32
Liu et al reported that TBIL < 16.5 µmol/L was an independent protective factor for diabetic retinopathy, when TBIL ≥ 16.5 µmol/L was positively associated with diabetic retinopathy.Citation8 Furthermore, a U-shaped association between TBIL and the prevalence of PAD was observed in Chinese patients with hypertension.Citation19 These above indicate that TBIL might exert its protective effects on diabetic microvascular complications only in the physiological range. The excessive serum TBIL levels are associated with other risk factors for developing vascular dysfunction, including increased ALT and AST levels.Citation33 According to previous and our studies, clinicians should consider whether the serum TBIL levels need to be maintained at a high level with the physiological range. More attention should be paid to the abnormal range of TBIL and the potential vascular risks.
Another important finding of this study is that there was a gender difference in the association among serum TBIL levels with diabetic microvascular complications. Previous studies have demonstrated gender differences in the association of bilirubin levels with PADCitation19 and cognition.Citation34 Such gender-differences could be attributed to sex hormones, as androgens exert detrimental effects on the cardiovascular system, whereas estrogen exhibits protective effects.Citation35 Given that the mean age of female patients in our study was beyond the average age of menopause in Chinese women,Citation36 the influence of estrogen was not so large in this study. Moreover, men may have other risk factors associated with the development of diabetic microvascular complications to women. For example, smoking is significantly hazardous for chronic kidney disease.Citation37
Limitations
Some limitations of this study need consideration. First, other diabetic macro- and microvascular complications, such as diabetic neuropathy and retinopathy and brachial-ankle pulse wave velocity, were not included in this study due to limited resources. Second, CVD risk factors known to differ by gender were not included in our study, such as socioeconomic status, dietary patterns, physical activity, and hormone levels. Besides, we did not include blood pressure in the present study, which is a risk factor for CVD. Third, our sample was hospital-based and perhaps not representative of the general population of patients with T2DM. Fourth, the sample size was relatively small in our study. Thus, further studies with a larger sample size and more indicators are warranted.
Conclusion
In conclusion, we found that serum TBIL levels were independently and negatively associated with the prevalence of MAU and CKD in male patients with T2DM. Further studies should be performed to prove the hypothesis that higher physiological TBIL levels may attenuate the development of diabetic microvascular complications.
Abbreviations
TBIL, total bilirubin; DM, diabetes mellitus; PAD, peripheral arterial disease; IBIL, indirect bilirubin; DBIL, direct bilirubin; T2DM, type 2 diabetes mellitus; MAU, microalbuminuria; CKD, chronic kidney disease; FPG, fasting plasma glucose; ALT, alanine aminotransferase; AST, aspartate aminotransferase; CHD, coronary heart disease; BMI, body mass index; TC, total cholesterol; TG, triglyceride; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; Crea, creatinine; CysC, cystatin C; HbA1c, glycated hemoglobin A1c; eGFR, estimated glomerular filtration rate; ABI, ankle-brachial index; CMT, carotid intima-media thickness; UACR, urinary albumin to creatinine ratio; SD, standard deviation; OR, odds ratio; CVD, cardiovascular disease.
Data Sharing Statement
All data are available from the corresponding author (Junkun Zhan) on reasonable request.
Disclosure
The authors declare no competing interests in this work.
Additional information
Funding
References
- Saeedi P, Petersohn I, Salpea P, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res Clin Pract. 2019;157:107843. doi:10.1016/j.diabres.2019.107843
- Arnold SV, Khunti K, Tang F, et al. Incidence rates and predictors of microvascular and macrovascular complications in patients with type 2 diabetes: results from the longitudinal global discover study. Am Heart J. 2022;243:232–239. doi:10.1016/j.ahj.2021.10.181
- Bhatti JS, Sehrawat A, Mishra J, et al. Oxidative stress in the pathophysiology of type 2 diabetes and related complications: current therapeutics strategies and future perspectives. Free Radic Biol Med. 2022;184:114–134. doi:10.1016/j.freeradbiomed.2022.03.019
- Rohm TV, Meier DT, Olefsky JM, et al. Inflammation in obesity, diabetes, and related disorders. Immunity. 2022;55(1):31–55. doi:10.1016/j.immuni.2021.12.013
- Magsi R, Shetty N, Giffen Z, et al. Serum bilirubin as a predictor of graft outcomes after renal transplant. Am J Clin Exp Urol. 2022;10(1):37–43.
- Zhong P, Sun D, Wu D, et al. Total bilirubin is negatively related to diabetes mellitus in Chinese elderly: a community study. Ann Transl Med. 2019;7(18):474. doi:10.21037/atm.2019.07.104
- Eto E, Maeda Y, Sonoda N, et al. Association of serum total bilirubin levels with progressive renal decline and end-stage kidney disease: 10-year observational cohort study in Japanese patients with diabetes. PLoS One. 2022;17(7):e0271179. doi:10.1371/journal.pone.0271179
- Liu M, Wang J, He Y. The U-shaped association between bilirubin and diabetic retinopathy risk: a five-year cohort based on 5323 male diabetic patients. J Diabetes Res. 2018;2018:4603087. doi:10.1155/2018/4603087
- Chen J, Wang J, Zhang X, et al. Inverse relationship between serum bilirubin levels and diabetic foot in chinese patients with Type 2 diabetes mellitus. Med Sci Monit. 2017;23:5916–5923. doi:10.12659/msm.907248
- Liu M, Li Y, Li J, et al. Elevated serum total bilirubin levels are negatively associated with major diabetic complications among Chinese senile diabetic patients. J Diabetes Complications. 2017;31(1):213–217. doi:10.1016/j.jdiacomp.2016.08.023
- Maric-Bilkan C. Sex differences in micro- and macro-vascular complications of diabetes mellitus. Clin Sci (Lond). 2017;131(9):833–846. doi:10.1042/CS20160998
- Alberti KG, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med. 1998;15(7):539–553. doi:10.1002/(SICI)1096-9136(199807)15:7
- The Japanese Society of Nephrology. Clinical Practice Guidebook for Diagnosis and Treatment of Chronic Kidney Disease. Jpn J Nephrol. 2012;54:1031–1189.
- Yasu T. Comprehensive cardiac rehabilitation program for peripheral arterial diseases. J Cardiol. 2022;80(4):303–305. doi:10.1016/j.jjcc.2021.11.011
- Zhao S, Yu S, Chi C, et al. Association between macro- and microvascular damage and the triglyceride glucose index in community-dwelling elderly individuals: the Northern Shanghai Study. Cardiovasc Diabetol. 2019;18(1):95. doi:10.1186/s12933-019-0898-x
- Wen G, Yao L, Hao Y, et al. Bilirubin ameliorates murine atherosclerosis through inhibiting cholesterol synthesis and reshaping the immune system. J Transl Med. 2022;20(1):1. doi:10.1186/s12967-021-03207-4
- Björkegren JLM, Lusis AJ. Atherosclerosis: recent developments. Cell. 2022;185(10):1630–1645. doi:10.1016/j.cell.2022.04.004
- Yu F, Zhang L, Liao D, et al. Serum bilirubin levels and extent of symptomatic intracranial atherosclerotic stenosis in acute ischemic stroke: a cross-sectional study. Front Neurol. 2021;12:714098. doi:10.3389/fneur.2021.714098
- Shi Y, Zhou W, Cheng M, et al. Association of plasma bilirubin levels with peripheral arterial disease in Chinese hypertensive patients: new insight on sex differences. Front Physiol. 2022;13:867418. doi:10.3389/fphys.2022.867418
- Zuo L, Huang J, Zhang H, et al. Dose-response association between bilirubin and cardiovascular disease: a systematic review and meta-analysis. Angiology. 2022;73(10):911–919. doi:10.1177/00033197211059693
- Lan Y, Liu H, Liu J, et al. The relationship between serum bilirubin levels and peripheral arterial disease and gender difference in patients with hypertension: BEST study. Angiology. 2020;71(4):340–348. doi:10.1177/0003319719900734
- Fukui M, Tanaka M, Shiraishi E, et al. Relationship between serum bilirubin and albuminuria in patients with type 2 diabetes. Kidney Int. 2008;74(9):1197–1201. doi:10.1038/ki.2008.398
- Katoh T, Kawamoto R, Kohara K, et al. Association between serum bilirubin and estimated glomerular filtration rate among diabetic patients. Int Sch Res Notices. 2015;2015:480418. doi:10.1155/2015/480418
- Chen J, Liu Q, He J, et al. Immune responses in diabetic nephropathy: pathogenic mechanisms and therapeutic target. Front Immunol. 2022;13:958790. doi:10.3389/fimmu.2022.958790
- Yang J, Liu Z. Mechanistic pathogenesis of endothelial dysfunction in diabetic nephropathy and retinopathy. Front Endocrinol (Lausanne). 2022;13:816400. doi:10.3389/fendo.2022.816400
- Hussein MM, Mahfouz MK. Effect of resveratrol and rosuvastatin on experimental diabetic nephropathy in rats. Biomed Pharmacother. 2016;82:685–692. doi:10.1016/j.biopha.2016.06.004
- Dugbartey GJ, Alornyo KK, Diaba DE, et al. Activation of renal CSE/H2S pathway by alpha-lipoic acid protects against histological and functional changes in the diabetic kidney. Biomed Pharmacother. 2022;153:113386. doi:10.1016/j.biopha.2022.113386
- Baranano DE, Rao M, Ferris CD, et al. Biliverdin reductase: a major physiologic cytoprotectant. Proc Natl Acad Sci USA. 2002;99(25):16093–16098. doi:10.1073/pnas.252626999
- Fujii M, Inoguchi T, Sasaki S, et al. Bilirubin and biliverdin protect rodents against diabetic nephropathy by downregulating NAD(P)H oxidase. Kidney Int. 2010;78(9):905–919. doi:10.1038/ki.2010.265
- Tran DT, Jeong YY, Kim JM, et al. The anti-inflammatory role of bilirubin on “Two-Hit” sepsis animal model. Int J Mol Sci. 2020;21(22):8650. doi:10.3390/ijms21228650
- Dekker D, Dorresteijn MJ, Pijnenburg M, et al. The bilirubin-increasing drug atazanavir improves endothelial function in patients with type 2 diabetes mellitus. Arterioscler Thromb Vasc Biol. 2011;31(2):458–463. doi:10.1161/ATVBAHA.110.211789
- Silveira Rossi JL, Barbalho SM, Reverete de Araujo R, et al. Metabolic syndrome and cardiovascular diseases: going beyond traditional risk factors. Diabetes Metab Res Rev. 2022;38(3):e3502. doi:10.1002/dmrr.3502
- Yardeni D, Toledano R, Novack V, et al. The association of alanine aminotransferase levels with myocardial perfusion imaging and cardiovascular morbidity. J Cardiovasc Pharmacol Ther. 2022;27:10742484221074585. doi:10.1177/10742484221074585
- He S, Li Y, Li T, et al. Sex differences between serum total bilirubin levels and cognition in patients with schizophrenia. BMC Psychiatry. 2021;21(1):396. doi:10.1186/s12888-021-03407-8
- Gerges SH, El-Kadi AOS. Sex differences in eicosanoid formation and metabolism: a possible mediator of sex discrepancies in cardiovascular diseases. Pharmacol Ther. 2022;234:108046. doi:10.1016/j.pharmthera.2021.108046
- Wang M, Gan W, Kartsonaki C, et al. Menopausal status, age at natural menopause and risk of diabetes in China: a 10-year prospective study of 300,000 women. Nutr Metab. 2022;19(1):7. doi:10.1186/s12986-022-00643-x
- Luo W, Gong L, Chen X, et al. Lifestyle and chronic kidney disease: a machine learning modeling study. Front Nutr. 2022;9:918576. doi:10.3389/fnut.2022.918576