
Abstract
Diabetes mellitus (DM) is one of the most common diseases all over the world. The effect of this endocrine disease on body systems cannot be ignored, where its oral side effects are well distinguished. As this disease incident is increasing dramatically, it is essential for the health care providers to be fully aware of the disease diagnosis, management and to deal with it in a full confident. This review discusses the disease itself, its complications, methods of diagnosis as well as its management. Furthermore, oral manifestations and dental considerations that should be followed when treating patients with diabetes mellitus have been discussed in this review.
Introduction
Diabetes mellitus (DM) is a group of metabolic multisystem diseases characterized by hyperglycemia as caused by the relative or absolute deficiency of insulin.Citation1 The high blood sugar causes an osmotic diuresis leading to the typical symptoms of thirst, polyuria, nocturia, weakness, and weight loss.Citation2 Three main types of diabetes include type 1, type 2, and gestational diabetes. Type 1 is caused by an autoimmune process with a sudden onset and requires insulin therapy.Citation3 Type 2 can be undiagnosed and unnoticed for years and may not warrant treatment with insulin. Gestational diabetes arises in pregnancy and can lead to serious risks to the infant and the mother and, later in life, it may also increase the risk of developing type 2 DM.Citation3 Types 1 and 2 DM can have common features including excessive urination (polyuria), excessive thirst (polydipsia), and excessive hunger (polyphagia).Citation4
DM is considered the most common cause of hospital admission.Citation5 Despite DM affecting less than 10% of the general population in some countries, 30% of primary healthcare visits are due to DM.5
In 2017, the International Diabetes Federation Atlas reported that 451 million people (age between 18 and 99 years) were living with diabetes and around 49.7% were undiagnosed.Citation6 It has been stated that there is a chance of increasing the prevalence of DM by 55% in 2023.Citation6 Type 1 DM is less common than type 2 DM. Still, it is increasing each year in both poor and rich countries. In rich countries, most young, diabetic individuals or children have type 1 DM.Citation3,Citation6 Due to worldwide economic development, increased urbanization, people living longer, changes in diet, low level of physical activities, unhealthy behaviors, and other changes in lifestyle patterns, the number of people with type 2 DM is increasing rapidly.Citation3,Citation6 Diabetes is a chronic metabolic disorder that is of significant public health concern.Citation7–9 This review discusses the disease itself, its complications, methods of diagnosis as well as its management. Furthermore, oral manifestations and dental considerations that should be followed when treating patients with diabetes mellitus have been discussed in this review.
Classification
In 2010 and 2013, Wilson et al and Aguirre et al have classified DM into four main categories. They include Type 1 DM, type 2 DM, gestational DM and other causes. Firstly, a total destruction of B-cell which leads to severe deficiency in insulin secretion is referred to type 1. Secondly, type 2 could be as a result of deficiency in the amount of insulin secreted or the cells are poorly responding to this hormone. Thirdly, pregnant women can be affected by diabetes during second and third trimester. Finally, there are varieties of diabetes due to other causes. They represent themselves as monogenic diabetes syndromes and genetic defects, disease of exocrine pancreas and drug, eg, cyclosporine or chemical diabetes.
In addition, according to the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus, 1998 DM was classified based on its aetiology. DM is divided into primary and secondary. Primary DM involves type 1 and type 2. Primary diabetes includes type 1 and type 2 where type 1 can involve type A immune mediated or type B idiopathic DM. Type 2 DM includes insulin resistance and an insulin secretory defect.Citation10 Secondary diabetes can take place as a result of multiple reasons such as pancreatic disease, hormonal abnormalities, severe illness, or other disorders such as gestational diabetes. Moreover, genetic syndromes, drug therapy, autoimmune endocrinopathies, and insulin resistance can lead to secondary diabetes.Citation10
Prevalence and Incidence
According to national diabetes statistics report in 2020, around 10.5% of US population with all ages was diagnosed with DM in 2018. However, adults who are aged 18 years and above showed 13% of US population with DM. Moreover, undiagnosed DM was noticed in 21.4% among adults.Citation11 gives statistics of adults (40 years and above) with diagnosed, undiagnosed DM in US in 2018. shows distribution of people who are affected by DM according to age and race in 2017–2018.
Figure 1 Prevalence of adults 18 years and above who are diagnosed with DM and their distribution according to age and ethnicity in 2017–2018.
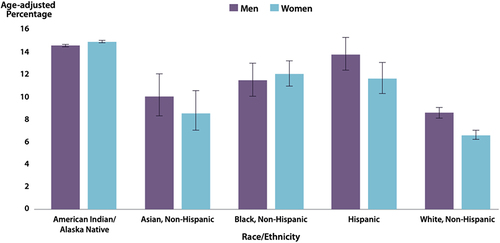
Table 1 Total Numbers Were Calculated from 2013–2016 to July 2018 of All US Residents
Incidence of DM
Incidence means number of new cases of DM that take place at specific time. According to National Health Interview Survey and 2018 US Census Bureau data, people who are aged 45 years old to 64 years old registered the highest incidence of DM and males were more than females. Regardind the race, White, non hispanic had the lowest incidence by 5.4 compared to Hispanic in which they had the highest incidence 9. exhibits the incidence of people who are diagnosed with DM among adults (18 years and above) in 2017–2018 in US population.Citation11 These data were delivered from the National Health Interview Survey and 2018 US Census Bureau data.
Table 2 Distribution of US Population According to Demographic Data
Epidemiology
It has been reported that DM is the most common reason behind hospital admission. It was mentioned that even though DM can affect less than 10% of general population, 30% of people visiting healthcare centers is due to DM.Citation5 The International Diabetes Federation Atlas in 2013 reported that 382 million people were living with diabetes and around 46% were undiagnosed. The number of people with diabetes varies according to the region.Citation13 shows the number of people with DM in 2013 and the percentage of increase in disease by 2035 according to the region.
Table 3 Shows the Number of People with DM in 2013 and the Percentage of Increase in Disease by 2035 According to the Region
Type 1
It has been stated that type 1 DM is less than type 2. According to NHS report in 2014, type 1 DM represents around 10% of total number of this disease. Internationally, there is increasing in type 1 DM by 2–5% per year. Scandinavia revealed the highest prevalence of DM, which is approximately 20%. In contrast, the lowest prevalence of DM type 1 is in Japan and China with less than 1% of the total number of people with diabetes type 1.Citation14
Type 1 DM is less common than type 2 DM. Still, it is increasing each year in both poor and rich countries. In fact, in rich countries, most of young diabetic individuals or children have type 2 DM.Citation3 In the UK, type 1 accounts for 10% of the total number of DM (NHS, 2014). According to Imkampe in 2011, internationally the rates of type 1 DM are increasing by 2–5% per year. The highest prevalence is in Scandinavia, which is approximately 20% of the total number of people with DM. On the other hand, the lowest prevalence of DM type 1 is in Japan and China, accounting for less than 1% of the total number of people with diabetes type 1.Citation10
Males are more affected with DM than females with a ratio 1.5:1. Non-Hispanic whites, Hispanic Americans and African Americans are more commonly affected, respectively. Although DM type 1 is increasing all over the world, the reason is still unknown. It could be due to environmental risks, diet, intra-uterine disturbances or viral infection.Citation3
Type 2
Type 2 DM is more common than type 1 DM and it accounts for around 85–95% of patients with DM (NHS, 2014). Age plays an essential role in developing DM type 2. It can be seen in adults who are 40 years and older.Citation15
There are several reasons behind this increasing percentage. They include economic development, aging, inactive lifestyle, low physical activities and unhealthy behaviors.Citation3 Moreover, women who are diagnosed with gestational DM are more commonly affected with DM type 2, individuals with high blood pressure or dyslipidemia. Certain ethnic groups such as African American, Hispanic/Latino, Native American, and Asian American.Citation16
With regard to prediabetes, it becomes a major global concern since glycemic levels are increasing in both developed and developing countries. A rise in prediabetes percentage can take place as a result of increase in glycaemia levels. Fasting plasma glucose (FPG) exhibited its highest mean in Oceania (6.1 mmol/L for men and women). Moreover, some other areas showed also high FPG such as South and Central Asia, Latin America, the Caribbean, North Africa, and the Middle East.Citation17
According to Centers for Disease Control and Prevention, the statistics of prediabetes among US population from 2017 to 2020 were as the followings; 38% of adults (18 years and above) had prediabetes, and this result was based on their fasting glucose or A1C level. Nineteen percent of people with prediabetes have informed by their healthcare professional that they have this condition. With regard to the gender, fasting glucose or A1C revealed higher percentages among males (41%) than females (32%). Race/ethnicity and education level did not have any significant difference in the prevalence of prediabetes. Likewise, age did not have a considerable influence on the prevalence of prediabetes. Only one-third of US adults had prediabetes during the period 2005–2008 to 2017–2020.Citation18
Pathogenesis
Diabetes Mellitus can be a result of two main pathophysiologic processes. A deficiency in insulin secretion is considered the most common one. The second process is that the mechanism of insulin action does not work properly; therefore, there is increase in insulin secretion as a compensatory mechanism. Genetic defects or environmental reasons or both can lead to insulin resistance.Citation19
It is important to have glucose level in the normal range, thus a reverse relationship between insulin secretion and insulin sensitivity. For normal glucose tolerant people, if insulin level drops below the fifth percentile, hyperglycemia will be developed. For individuals who are having a regular insulin sensitivity, DM will be developed if there is a total absence in insulin production (type 1). In contrast, insulin resistance can result in DM even if there is insulin secretion.Citation19
It has been observed that a direct relationship between high blood glucose level and physiological and behavioural reactions. Hyper-glycemia triggers the brain to release signals to pancreas and other involved organs to reduce their effect.Citation19
Type 1 DM
The pathogenesis of type 1 DM represents itself as destruction of insulin producing cells as a result of autoimmune disease. Macrophages, CD4+ and CDB+ T cells are the main cells that are involved in this mechanism.Citation20
The majority of patients who are diagnosed with type 1 DM have circulating anti-insulin antibodies that can be detected even before receiving insulin therapy. The glutamic acid decarboxylase that is located within pancreatic B cells is targeted by islet cell antibodies.Citation21
As a result of pancreatic β-cells destruction, insulin production is affected which leads to metabolic derangement. Moreover, pancreatic α-cells have also disturbed and show aberrant behaviour in which excessive secretion of glucagon takes place. Physiologically, there is a reverse relationship between hyperglycemia and glucagon production. However, this process is disturbed in patients with type 1 DM in which glucagon level is elevated with hyperglycemia.Citation22
Furthermore, insufficient insulin secretion has a direct effect on metabolism of lipid. This is represented as uncontrolled lipolysis and increased amount of free fatty acids in the plasma, which lead to destruction of glucose metabolism in peripheral tissues such as skeletal muscles.Citation23
Insulin deficiency can cause genetic defect and affect the expression of a number of genes that are essential to help body tissues to respond normally to insulin. Glucokinase in liver and the GLUT 4 class of glucose transporters in adipose tissue are examples which give a sign that insufficient insulin secretion in type 1 DM impairs the metabolism of glucose, lipid and protein.Citation23
Type 2 DM
There are two main pathological mechanisms in type 2 DM. They include disturbances in insulin production and disturbances in insulin work through tissue resistance.Citation10 In case of insulin resistance, alteration on insulin producing cells takes place and thus increase its production to compensate for this resistance.Citation24
Glucose tolerance discrepancy is the outcome of insulin resistance and hyperinsulinemia.Citation25 The situation is different in the case of maturity onset diabetes of the young (MODY) in which the mode of inheritance for type 2 diabetes mellitus is still unclear. MODY is known as “hyper-glycemia diagnosed before the age of twenty-five years and treatable for over five years without insulin in cases where islet cell antibodies (ICA) are negative“.Citation26 It has been mentioned that the reason behind it could be a mutation in glucokinase gene on chromosome 7p.Citation25
Clinical Features and Complications of Diabetes Mellitus
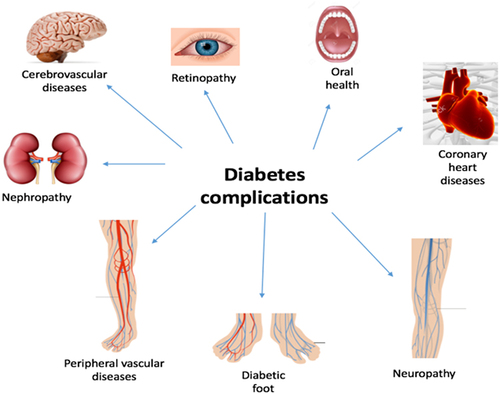
Clinical features of DM vary according to the type and the associated complications. Hyperglycemia manifests as polydipsia, polyuria, weight loss, blurred vision, headache, fatigue, and occasionally polyphagia.Citation27 In addition, impaired growth and liability to infections can be associated with high blood sugar.Citation2,Citation28 Type 1 DM can have sudden onset, and hyperglycemia can progress into ketoacidosis. In essence, long-lasting DM gives rise to an increased risk of atherosclerosis that ultimately affects many key body systems and, in particular, increases the risk of cardiovascular, retinal, and renal diseaseCitation3,Citation6. The complications of DM can provoke damages to multiple organs and systems such as the kidneys, feet, eyes, and heart and can unfortunately lead to early death if not treatedCitation3,Citation6 (). The complications of DM can be classified as acute or chronic.Citation2
Figure 2 Shows major clinical complications of DM on different organs.
Acute and Chronic Complications
DM can cause hypoglycemic or hyperglycemia comas. Hypoglycemia is more common due to a loss of metabolic control in DM related to excess insulin or hypoglycemic drugs, missed meals, unaccustomed exercise, or alcohol consumption.Citation29 DM patients who are treated with insulin are more liable to hypoglycemic coma due to an imbalance between insulin therapy and food intake.Citation4 In hypoglycemia, rapid consciousness is lost and requires rapid treatment to avoid central nervous system (CNS) damage.Citation4,Citation5,Citation29 Hyperglycemia coma is less common than a hypoglycemic episode and has a slower onset not usually associated with loss of consciousness. This type of coma manifests as dehydration, dry skin, weak pulse, hypotension, and hyperventilation of ketosis breath.Citation29,Citation30
Chronic complications of DM are due to microvascular and macrovascular diseases that can affect multiple systems in the body.Citation4 The microvascular damages can include retinopathy, neuropathy, and nephropathy. Macrovascular complications can include strokes, peripheral vascular disease, and ischemic heart disease.Citation4
Diabetic Ketoacidosis
Diabetic ketoacidosis (DKA) is one of the diabetes complications that can lead to death every year. It happens when the plasma glucose level is more than 250 mg per dl or even more. There are several reasons behind this side effect. They represent themselves as decreased insulin levels, reduced glucose use, and increased gluconeogenesis from elevated counter regulatory hormones, including catecholamines, glucagon, and cortisol.Citation31 It has an influence mainly on patients who are diagnosed with type 1 DM, however individuals with type 2 diabetes can be affected too. Following a standard protocol can give a reliable result in managing DKA. It has been stated that patients with DKA can reveal polyuria, polydipsia, polyphagia, and weakness. In addition, 50–80% of them represent nausea and vomiting. Cerebral edema is a serious but uncommon feature that might be observed.
The first step in treating such a complication is diagnosis and management of precipitating factors. They include infection, noncompliance with insulin therapy, myocardial infarction, new-onset diabetes and others.Citation32
Diagnostic Tools
Plasma glucose is used to diagnose diabetes, either by the fasting plasma glucose (FPG) or the 2-hours plasma glucose (2-PG) value after 75 g of an oral glucose tolerance test (OGTT).Citation33 The glycosylated hemoglobin (HbA1C) can also be used to monitor the long-term control of blood glucose level at least for 3 months.Citation33,Citation34 The fructos-amine test is another assay. This gives estimation of a hyperglycemia state over the previous 12–21 days. summarizes the different tests used to diagnose diabetes.Citation35
Table 4 Different Tests and Criteria Used for the Diagnosis of DMCitation36,Citation38
Diagnosis Using Hba1c Test
The HbA1C is used to monitor the long-term control of blood glucose level. The haemoglobin is glycosylated in which the glucose binds to the erythrocytes in a stable process. This haemoglobin remains glycosylated for the full lifespan of the erythrocyte (123 days).Citation23 Therefore, this can give a reflection of the blood glucose level within the last 1–3 months.Citation27
There are several advantages of using the HbA1C in measuring the level of glucose in the blood. They involve no fasting is required and does not alter significantly during illness and stress. On the other hand, it is less sensitive, costly compared to estimated plasma glucose and the relation between the average glucose and the HbA1C is poor.
A survey done by the National Health and Nutrition Examination (NHANES) indicated that one-third fewer cases are diagnosed with a HbA1C cut-off point of ≥48 mmol/L than a fasting glucose cut-off point of ≥7.0 mmol/L.Citation37 Moreover, when the HbA1C is used, features such as age, race, and haemoglobinopathies require to be considered.Citation35
Management of Diabetes Mellitus
The aim of DM management is to prevent DM complications.Citation9,Citation30,Citation38 The optimum control is to keep the glucose levels between 4 and 7 mmol/l (72 −126 mg/dL) before meals and not higher than 10 mmol/l (180 mg/dL) 2 hours after meals.Citation39 The strategy now toward prevention is to obtain effective management. This management can be achieved by both medications and lifestyle modifications.Citation27 Obvious lifestyle changes that are encouraged include avoidance of tobacco, sensible alcohol consumption, weight loss, regular exercise, and diet modification.Citation36 The drugs required for the treatment of DM principally comprise oral hypoglycemic agents and insulin.
Insulin Therapy
A number of different preparations are available for insulin treatment of type 1 DM. Regular basal and bolus dosing plans or continuous pump delivery are commonly employed in a type 1 diabetic patient.Citation5 The different insulin preparations are according to the duration of action as noted in .
Table 5 Types of Insulin and Their Duration of Action
Oral Hypoglycemic Agents
In type 2 DM, oral hypoglycemic agents (OHA) are considered as the first-line treatment. Their mode of action is to either to enhance the action of insulin at target cells or to increase the insulin secretion from the pancreas.Citation5,Citation40 lists the OHA mode of actions.Citation5
Table 6 Commonly Prescribed Oral Hypoglycemic Agents and Their Mode of Actions
Oral Manifestations
There are no specific oral manifestations of DM, although affected individuals may be more prone to infections and have more severe periodontal diseases. A broad spectrum of oral symptoms has been reported in the literature.Citation41,Citation42 DM can give rise to immunological and salivary dysfunction that will increase the risk of common oral diseases such as caries and periodontitis.Citation42 summarizes the oral manifestations of DM.
Table 7 Oral Manifestations of DM and Their Etiology and Associated Risks
Salivary Dysfunction
Salivary dysfunction that changes in the quantity or quality of the salivary protection can consequently affect oral health. Xerostomia has been massively reported in the literature due to the impaired function of the gland as a result of the dehydration because of hyperglycemia and peripheral autonomic neuropathy.Citation9,Citation29,Citation41 Xerostomia is a common complaint of patients with DM, but the exact reason is not completely known.Citation27 Symptoms of dry mouth may reflect an increased glucose level that leads to a more viscous consistency of saliva.Citation27 Unrelated to the symptoms of xerostomia, sialosis can arise in which there is enlargement of the glands due to acinar cell enlargement.Citation43
In DM, thirst, dehydration, oral sensory dysfunction, altered saliva composition, and reduced salivary flow can cause xerostomia.Citation42 In literature, studies have showed that as HbA1c values increase, there is a trend toward decreased salivary flow rate.Citation15 As a consequence of xerostomia, irritation of the oral soft tissue may occur leading to inflammation and pain. In addition, chronic complications of DM such as endothelial dysfunction, microvascular complication, and neuropathy can affect the microcirculation and deteriorate the salivary flow and composition.Citation44
Dental Caries
The association between diabetes and dental caries is complex. No specific connection has been identified, and data are conflicted in this issue. There is no evidence that DM does increase the risk of dental caries.Citation12 Dentists should be aware that salivary dysfunction can reduce the salivary output in conjunction with a high content of glucose in saliva, which can subjectively increase the incidence of caries.Citation4,Citation27 Research has shown that in the presence of standard oral health prevention with a good diabetic control, patients with diabetes are not a higher risk of developing caries in comparison to the general population.Citation27 Diabetic patients might have more dental caries due to poor oral hygiene or a higher number of meals a day.Citation12 In addition, type 2 DM children are exposed to a diet higher in carcinogens compared to type 1 DM children. This is due to the association between obesity and type 2 DM. This can increase the prevalence of caries amongst children with type 2 DM. Neuropathy can diminish the salivary flow rate and increase the risk of developing caries because of dry mouth, but this is not consistent in literature.Citation12 Also, the buffering capacity of saliva in patients with DM is diminished, leading to a higher risk of developing dental caries.Citation44
Oral Infections and Other Oral Mucosal Diseases
A number of different oral mucosal disorders can arise in patients with DM, but the frequency of such lesions in DM is low. Oral lichen planus can arise as a consequence of sulfonylurea therapy, while candida infection manifests as pseudomembranous candidiasis or median rhomboid glossitis can occasionally occur.Citation4 The former may reflect impaired phagocytic function due to a lack of compliance with, or inappropriate insulin therapy.Citation4,Citation27,Citation44 There have been a number of reports of geographic tongue (erythema migrans) in patients with DM, but the vast majority of individuals with this oral disorder do not have DM.Citation12
Periodontal Disease
Gingival and periodontal diseases are more common in patients with DM. It is considered the main oral problem as observed by dental professionals. Based on a literature review of 17 cross-sectional studies that evaluated the relationship between periodontal diseases and diabetes, it was reported that there is increased risk, prevalence, severity, extent, or progression of periodontal diseases. Besides, poor control of DM is associated with severe periodontitis compared to those without diabetes.Citation45,Citation46 Periodontal diseases are a well-documented and well-recognized complication of DM.Citation47 This evidence base is supported by epidemiological data and studies on animal models. This also helped explaining the pathophysiology of periodontal diseases in DM.Citation12,Citation48
In the presence of periodontal diseases, bacteremia can cause an elevated and chronic systemic inflammatory response. This can be associated with increased serum C-reactive protein, cytokine levels, and interleukin-6.Citation27 Diabetic and non-diabetic patients with periodontitis have differences in their subgingival microflora that can alter the inflammatory response.Citation1,Citation27 In addition, reduced collagen metabolism and high levels of local pro-inflammatory mediators can be found in diabetic patients.Citation27 The higher response of macrophage phenotype and compromised neutrophil function can be found in DM patients with periodontitis in comparison with a healthy individual with periodontitis.Citation1,Citation27 Also, high levels of glucose in the crevicular fluid can increase the bacterial existence in the periodontal pocket.Citation1 These two conditions, the inflammatory response and bacterial existence, are reciprocal and are part of periodontitis in DM.Citation27,Citation46 When DM is poor, there is a greater risk of acquiring periodontal disease.Citation5 It was reported that periodontal diseases might lead to poor metabolic control.Citation12,Citation47–49 In addition, periodontal diseases are the sixth complication type associated with DM after retinopathy, nephropathy, neuropathy, peripheral diseases, and cardiovascular diseases.Citation5,Citation46 It is well described that poorly controlled diabetes can increase the incidence of gingival inflammation and alveolar bone loss.Citation1,Citation50 The pathophysiology of this mechanism is similar to the microvascular and macrovascular pathophysiological complications of DM.Citation15,Citation27 The evidence of the effect of periodontal disease on the glycemic control is poor. However, compared to individuals with healthy periodontal tissues, people with periodontal diseases and type 1 or type 2 DM have a greater risk of DM-related complications.Citation51
Impaired Wound Healing
The exact pathogenesis of delayed healing in diabetic patients is poorly understood.Citation1 Abnormal keratinocyte and fibroblast migration, proliferation, differentiation, and apoptosis can contribute to impaired wound healing. In addition, decreased vascularization, impaired function of endothelial progenitor cells (EPCs) and mesenchymal stem cells (MSCs), and abnormal polarization of macrophages can be part of the complex factors involved in delayed wound healing. Furthermore, it has been reported that patients with DM had a prolonged expression of TNF- αα that cause impaired healing.Citation52 It is supposed that diabetic patients have altered homeostasis and impaired phagocyte/macrophage function due to high levels of matrix metallo-proteinases that can contribute to delayed wound healing.Citation27,Citation44
Taste and Other Neurosensory Disorders
Taste is a complex symptom, and it might be related to changes in diet and salivary flow alterations associated with the disease management.Citation46 One in three adults with DM can have hypogeusia. Consequently, it can affect 80% and 50% of individuals with uncontrolled and controlled type 2 DM.Citation53 Taste alteration can affect the salty, sweet, and sour flavors. In the literature, there is no relation between the severity of gustatory impairment and the HbA1c levels.Citation53 Other neurosurgery disorders reported by diabetic patients are burning mouth syndrome and dysphagia. However, the prevalence of this data is not available.Citation5,Citation12
Trigeminal Neuropathy
In literature, DM can affect the function of the trigeminal nerve. In a study of 40 patients with trigeminal neuralgia (TN), 48% had DM. Another study reviewed 30 patients with TN, and 10 out of these patients had an elevated blood glucose level. Therefore, DM can cause TN.Citation54
Special Implications for Dentistry
Access
Patients with diabetic foot ulcers and retinopathy as chronic complications of DM can have compromised access. Such as in complications of advanced nephropathy, access can be compromised due to dialysis. In type 2 DM, increased body weight can compromise access.Citation35 Loss of pain in distal extremities in DM patients can affect the access of the patient. Thus, joint flexibility can impact dental treatment and, if any dental procedure requires prolonged treatment, breaks should be allowed so the patient can move the stiff joint.
Communication
Communication is mainly affected in the case of retinopathy that can lead to blindness. In addition, the association of other comorbidities can affect the function of the brain such as stroke or dementia and compromise communication. Therefore, if there are retinopathy associated complications, communication aids should be considered such as braille or large fonts for documents.Citation8
Consent
In situations where a patient with DM is in a coma due to hyperglycemia or loss of consciousness in hypoglycemia, they can have altered capacity. This can affect a patient’s capacity and complicate consent. Therefore, the national legal regulations should be considered when obtaining consent.Citation55
Education
Good oral hygiene measures should be in place to reduce the risk of oral infections in diabetic patients.Citation56 The International Diabetes Federation Atlas recommends an annual review of the patients’ compliance with daily dental care, the patients’ regular checkups with the dental professional, and awareness of the patients’ regarding the symptoms of gum diseases such as red, swollen, or bleeding gums.Citation44 It is also advisable to educate the patients of the implication of diabetes on oral health and gum disease in particular if the diabetes is poorly controlled.Citation46 If blood glucose levels are poorly controlled, infectious diseases are therefore more common and insulin sensitivity is reduced.Citation15,Citation44,Citation45
Dentists can play an important role in the preventive aspects of DM. They can screen and diagnose periodontal disease in diabetic patients and assess the general population who are at risk of developing diabetes.Citation5,Citation27
Surgical and Operative Dentistry: Challenges and Solutions
Surgical intervention in patients with DM can include the risk of infection and delayed healing due to impaired immunity. This can be managed by performing any dental procedure as atraumatic as possible by using chlorhexidine mouthwash (0.2%) and ensuring that controlled blood sugar levels are in place pre-operatively.Citation28 Therefore, liaising with the diabetic team is necessary to ensure all precautions are in place. This can include obtaining the profile of the blood glucose level of the patient and discussing the planned dental procedure with the diabetic team to consider the need for any antibiotics pre- or post-operatively.Citation5,Citation9
Hypoglycemia is the major issue and risk that most dentists will confront when treating diabetic patients. This is particularly an issue if diabetic patients are asked to fast before any procedure such as general anesthesia or receiving insulin therapy.Citation28 In addition, long dental procedures that may disturb regular food regimes or any procedures that require sedation or systematic anesthesia are associated with high-risk of hypoglycemia. All dental staff should be well trained to manage such an emergency.Citation57 A full awareness of the signs and symptoms of hypoglycemia such as unusual behavior should raise suspicion in staff, and proper management should be implemented before becoming unconscious.Citation5 Every practice should have a detailed and effective emergency management protocols, and all members of staff should be confident enough to treat any suspected emergency.Citation57
Hyperglycemia or ketoacidosis is considered rare compared to hypoglycemia. It is sensible that if blood glucose levels are high enough that dental treatment should be postponed until reasonable blood glucose levels are achieved.Citation5,Citation38
Blood glucose levels should be monitored before any procedure.Citation5 Blood glucose levels should be as close as possible to normal. The blood glucose targets for non-diabetic, type 1 DM, type 2 DM, and pregnant women with diabetes are summarized in .
Table 8 Targeted Blood Glucose levelsCitation36,Citation58
A multidisciplinary care pathway is essential to allow a professional and effective management with no associated risks that can alter the safety of treatment provided. Dental care providers should always have a clear appreciation of a patient’s diabetic status, seek additional advice when necessary (eg, liaise with the patient’s general medical practitioner), and modify clinical care procedures when necessary.Citation5,Citation27,Citation39 Postoperative instructions should necessitate the importance of well-controlled blood glucose levels during the healing period to allow infection free and healthy wound healing.
Delivering dental treatment under local anesthesia and conscious sedation can be safe and effective as long as the previous precautions are considered. The main challenge is providing dental treatment under general anesthesia as the patient should fast at least six hours and therefore increase the risk of hypoglycemia. Dental appointment length and time should not interfere with treatment and the control regime of diabetes. Consideration should be reflected to have a stress-free appointment to reduce the incidence of diabetic emergencies. Early morning or early afternoon appointments not interfering with the routine of food and drugs should be considered to reduce the risk of a hypoglycemia emergency.Citation27
Spread
Patients with DM are not at any increased risk of acquisition or carriage of bloodborne viruses (eg, HIV, HCV, or HBV), mycobacteria (eg, mycobacterium tuberculosis), or prion disease. Normal methods of infection control should be employed for the dental management of patients with DM.Citation28
Conclusion
DM is a disease that all members of the dental team should be aware of. It can affect oral health in several ways, and there is a bidirectional relation between glycemic control and oral health status.Citation27 The long-term maintenance of the oral health of patients with DM may ensure better glycemic control as well as delay the painful symptoms that may require clinical invasive care.Citation5,Citation59 As long as dental healthcare providers are aware of the key aspects of how DM may affect oral health and dentistry and take the necessary appropriate actions, it is unlikely that oral health care will increase the morbidity of patients. Central to the care of patients with DM, and indeed individuals with good health, it must be the prevention of commonly acquired oral diseases (eg, caries and periodontitis) that may cause pain, interfere in oral function, lessen quality of life, and require perhaps avoidable invasive dental procedures.Citation1
Dental care providers should always give attention to diabetic patients, seek additional advice if required (eg, liaise with the patient’s general medical practitioner) and modify clinical care procedures when necessary.Citation27,Citation38
As long as dental healthcare providers are aware of the key aspects of how DM may affect oral health and take the necessary appropriate actions – it is unlikely that oral health care will increase the morbidity of patients. Central to the care of patients with DM, and indeed individuals with good health, it must be the prevention of commonly acquired oral diseases (eg, caries and periodontitis) that may cause pain, interfere in oral function, lessen quality of life, and require perhaps avoidable invasive dental procedures.
Ethical Approval
There is no ethical issue.
Disclosure
The author reports no conflicts of interest in this work.
Acknowledgment
I would like to express my sincere gratitude to my friend, Dr. Lama Dakkouri, for her advices and support.
The Following Organizations:
- Centers for Disease Control and Prevention, National Center for Health Statistics
- Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Division of Diabetes Translation
- Indian Health Service, Division of Diabetes Treatment and Prevention
Additional information
Funding
References
- Mealey BL, Oates TW. Diabetes mellitus and periodontal diseases. J Periodontal. 2006;77(8):1289–1303. doi:10.1902/jop.2006.050459
- American Diabetes Association. Classification and diagnosis of diabetes. Diabetes Care. 2017;40(Suppl 1):S11–S24. doi:10.2337/dc17-S005
- Aguirre F, Brown A, Cho NH, et al. IDF diabetes atlas; 2013.
- Wilson MH, Fitpatrick JJ, McArdle NS, Stassen LFA. Diabetes mellitus and its relevance to the practice of dentistry. J Ir Dent Assoc. 2010;56(3):128–133.
- Kidambi S, Patel SB. Diabetes mellitus: considerations for dentistry. J Am Dent Assoc. 2008;139:8S–18S. doi:10.14219/jada.archive.2008.0364
- Ogurtsova K, da Rocha Fernandes JD, Huang Y; Atlas ID. Global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res Clin Pract. 2017;128:40–50. doi:10.1016/j.diabres.2017.03.024
- National Health Service (NHS). Diabetes; 2019. Available from: http://www.nhs.uk/Conditions/Diabetes/Pages/Diabetes.aspx. Accessed March 2, 2020.
- Lalla E, Lamster IB. Assessment and management of patients with diabetes mellitus in the dental office. Dent Clin North Am. 2012;56(4):819–829. doi:10.1016/j.cden.2012.07.008
- Lewis D, Fiske J, Dougall A. Access to special care dentistry, part 7. Special care dentistry services: seamless care for people in their middle years–part 1. Br Dent J. 2008;205(6):305. doi:10.1038/sj.bdj.2008.803
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2010;33(Suppl 1):S62–S69. doi:10.2337/dc10-S062
- Centers for Disease Control and Prevention. National diabetes statistics report, 2020. Atlanta, GA: Centers for Disease Control and Prevention, US Department of Health and Human Services; 2020.
- Lamster IB, Lalla E, Borgnakke WS, Taylor GW. The relationship between oral health and diabetes mellitus. J Am Dent Assoc. 2008;139:19S–24S. doi:10.14219/jada.archive.2008.0363
- Aguirre F, Brown A, Cho NH, et al. IDF Diabetes Atlas. 6th ed. International Diabetes Federation;2013.
- Imkampe AK, Gulliford MC. Trends in Type 1 diabetes incidence in the UK in 0- to 14-year-olds and in 15- to 34-year-olds, 1991–2008. Diabet Med. 2011;28(7):811–814. doi:10.1111/j.1464-5491.2011.03288.x
- Leite RS, Marlow NM, Fernandes JK, Hermayer K. Oral health and type 2 diabetes. Am J Med Sci. 2013;345(4):271–273. doi:10.1097/MAJ.0b013e31828bdedf
- Hutchinson RN, Shin S. Systematic review of health disparities for cardiovascular diseases and associated factors among American Indian and Alaska Native populations. PLoS One. 2014;9(1):e80973. doi:10.1371/journal.pone.0080973
- Danaei G, Finucane MM, Lu Y, et al. National, regional, and global trends in fasting plasma glucose and diabetes prevalence since 1980: systematic analysis of health examination surveys and epidemiological studies with 370 country-years and 2·7 million participants. Lancet. 2011;378(9785):31–40. doi:10.1016/S0140-6736(11)60679-X
- Centers for Disease Control and Prevention. Prevalence of prediabetes among adults. Available from: https://www.cdc.gov/diabetes/data/statistics-report/prevalence-of-prediabetes.html. Accessed September 29, 2023.
- Baynes HW. Classification, pathophysiology, diagnosis and management of diabetes mellitus. J Diabetes Metab. 2015;6(5):1–9.
- Al Homsi MF, Lukic ML. An update on the pathogenesis of diabetes mellitus. Dubai Diabetes Endocrinol J. 1993;1:1–2.
- Raju SM, Raju B. Illustrated Medical Biochemistry. 2nd ed. New Delhi, India: Jaypee Brothers Medical Publishers ltd; 2010.
- Holt RI. Diagnosis, epidemiology and pathogenesis of diabetes mellitus: an update for psychiatrists. Br J Psychiatry Suppl. 2004;47:S55–S63. doi:10.1192/bjp.184.47.s55
- Mealey BL, Ocampo GL. Diabetes mellitus and periodontal disease. Periodontol 2000. 2007;44:127–153. doi:10.1111/j.1600-0757.2006.00193.x
- Kumar PJ, Clark M. Textbook of Clinical Medicine. London, UK: Saunders; 2002.
- Mahler RJ, Adler ML. Clinical review 102: type 2 diabetes mellitus: update on diagnosis, pathophysiology, and treatment. J Clin Endocrinol Metab. 1999;84(4):1165–1171. doi:10.1210/jcem.84.4.5612
- Sekikawa A, Tominaga M, Takahashi K, et al. Prevalence of diabetes and impaired glucose tolerance in Funagata area, Japan. Diabetes Care. 1993;16(4):570–574. doi:10.2337/diacare.16.4.570
- Mohamed K, Yates J, Roberts A. Diabetes mellitus: considerations for the dental practitioner. Dent Update. 2014;41(2):144–154. doi:10.12968/denu.2014.412.144
- Maranta F, Cianfanelli L, Cianflone D. Glycaemic control and vascular complications in diabetes mellitus type 2. Adv Exp Med Biol. 2021;1307:129–152. doi:10.1007/5584_2020_514
- Scully C. Medical Problems in Dentistry E-Book. 7th ed. Elsevier Health Sciences; 2015.
- American Diabetes Association. Standards of medical care in diabetes-2015 abridged for primary care providers. Clin Diabetes. 2015;33(2):97–111. doi:10.2337/diaclin.33.2.97
- Trachtenbarg DE. Diabetic ketoacidosis. Am Fam Physician. 2005;71(9):1705–1714.
- Kitabchi AE, Umpierrez GE, Murphy MB, et al. Hyperglycemic crises in diabetes. Diabetes Care. 2004;27(Suppl 1):S94–S102. doi:10.2337/diacare.27.2007.s94
- Gillett M. International expert committee report on the role of the A1C assay in the diagnosis of diabetes. Clin Biochem Rev. 2009;32(7):1327–1334. doi:10.2337/dc09-9033
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2014;37(Suppl 1):S81–S90. doi:10.2337/dc14-S081
- American Diabetes Association. Standards of medical care in diabetes—2016 abridged for primary care providers. Clin Diabetes. 2016;34(1):3–21.
- Diabetes UK. Checking your blood sugar levels; 2016. Available from: https://www.diabetes.org.uk/Guide-to-diabetes/Monitoring/Testing/#glucose. Accessed March 2, 2020.
- Cowie CC, Rust KF, Byrd-Holt DD, et al. Prevalence of diabetes and high risk for diabetes using A1C criteria in the U.S. population in 1988–2006. Diabetes Care. 2010;33(3):562–568. doi:10.2337/dc09-1524
- Ali D, Kunzel C. Diabetes mellitus: update and relevance for dentistry. Dent Today. 2011;30(12):45–46.
- Wisconsin Diabetes Prevention and Control. Diabetes; 2015. Available from: https://www.dhs.wisconsin.gov/diabetes/index.htm. Accessed March 2, 2020.
- Nathan DM. Finding new treatments for diabetes—how many, how fast. how good? N Engl J Med. 2007;356(5):437–440. doi:10.1056/NEJMp068294
- Manfredi M, McCullough M, Vescovi P, Al‐Kaarawi Z, Porter S. Update on diabetes mellitus and related oral diseases. Oral Dis. 2004;10(4):187–200. doi:10.1111/j.1601-0825.2004.01019.x
- Priya BM, ShivaKumar V, Anitha V, Shanmugam M. Diabetes & dental diseases. CHC Med J. 2012;1(4):188–191.
- Mandel L, Khelemsky R. Asymptomatic bilateral facial swelling. J Am Dent Assoc. 2012;143(11):1205–1208. doi:10.14219/jada.archive.2012.0065
- Al-Maskari AY, Al-Maskari MY, Al-Sudairy S. Oral manifestations and complications of diabetes mellitus: a review. Sultan Qaboos Univ Med J. 2011;11(2):179.
- D’Aiuto F. Guideline on oral health for people with diabetes. Available from: https://www.idf.org/e-library/. Accessed September 29, 2023.
- Preshaw P, Alba A, Herrera D, et al. Periodontitis and diabetes: a two-way relationship. Diabetologia. 2012;55(1):21–31. doi:10.1007/s00125-011-2342-y
- Chapple IL, Genco R; Working group 2 of the joint EFP/AAP workshop. Diabetes and periodontal diseases: consensus report of the joint EFP/AAP workshop on periodontitis and systemic diseases. J Periodontal. 2013;84(4 Suppl):S106–12. doi:10.1902/jop.2013.1340011
- Pontes Andersen CC, Flyvbjerg A, Buschard K, Holmstrup P. Relationship between periodontitis and diabetes: lessons from rodent studies. J Periodontol. 2007;78(7):1264–1275. doi:10.1902/jop.2007.060491
- Taylor GW, Borgnakke W. Periodontal disease: associations with diabetes, glycemic control and complications. Oral Dis. 2008;14(3):191–203. doi:10.1111/j.1601-0825.2008.01442.x
- Campus G, Salem A, Uzzau S, Baldoni E, Tonolo G. Diabetes and periodontal disease: a case‐control study. J Periodontol. 2005;76(3):418–425. doi:10.1902/jop.2005.76.3.418
- Borgnakke WS, Ylöstalo PV, Taylor GW, Genco RJ. Effect of periodontal disease on diabetes: systematic review of epidemiologic observational evidence. J Periodontol. 2013;84(4 Suppl):S135–S52. doi:10.1902/jop.2013.1340013
- Xu F, Zhang C, Graves DT. Abnormal cell responses and role of TNF-in impaired diabetic wound healing. BioMed Res Int. 2013;2013:754802. doi:10.1155/2013/754802
- Imoscopi A, Inelmen EM, Sergi G, Miotto F, Manzato E. Taste loss in the elderly: epidemiology, causes and consequences. Aging Clin Exp Res. 2012;24(6):570–579. doi:10.3275/8520
- Sabalys G, Juodzbalys G, Wang H-L. Aetiology and pathogenesis of trigeminal neuralgia: a comprehensive review. J Oral Maxillofac Res. 2012;3(4):e2. doi:10.5037/jomr.2012.3402
- Johnston C, Liddle J. The mental capacity act 2005: a new framework for healthcare decision making. J Med Ethics. 2007;33(2):94–97. doi:10.1136/jme.2006.016972
- Alzahrani AS, Abed HH. To what extent should dental implant placement be adopted as a standard for diabetic patients? Saudi Med J. 2016;37(11):1179. doi:10.15537/smj.2016.11.15512
- Jevon P. Resuscitation in the dental practice. Br Dent J. 2016;220(5):261–263. doi:10.1038/sj.bdj.2016.181
- National Institute for Health and Care Excellence (NICE). Diabetes; 2015. Available from: https://www.nice.org.uk/guidance/conditions-and-diseases/diabetes-and-other-endocrinal--nutritional-and-metabolic-conditions/diabetes?unlid=2396662832016122184017. Accessed March 2, 2020.
- Kim J, Amar S. Periodontal disease and systemic conditions: a bidirectional relationship. Odontology. 2006;94(1):10–21. doi:10.1007/s10266-006-0060-6