Abstract
The glucagon-like peptide (GLP)-1 receptor agonist lixisenatide (Lyxumia®) was approved for marketing by the European Medicines Agency in February 2013 and has been evaluated in a clinical study program called GetGoal. Lixisenatide activates the GLP-1 receptor and thereby exercises the range of physiological effects generated by GLP-1, which consist of increased insulin secretion, inhibition of glucagon secretion, and decreased gastrointestinal motility alongside the promotion of satiety. In the GetGoal study program, lixisenatide demonstrated significant reductions in glycated hemoglobin (HbA1c), and fasting and postprandial plasma glucose compared with placebo. The effect on glycemia was evident, with both monotherapy and in combination with insulin and various oral antidiabetic agents. Furthermore, a general trend towards reduced bodyweight was reported. In head-to-head trials with the other GLP-1 receptor agonists (exenatide and liraglutide) on the market, lixisenatide demonstrated a superior effect with respect to reduction in postprandial plasma glucose and had a tendency towards fewer adverse events. However, lixisenatide seemed to be less efficient or at best, equivalent to exenatide and liraglutide in reducing HbA1c, fasting plasma glucose, and bodyweight. The combination of a substantial effect on postprandial plasma glucose and a labeling with once daily administration separates lixisenatide from the other GLP-1 receptor agonists. The combination of basal insulin, having a lowering effect on fasting plasma glucose, and lixisenatide, curtailing the postprandial glucose excursions, makes sense from a clinical point of view. Not surprisingly, lixisenatide is undergoing clinical development as a combination product with insulin glargine (Lantus®). At present the main place in therapy of lixisenatide seems to be in combination with basal insulin. A large multicenter study will determine the future potential of lixisenatide in preventing cardiovascular events and mortality, in patients with type 2 diabetes and recent acute coronary syndrome.
Keywords:
Pathophysiology of type 2 diabetes mellitus (T2DM) and glycemic control
T2DM is a result of both heritage and environment. The fast-increasing prevalence of T2DM during recent years is, however, mainly seen as a consequence of an evolution towards a sedentary lifestyle and overeating. It is estimated that in 2025, almost 400 million people worldwide will suffer from diabetes, with T2DM comprising more than 90% of the cases.Citation1 T2DM is a multifaceted disease characterized by a disruption of glucose and lipid metabolism, leading to hyperglycemia in both the fasting and postprandial state. It has been suggested that postprandial glycemic excursions play a major role in the metabolic disequilibrium of patients suffering from mild or moderate hyperglycemia, whereas the role decreases as patients progress toward poorer diabetic controlCitation2 – fasting hyperglycemia appears to be a main contributor to the overall hyperglycemia in poorly controlled diabetic patients.Citation2
Subjects with T2DM exhibit peripheral and hepatic insulin resistance, β-cell dysfunction (including an absent early insulin secretory response), reduced β-cell mass, and glucagon hypersecretion.Citation3 The compromized β-cell function seems to be partly due to an impaired response to the incretin hormones glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP).Citation4 T2DM is typically a progressive disease characterized by worsening glycemia, which over time necessitates escalating pharmacotherapy if treatment goals are to be met.Citation5
Patients with T2DM have a reduced life span expectancy of up to 10 years, primarily due to an increased risk of fatal cardiovascular events.Citation6 In order to reduce this risk, it is very important to treat cardiovascular risk factors, such as obesity, hyperlipidemia, and hypertension.Citation7 In addition, it is well established that the risk of microvascular and macrovascular complications is related to overall glycemia, as measured by glycated hemoglobin (HbA1c), and this remains a major focus of therapy.Citation8
A variety of therapeutic options are available for the treatment of hyperglycemia in patients with T2DM. It is generally accepted that the initial therapy should consist of lifestyle changes plus metformin.Citation8 The American Diabetes Association and the European Association for the Study of Diabetes recommends lowering HbA1c to <7.0% in most patients. Furthermore, fasting and premeal glucose should be maintained at <7.2 mmol/L and the postprandial glucose (PPG) at <10 mmol/L.Citation8 These recommendations should be considered within the context of the needs, preferences, and tolerances of each patient. If needed, several different drugs (sulfonylureas, insulin, dipeptidyl peptidase [DPP]-4 inhibitors, and GLP-1 receptor agonists) can be used in combination with metformin to reach an individualized HbA1c target. A general lack of comparative effectiveness research regarding these different antidiabetic drugs makes it difficult to put together a preferred algorithm when considering add-on treatment to metformin.Citation8 All of these agents, used alone or in combination, are associated with different adverse events (eg, hypoglycemia, weight gain, and/or gastrointestinal side effects) that must be taken into account.
Three GLP-1 receptor agonists (GLP-1RAs), exenatide twice daily (Byetta®; Amylin Pharmaceuticals, Inc, San Diego, CA, USA), exenatide once weekly (Bydureon®; Bristol-Myers Squibb, New York, NY, USA and AstraZeneca, London, UK), and liraglutide once daily (Victoza®; Novo Nordisk, Bagsværd, Copenhagen, Denmark) are currently available for the treatment of T2DM. In November 2012, the European Medicines Agency adopted a positive opinion for the new GLP-1RA, lixisenatide (Lyxumia®; Sanofi SA, Paris, France), and this was followed by marketing approval in February 2013.
The aim of this manuscript was to review the clinical data of lixisenatide, identified by searching the US National Institutes of Health registry (ClinicalTrials.gov), and reviewing Medline indexed published articles and scientific meeting posters and abstracts.
The incretin system as a therapeutic target for T2DM
The incretin effect refers to the amplification of insulin secretion elicited by hormones secreted from the gastrointestinal tract.Citation9 The effect is quantified by comparing insulin responses to oral and intravenous glucose administration, in amounts adjusted in order to achieve identical glucose excursions.Citation10 The incretin effect has been shown to account for as much as 50%–70% of insulin secretion following oral glucose ingestion in healthy subjects.Citation11 The incretin effect is markedly reduced in patients with T2DM, and this contributes importantly to the postprandial hyperglycemia seen in these patients.Citation12 In addition to the insulinotropic effect, the incretin hormones have a variety of advantageous effects in relation to the typical phenotype of patients with T2DM, as will be addressed below.
Currently, it is generally agreed upon that the incretin effect is mainly constituted by the two incretin hormones GLP-1 and GIP.Citation13 The effects of the two hormones, with respect to insulin secretion, is additive, and they seem to make an equal contribution to the incretin effect in healthy subjects.Citation14 However, in a study by Nauck et al,Citation15 GIP was reported to make a larger contribution to the incretin effect than GLP-1. The insulinotropic effect of GIP is severely impaired in most patients with T2DM, whereas the effect of GLP-1 is retained at supraphysiological doses,Citation15 thus making GLP-1 interesting as a therapeutic option in T2DM.
GLP-1 is a 30-amino acid polypeptide produced in the endocrine L-cells of the intestinal epithelium, as a product of proglucagon gene expression.Citation16 L-cells are located with the highest density in the ileum and the colon but can be found throughout the intestinal tract.Citation9 GLP-1 is secreted rapidly in response to the ingestion of nutrients, with a noticeable response after 10 minutes.Citation16
The enzyme DPP-4 is responsible for the rapid degradation and inactivation of GLP-1, resulting in a short elimination half-life (t½) of native GLP-1 of 1–1.5 minutes.Citation17 Until now, a number of GLP-1RAs resistant to degradation by DPP-4 have been developed for therapeutic use. Furthermore, several different DPP-4 inhibitors are available for the treatment of patients with T2DM.
GLP-1 augments insulin secretion by the pancreatic β-cells in a glucose-dependent manner and has also been shown to enhance all steps of insulin biosynthesis as well as insulin gene transcription.Citation13 The potentiating effect on insulin release is absent at plasma glucose levels below 4 mM, resulting in a low risk of hypoglycemia.Citation18 In rodents, GLP-1 has trophic effects on β-cells,Citation19 and in isolated human islets, GLP-1 has been demonstrated to inhibit apoptosis of β-cells.Citation20 Glucagon secretion, and thereby, hepatic glucose production, is inhibited by GLP-1.Citation21 Equivalent to the effect on insulin release, the suppression of glucagon secretion is glucose-dependent, and so, GLP-1 has no inhibitory effect on glucagon release at hypoglycemic plasma glucose concentrations, resulting in a preserved counter-regulatory glucagon response to hypoglycemia.Citation18 It seems that the inhibition of glucagon secretion is as clinically important as the insulinotropic effect of GLP-1 for the treatment of hyperglycemia in patients with T2DM.Citation22
Furthermore, GLP-1 decreases gastrointestinal motility, which, in combination with afferent signaling through the vagus nerve and activation of GLP-1 receptors in the central nervous system, promotes satiety and reduces food intake, thereby controlling or even reducing body weight.Citation16,Citation23 The delaying effect of GLP-1 on gastric emptying plays an important role in PPG control following short-term GLP-1 receptor activation.Citation24
Finally, GLP-1 seems to have several beneficial effects in relation to the cardiovascular system. GLP-1 has been shown to improve left ventricular function in the failing and ischemic heart,Citation25,Citation26 to improve endothelial dysfunction in patients with T2DM and coronary heart disease,Citation27 and moreover, seems to increase myocardial salvage after myocardial infarction.Citation28 Additionally, GLP-1 has been found to cause a reduction in the postprandial rise in serum triglycerides and free fatty acids in healthy subjects.Citation29 Furthermore, GLP-1 has been shown to exercise a blood pressure–lowering effect,Citation30 presumably based on both its vasodilatoryCitation31 and diuretic properties.Citation32
Pharmacology of lixisenatide
Lixisenatide is a GLP-1RA for once daily subcutaneous injection, developed by Sanofi under license from Zealand Pharma A/S (Copenhagen, Denmark). As previously described, market authorization approval was granted in February 2013. The peptide is based on the structure of exendin-4 (exenatide) and contains 44 amino acids. The modifications, compared with exendin-4, consist of a deletion of a proline residue and an addition of six lysine residues C-terminally (). The time to maximal plasma concentration (tmax) has been reported to be approximately 2 hours in both healthy subjects and patients with T2DM.Citation33 The mean maximal plasma concentration (Cmax) with the intended 20 μg once daily dosing was demonstrated to be 187 pg/mL,Citation34 and Cmax has been reported to be higher in healthy subjects compared with patients with T2DM.Citation33 Lixisenatide is resistant to cleavage by DPP-4 but is, like native GLP-1, still subject to renal filtration.Citation35 The resulting elimination t½ in plasma is 2–3 hours,Citation34,Citation36 which is similar to the values obtained with exenatide.Citation37 In patients with moderate renal impairment (creatinine clearance 30–50 mL/min), the clearance of lixisenatide is not affected, while in patients with severe renal impairment (creatinine clearance < 30 mL/min, not requiring renal dialysis), clearance is lowered by approximately 30%.Citation38 Lixisenatide has been shown to lower the Cmax and to prolong the tmax of concomitantly administered oral warfarin, acetaminophen, and ethinyl estradiol. However, the extent of absorption (area under curve) was not shown to be significantly affected, which is consistent with a delaying effect on gastric emptying.Citation39,Citation40
Figure 1 Structure of lixisenatide.
Abbreviation: GLP-1, glucagon-like peptide-1.
In early binding studies, lixisenatide demonstrated a fourfold higher affinity for the human GLP-1 receptor when compared with native GLP-1.Citation41 This affinity is claimed to be superior to that of the similar compound exenatide, though no head-to-head trials have been published.Citation42 In a 13-week randomized, placebo-controlled trial, the efficacy of lixisenatide with respect to glycemic control was shown to reach a plateau at a dose of 20 μg once daily.Citation43 The optimal dose of 20 μg once daily differs from the twice-daily administration of exenatide. This suggests a longer duration of action as compared with exenatide despite a similar elimination t½, which could reflect the difference in affinity for the GLP-1 receptor between the two peptides.
Lixisenatide activates the GLP-1 receptor and thereby generates the range of physiological effects generated by GLP-1. As described earlier, these consist of increased insulin secretion, inhibition of glucagon secretion, and decreased gastrointestinal motility alongside the promotion of satiety and several promising cardiovascular effects. Although lixisenatide stimu lates insulin secretion, its marked effect on postprandial blood glucose levels seems mainly to be mediated through the inhibition of gastric emptying.Citation44
Clinical study program
Lixisenatide has been evaluated in a clinical study program entitled GetGoal. Several different studies have now been completed, and many of the results have been published as either abstracts or full-length publications. Furthermore, there are a number of on-going trials for which results are being awaited. An overview of the studies with already published results can be found in . The vast majority of the listed studies had the change in HbA1c from baseline as the primary outcome. HbA1c can be used as an estimate of average blood glucose levels during the preceding 2–3 months.Citation45 Fasting plasma glucose (FPG) and PPG were both frequently listed as secondary outcomes. The change in bodyweight was also an outcome measure in most of the studies. Finally, many of the studies reported safety and tolerability data.
Table 1 An overview of the GetGoal study program
Glycemic control Change in HbA1c
Results from nine studies in the GetGoal program with HbA1c as primary outcome have so far been presented (). The HbA1c at baseline was approximately 8%–8.5% in these studies. In the GetGoal-Duo 1 study, the average HbA1c was initially 8.6% at screening but had decreased to 7.6% at randomization after the run-in treatment with insulin glargine.Citation46 In eight out of nine studies, lixisenatide was compared with placebo. This was done in different regimes with respect to dosage titration and time of day for administration. In the studies, lixisenatide was used as both monotherapy and as add-on to metformin, sulfonylureas, glitazones, insulin, and various combinations of these antidiabetic drugs. The GetGoal-X study compared lixisenatide with exenatide (Byetta) as add-on to metformin.
Table 2 Efficacy outcomes from the GetGoal study program
In these various trials, lixisenatide was shown to reduce HbA1c between 0.32% and 0.88% when compared with placebo. The smallest reductions of 0.32% and 0.36% were seen in the GetGoal-Duo1 and the GetGoal-L study, respectively.Citation46,Citation47 In the GetGoal-Duo 1 study, this could have been due to a lower HbA1c at randomization and additionally, a decrease in the daily basal insulin dose of 2.2 IU in patients treated with lixisenatide as compared with the placebo group. Along these lines, the patients treated with lixisenatide, when compared with controls, either had substantial reductions in daily basal insulin dose (eg, the GetGoal-L, a reduction of 5.6 versus [vs] 1.9 IU) in combination with minor changes in HbA1c, or a smaller reduction in daily basal insulin dose (1.4 vs 0.1 IU) combined with a larger reduction in HbA1c, as observed in the GetGoal-L-Asia study.Citation48
There was no readily apparent correlation between the obtained reductions in HbA1c and the specific combinations of antidiabetic drugs in the nine studies. In general, significantly more patients treated with lixisenatide compared with placebo reached the defined target of HbA1c below 7.0%.
The primary outcome of the GetGoal-X studyCitation49 was to establish the noninferiority of lixisenatide to twice daily exenatide (Byetta) as add-on therapy to metformin, in terms of HbA1c reduction. Both lixisenatide and exenatide reduced HbA1c significantly, by 0.79% and 0.96%, respectively. Thus, despite a statistically significant difference of 0.17% (95% confidence interval: 0.03%–0.30%) in HbA1c reduction, noninferiority was claimed because the upper limit confidence interval for the estimate did not exceed the noninferiority margin of 0.4%. Similar proportions of patients in the two treatment groups achieved the target HbA1c below 7.0% or 6.5%.
In another study, lixisenatide was reported to have a significantly smaller effect on HbA1c compared with liraglutide, with reductions of 0.32% and 0.51% (P < 0.01), respectively.Citation50 However, the duration of this study was only 4 weeks, which could question the relevance of the chosen outcome measures, considering that HbA1c is an estimate of average blood glucose levels over the preceding 2–3 months.
In the GetGoal-M study,Citation51 lixisenatide was administered either before breakfast or dinner in order to assess whether the administration time of day was important for reductions in HbA1c. No significant difference between the two groups treated with lixisenatide at different times was observed, although a tendency towards higher effect with morning administration was seen (HbA1c reduced with 0.49% vs 0.37%).
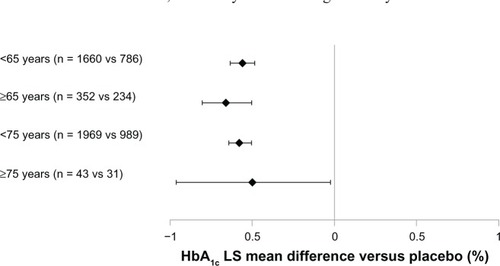
A meta-analysis based on six of the trials from the GetGoal program compared the effect of lixisenatide in different age groups and found comparable and significant HbA1c reductions in all groups ().Citation52
FPG and PPG
A number of studies from the GetGoal program have so far reported results regarding the effect of lixisenatide on FPG and PPG. GetGoal-X has compared lixisenatide with exenatide, whereas treatment with placebo was used as the control in the remaining studies. As previously described, the studies include several different combinations of antidiabetic treatments (see ).
Treatment with lixisenatide, as compared with placebo, generally resulted in a significant decrease in FPG. The obtained range of decrease from baseline was between 0.6 and 1.1 mmol/L. The GetGoal-Duo 1Citation46 was the only placebo-controlled trial with no observed effect of lixisenatide on FPG. In fact, a small rise in FPG was seen in both the treatment and the control groups in this study. It has to be noted that the baseline FPG of 6.6 mmol/L in this study was by far the lowest in the group of trials reporting results on FPG, and this could be an explanation for the absent effect. In comparison, the FPG at baseline was approximately 9.0 mmol/L in the GetGoal-Mono studyCitation53 that had the largest observed decrease (of 1.1 mmol/L) in FPG. In the GetGoal-X study,Citation49 both lixisenatide and exenatide resulted in a significant decrease in FPG, from baselines of 1.2 and 1.4 mmol/L, respectively.Citation49 Thus, no significant difference in effect between the two treatments was observed. In contrast, liraglutide demonstrated a greater reduction in FPG compared with lixisenatide (1.3 vs 0.3 mmol/L) (P < 0.01).Citation50
Results from the GetGoal study program indicate that lixisenatide has a pronounced effect on postprandial glycemic control. Compared with placebo, significant decreases (of 3.2–7.2 mmol/L) in PPG from baseline have been observed. The PPG values were measured 2 hours after a standardized test meal. The lowest reported effect was seen in the GetGoal Duo-1 study. Again, the characteristics of the patients at baseline could at least partly help explain the difference between studies. In the GetGoal Duo-1 study, the average PPG at baseline was 13 mmol/L, whereas the GetGoal-L-Asia study had the largest observed effect on PPG and also had the highest baseline PPG value (of 18 mmol/L).Citation48
A head-to-head trial with the main objective of comparing the effect of lixisenatide and liraglutide on PPG excursions was not part of the original GetGoal program but was also conducted by Sanofi. The patients included in the study had a baseline maximum PPG excursion of 4.9 mmol/L, which was reduced to 1.0 and 3.5 mmol/L (P < 0.01) after treatment with lixisenatide and liraglutide, respectively.Citation50 Furthermore, the area under the plasma glucose concentration curve in a 4-hour period after the start of the standardized breakfast test meal was significantly reduced following treatment with lixisenatide as compared with liraglutide. The study thereby found lixisenatide to have a significantly larger effect on PPG than liraglutide.
A study by Lorenz et al,Citation54 presented at the scientific sessions of the American Diabetes Association 2012 meeting, tested the effect of a morning administration of lixisenatide on postprandial glycemia throughout the day. The largest effect on PPG was seen after breakfast, in accordance with the relatively short elimination t½ of lixisenatide. Although smaller, the effect on PPG observed after lunch and dinner was still improved compared with placebo (). Thus, it seems that lixisenatide exercises the most pronounced effect on PPG following the first meal after administration of the drug. The interpretation of this result was that the marked PPG-effect of lixisenatide mainly reflected the delaying effect on gastric emptying; the same interpretation was put forth and discussed by Distiller and Ruus.Citation34 This suggests a possible advantage of administration of lixisenatide in conjunction with the main meal of the day, an assumption that still needs to be tested in clinical settings. Besides the effect on gastric emptying, lixisenatide also increases first-phase insulin secretion by almost threefold, thereby accelerating glucose disposition in subjects with early-stage T2DM.Citation36 This insulinotropic effect could also contribute to the improvement in postprandial glycemic control seen after treatment with lixisenatide.
Figure 2 Mean blood glucose concentrations in patients with T2DM after administration of lixisenatide or placebo.
Abbreviations: AUC, area under the curve; LS, least squares; QD, once daily; SE, standard error; T2DM, type 2 diabetes mellitus; vs, versus.
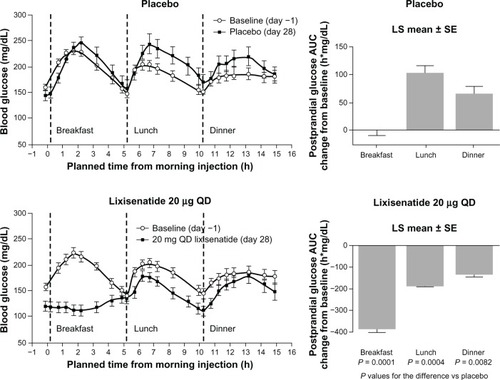
Figure 3 LS mean difference in HbA1c change with lixisenatide versus (vs) placebo from a meta-analysis for the pooled data of six Phase III studies.
Abbreviations: HbA1c, glycated hemoglobin; LS, least squares; mITT, modified intent-to-treat; vs, versus.
Weight
Nine studies in the GetGoal program have so far reported results on change in body weight after treatment with lixisenatide. In these studies, the effect of lixisenatide was compared with both placebo and exenatide. Furthermore, one study has reported results of lixisenatide vs liraglutide, with respect to change in body weight. Body mass index (BMI) at baseline was between 30 and 34 kg/m2, except in the GetGoal-L-Asia study that had an Asian study population with a BMI at baseline of 25 kg/m2 ().
The eight placebo-controlled trials found diverse effects of lixisenatide, with changes in body weight in the range of −2.7 to +0.3 kg and reductions between −1.3 and 0.0 kg, when compared with placebo (). In four of the studies, patients were treated with sulfonylurea or insulin, both of which can cause weight gain. A statistically significant placebo-adjusted decrease in body weight was reported in the GetGoal-L, GetGoal-Duo 1, GetGoal-S, and the GetGoal-F1 studies.Citation46,Citation47,Citation55,Citation56 In three of these studies, lixisenatide was used as add-on to insulin or sulfonylurea, but increase in bodyweight was only observed in the GetGoal-Duo 1 study, which found increases after treatment with lixisenatide and placebo, of 0.3 kg and 1.2 kg, respectively.Citation46
In the GetGoal-X study,Citation49 exenatide demonstrated a more pronounced effect on body weight than did lixisenatide. This study reported the two drugs to cause significant weight reductions from baseline, of 4.0 and 3.0 kg, respectively. Thus, the mean difference was 1.0 kg (95% confidence interval: 0.5–1.6), in favor of exenatide.Citation49 The head-to-head trial comparing lixisenatide and liraglutide mentioned above found a decrease in body weight of 1.6 and 2.4 kg after 4 weeks of treatment with lixisenatide and liraglutide, respectively (P < 0.01).Citation50
Safety and tolerability
Clinical safety of lixisenatide
All of the trials in the GetGoal program have reported results concerning the safety of treatment with lixisenatide (). Additionally, treatment discontinuation rates among patients were stated in most of these studies (). The overall frequency of adverse events (AEs) to treatment with lixisenatide varied from 52% in the GetGoal-Mono study to 89% in the GetGoal-L-Asia study. Likewise, the occurrence of serious adverse events (SAEs) differed substantially between these same two studies, with rates of 0% and 13%, respectively.Citation48,Citation53
Table 3 Safety data from the GetGoal study program
Table 4 Discontinuation data from the GetGoal study program
The most frequently reported AEs to treatment with GLP-1RAs are related to the gastrointestinal system, with nausea and vomiting being by far, the most frequent. Gastrointestinal complaints most often occur within the first month of treatment and tend to diminish over the following weeks.Citation53
Hypoglycemia is a feared AE to antidiabetic treatment and especially with insulin and the sulfonylureas. A limited risk of treatment-induced hypoglycemia in relation to lixisenatide would be expected when considering the glucose-dependent manner of effect. However, the risk of hypoglycemia must especially be taken into account when using lixisenatide in combination with other antidiabetic drugs and in particular, with insulin and sulfonylurea, which will very often be the case in clinical practice.
As expected, some patients in the clinical studies discontinued treatment before completing the planned follow up. In general, most of these discontinuations were associated with treatment-related AEs. The most relevant findings concerning safety and tolerability will be further elucidated in the following sections.
Gastro-intestinal adverse effects
The most frequent AE, nausea, was observed in as many as 20%–40% of patients treated with lixisenatide in the GetGoal program (). In the placebo-treated patients, nausea was much less common, with a range of 4%–11%. Nausea in relation to lixisenatide was most frequently observed in the GetGoal-L-Asia study. An exclusively Asian population with a suggested more advanced disease due to longer duration of T2DM compared with patients in the remaining studies was listed as a possible explanation for the higher observed incidence.Citation48 Additionally, the study population in the GetGoal-L-Asia study had a relatively low BMI (25 kg/m2), which could have led to a relatively higher exposure of lixisenatide and thereby, a higher incidence of nausea.
Vomiting was in general, less frequently observed, with rates of 7%–18% and 0%–4% in patients treated with lixisenatide and placebo, respectively (). Again, the highest incidence was observed in the GetGoal-L-Asia study. It has been suggested that the incidence of gastrointestinal AEs can be reduced using a dose-escalation strategy.Citation57 However, in both the GetGoal-Mono and in the GetGoal-F1 study, a trend towards higher incidence of gastrointestinal AEs following two-step titration compared with one-step titration, was observed ().Citation53,Citation58
In the GetGoal-X study, lixisenatide was found to cause less gastrointestinal AEs compared with exenatide. In this study, the incidence of nausea and vomiting in the lixisenatide-treated group was 25% and 10%, respectively. The corresponding rates for patients treated with exenatide were 35% and 13% ().Citation49
The head-to-head trial comparing lixisenatide and liraglutide as add-on to metformin found similar incidences of nausea (23% vs 22%) and vomiting (10% vs 7%) in the two treatment groups. Diarrhea seemed to be more frequent during treatment, with liraglutide having an incidence of 16% as compared with 3% for lixisenatide.Citation50 In the GetGoal-X study,Citation49 diarrhea was observed in 10% and 13% of patients treated with lixisenatide and exenatide, respectively. In the placebo-controlled trials of the GetGoal study program, diarrhea was observed in 7%–9% of patients treated with lixisenatide and 3%–11% of controls. Interestingly, in the GetGoal-P study,Citation59 a higher occurrence of diarrhea was observed with placebo compared with lixisenatide treatment.
As previously described, the gastrointestinal AEs in relation to treatment with GLP-1 often tend to decrease within the first weeks of ongoing use. The GetGoal-Mono study stated that the gastrointestinal AEs diminished within 7 weeks of ongoing treatment, and the GetGoal-L, GetGoal-Duo 1, and GetGoal-L-Asia studies also described a spontaneous reduction in gastrointestinal AEs over time.Citation46–Citation48,Citation53
Hypoglycemia
All studies in the GetGoal program reported results concerning hypoglycemic events. The applied definition of symptomatic hypoglycemia in these studies was: symptoms of hypoglycemia, with accompanying blood glucose < 3.3 mmol/L or prompt recovery after carbohydrate intake. Furthermore, severe hypoglycemia was defined as hypoglycemic episodes requiring assistance.
As previously described, the glucose-dependent effect of lixisenatide should in theory, confer a low risk of treatment-induced hypoglycemia. The GetGoal-Mono studyCitation53 confirmed this assumption. In this study, lixisenatide monotherapy caused symptomatic hypoglycemia in 0.8% and 2.5% of patients treated with lixisenatide one-step and two-step titration, respectively. A similar incidence of 1.6% was observed in the combined placebo group. No severe hypoglycemic events were reported in the GetGoal-Mono study. Both the frequency and severity of hypoglycemia in clinical trials seemed to be highly dependent on comedication with insulin or the sulfonylureas, as these drugs are known to raise serum insulin levels irrespective of the prevailing plasma glucose level. A limited frequency of hypoglycemia was seen in studies combining lixisenatide with metformin and the glitazones (GetGoal-P, GetGoal-M, and GetGoal-F1). The highest frequency of symptomatic hypoglycemia in lixisenatide-treated patients in these studies was 7.5%, and the reported incidences were in general, comparable with placebo ().Citation51,Citation58,Citation59 Furthermore, no severe hypoglycemic events were reported in any of these studies.
The combination of treatment with lixisenatide and insulin in the GetGoal-L,Citation47 GetGoal-L-Asia,Citation48 and GetGoal-Duo 1Citation46 studies resulted in considerably more hypoglycemic events. Incidences of symptomatic hypoglycemia between 20% and 43% in lixisenatide-treated patients were reported in these studies. The frequency of symptomatic hypoglycemia was similar to that seen with placebo in the GetGoal-L study, whereas the incidence was almost doubled in comparison to that of placebo in the GetGoal-L-Asia and GetGoal-Duo 1 studies (). Symptomatic hypoglycemia was by far the most common in the GetGoal-L-Asia study, which could be explained by the fact that 70% of patients in this study, in addition to insulin, were treated with sulfonylureas. One (0.4%) and four (1.2%) cases of severe hypoglycemia in lixisenatide-treated patients were reported in the GetGoal-Duo 1 and GetGoal-L studies, respectively. No cases were reported in the placebo-treated controls.
Lixisenatide was used as add-on to sulfonylurea in the GetGoal-S study.Citation56 Comparable frequencies of symptomatic hypoglycemia (15% vs 12%) were observed in the lixisenatide and placebo-treated patients. One case (0.2%) of severe hypoglycemia was reported in the group treated with lixisenatide and none in relation to placebo. It has been suggested that sulfonylurea drugs may uncouple the glucose dependency of GLP-1.Citation60 Whether this possible mechanism was responsible for the difference in observed cases of hypoglycemia is unknown. However, the data showed that the risk of hypoglycemia must be considered when using lixisenatide in combination with sulfonylurea and particularly, if additional treatment with insulin is applied.
In the GetGoal-X study,Citation49 significantly fewer patients treated with lixisenatide experienced a symptomatic hypoglycemic event as compared with exenatide. The incidences of hypoglycemia were 2.5% and 7.9% (P < 0.05). No cases of severe hypoglycemia were reported. In the head-to-head study between lixisenatide and liraglutide, no cases of either symptomatic or severe hypoglycemia were reported.Citation50
Other adverse events
No cases of suspected pancreatitis have been observed during treatment with lixisenatide. A total number of four allergic reactions in about 2500 patients treated with lixisenatide have been reported. One patient experienced angioedemaCitation53 and the remaining three had urticarial reactions.Citation48,Citation50,Citation53 Other adverse events (eg, headache and dizziness) were in general, reported only slightly more often after treatment with lixisenatide compared with placebo.
The head-to-head trial comparing lixisenatide and liraglutide found these treatments to cause a change in heart rate, of −3.6 and +5.3 beats/min, respectively. The observed difference between treatments of 8.9 beats/min was significant.Citation50 A different study reported no changes in heart rate following treatment with lixisenatide.Citation43
Antibody formation
Two studies have discussed the clinical importance of anti-lixisenatide antibodies. In the GetGoal-Mono studyCitation53 the development of antibodies was reported in approximately 60% of patients treated with 20 μg lixisenatide once daily. In another study antibodies were found in 43% of subjects treated with 10 μg lixisenatide once daily and in 71% treated with 20 μg twice dailyCitation43 No relevant differences were reported in terms of safety and efficacy between antibody-positive and -negative patients in either of the two studies. None of the studies reported on the incidences of high-titer antibodies, which have been noted to better predict the clinical significance of antibodies to the similar GLP-1RA, exenatide.Citation61
Tolerability and patient satisfaction
All studies in the GetGoal program except the GetGoal-M study provided information about patient discontinuation due to adverse events, which can be used as an expression of tolerability. A discontinuation rate due to AEs above 10% was only observed in patients treated with two-step titration in the GetGoal-F1 study. In the GetGoal-Mono study, AEs due to lixisenatide monotherapy caused discontinuation in less than 5% of patients. In the remaining studies, treatment with lixisenatide as add-on to various other antidiabetic drugs resulted in discontinuation due to AEs in 5%–10% of patients (). A tendency towards less discontinuation due to AEs in the control groups was observed in all of the placebo-controlled studies in the GetGoal program. Several of the studies stated that discontinuation due to AEs was mainly a result of nausea and vomiting.Citation46–Citation48,Citation58,Citation59 Furthermore, higher rates of overall discontinuation (all reasons) were reported following treatment with lixisenatide, as compared with placebo ().
Similar discontinuation rates were seen when comparing lixisenatide to the other available GLP-1RAs, exenatide and liraglutide. In the GetGoal-X study,Citation49 treatment with lixisenatide and exenatide led to discontinuation due to AEs in 9.1% and 9.8% of patients, respectively. The corresponding rates in the trial comparing lixisenatide and liraglutide were 2.6% and 2.8%, respectively.Citation50
GetGoal-X was the only study that directly addressed patient satisfaction in relation to treatment with lixisenatide. This was done using the Patient Assessment of Upper Gastrointestinal Disorders-Quality Of Life (PAGI-QOL) questionnaire that is a tool for assessing quality of life in patients with upper gastrointestinal disorders. Changes in the PAGI-QOL score of less than 0.4 in relation to treatment is described to be without any clinical relevance.Citation62 The change from baseline in PAGI-QOL score did not differ between lixisenatide- and exenatide-treated patients, with absolute changes of −0.09 and −0.06, respectivelyCitation49
A recently published review by RussellCitation63 discussed patient satisfaction in relation to different incretin-based therapies. Despite the need for injections and a higher frequency of gastrointestinal side effects, a greater patient satisfaction was seen in relation to treatment with the GLP-1RAs liraglutide and exenatide in comparison with DPP-4 inhibitors. The author suggested a greater effect with respect to glycemic control and weight loss as the most likely explanation for this finding.
Conclusion, place in therapy
A dose of 20 μg once daily administered before breakfast has been established as the most rational regimen of treatment with lixisenatide (Lyxumia). This regimen is similar to the once daily administration of liraglutide (Victoza) and differs from the twice daily (Byetta) and once weekly (Bydureon) administration of exenatide.
In the GetGoal Phase III study program, lixisenatide has demonstrated significant reduction in HbA1c, FPG, and PPG compared with placebo. The effect on glycemia was present for both monotherapy and in combination with insulin and various oral antidiabetic agents. Furthermore, a trend towards reduced body weight, in the range of 0.5–1.0 kg was observed. However, in several of the studies, the reported reductions in body weight were not statistically significant. Exenatide and liraglutide have been reviewed elsewhere, and these drugs were shown to reduce HbA1c by about 1–2 percentage points and cause a weight loss of ~2 kg.Citation64 A recent meta-analysis concerning the efficacy of treatment with the various DPP-4 inhibitors has reported placebo-controlled reductions in HbA1c and FPG of 0.5%–1.0% and 0.7–1.5 mmol/L, respectivelyCitation65 Furthermore, the DDP-4 inhibitors were found to be weight neutral.Citation65 Thus, the treatment effects of lixisenatide, in terms of HbA1c, FPG, and body weight, seem to be very similar to the efficacy of treatment with DPP-4 inhibitors. However, it has to be noted that no direct comparisons have been carried out.
The potential of lixisenatide, in terms of PPG reduction, has been demonstrated in a direct comparison with liraglutide. The delaying effect on gastric emptying by GLP-1 has been shown to wane during continuous exposure,Citation24 and this could very likely be the explanation for the significantly larger effect of the short-acting lixisenatide (t½ = 2–3 hours) on PPG as compared with the longer acting liraglutide (t½ = 13 hours). The clinical value of targeted treatment of PPG excursions still needs to be determined. As previously described, PPG has been recognized as a contributor to overall glycemic control, in terms of HbA1c, in patients with mild to moderate severity T2DM. In the GetGoal-Duo 1 study, a decrease in HbA1c was observed without a corresponding decrease in FPG, which could indicate an important role of PPG when it comes to achieving overall glycemic control. Furthermore, PPG has been discussed as a potential therapeutic target with respect to achieving reduced cardiovascular morbidity in relation to T2DM.Citation66
Based on the results from the GetGoal-X study and the comparison with liraglutide, it appears that liraglutide and possibly exenatide are superior to lixisenatide in terms of HbA1c reduction.Citation49,Citation50 However, the GetGoal-X study claimed noninferiority of lixisenatide in comparison with exenatide, based on a defined noninferiority margin (95% confidence interval of the difference not exceeding 0.4). Furthermore, the limited duration of the trial with liraglutide should be taken into account when interpreting the result of this study. The two studies demonstrated a superior reduction in body weight after treatment with exenatide and liraglutide as compared with lixisenatide. In addition, liraglutide was found to reduce FPG more than lixisenatide.
Nausea and vomiting were the most frequently observed adverse events in relation to treatment with lixisenatide. Although several studies listed nausea and vomiting as the main reasons for discontinuation of treatment, these events were in general reported to decrease within the first weeks of ongoing use. Hypoglycemic events after treatment with lixisenatide seemed to be highly dependent on comedication with insulin or the sulfonylureas, and the risk of hypoglycemia must be considered when applying these combinations of antidiabetic treatment. Similar rates of discontinuation were observed after treatment with lixisenatide, exenatide, and liraglutide.
Weighing the efficacy against the adverse events and the economic costs generated by a specific treatment is a rational approach when having to decide on a specific treatment, and when comparing across treatments with the same indication. At best, lixisenatide seems to be equivalent to the alternative GLP-1RAs, with respect to HbA1c, FPG, and weight reduction. However, in direct comparisons, lixisenatide demonstrated a tendency towards fewer AEs. Considering the equal method of action, it is likely that the difference in efficacy and AEs is mainly a pharmacokinetic issue.
The combination of a substantial effect on PPG and a labeling of once daily administration is, however, a discerning factor compared with the GLP-1RAs already on the market. The combination of basal insulin, with its lowering effect on FPG, and lixisenatide, curtailing the postprandial glucose excursions, makes sense from a clinical point of view. Not surprisingly, lixisenatide is undergoing clinical development as a combination product with insulin glargine (Lantus®; Sanofi). This treatment combination has been shown to substantially improve HbA1c, without weight gain, in the GetGoal-L, GetGoal-L-Asia, and the GetGoal-Duo 1 studies. At present, unless lixisenatide is priced lower than the already available GLP-1RA alternatives, it appears that the main place in therapy for lixisenatide is in the combination with insulin glargine. The ongoing multicenter ELIXA study (evaluation of cardiovascular outcomes in patients with Type 2 Diabetes after Acute Coronary Syndrome during treatment with AVE0010 [Lixisenatide], NCT01147250) will determine the future potential of lixisenatide in preventing cardiovascular events and mortality, in patients with T2DM and recent acute coronary syndrome.
Acknowledgments
The authors would like to thank JP Kampmann for his critical appraisal of this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
- Wild S Roglic G Green A Sicree R King H Global prevalence of diabetes: estimates for the year 2000 and projections for 2030 Diabetes Care 2004 27 5 1047 1053 15111519
- Monnier L Lapinski H Colette C Contributions of fasting and postprandial plasma glucose increments to the overall diurnal hyperglycemia of type 2 diabetic patients: variations with increasing levels of HbA(1c) Diabetes Care 2003 26 3 881 885 12610053
- Göke B Islet cell function: alpha and beta cells – partners towards normoglycaemia Int J Clin Pract Suppl 2008 159 2 7 18269435
- Meier JJ Nauck MA Is the diminished incretin effect in type 2 diabetes just an epi-phenomenon of impaired beta-cell function? Diabetes 2010 59 5 1117 1125 20427697
- Nathan DM Buse JB Davidson MB American Diabetes Association; European Association for the Study of Diabetes Medical management of hyperglycaemia in type 2 diabetes mellitus: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement from the American Diabetes Association and the European Association for the Study of Diabetes Diabetologia 2009 52 1 17 30 18941734
- Cubbon R Kahn M Kearney MT Secondary prevention of cardiovascular disease in type 2 diabetes and prediabetes: a cardiologist’s perspective Int J Clin Pract 2008 62 2 287 299 18036163
- Gaede P Lund-Andersen H Parving H-H Pedersen O Effect of a multifactorial intervention on mortality in type 2 diabetes N Eng J Med 2008 358 6 580 591
- Inzucchi SE Bergenstal RM Buse JB Management of hyperglycaemia in type 2 diabetes: a patient-centered approach. Position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) Diabetologia 2012 55 6 1577 1596 22526604
- Vilsbøll T Holst JJ Incretins, insulin secretion and Type 2 diabetes mellitus Diabetologia 2004 47 3 357 366 14968296
- Perley MJ Kipnis DM Plasma insulin responses to oral and intravenous glucose: studies in normal and diabetic subjects J Clin Invest 1967 46 12 1954 1962 6074000
- Nauck MA Homberger E Siegel EG Incretin effects of increasing glucose loads in man calculated from venous insulin and C-peptide responses J Clin Endocrinol Metab 1986 63 2 492 498 3522621
- Holst JJ Gromada J Role of incretin hormones in the regulation of insulin secretion in diabetic and nondiabetic humans Am J Physiol Endocrinol Metab 2004 287 2 E199 E206 15271645
- Fehmann HC Göke R Göke B Cell and molecular biology of the incretin hormones glucagon-like peptide-I and glucose-dependent insulin releasing polypeptide Endocr Rev 1995 16 3 390 410 7671853
- Vilsbøll T Krarup T Madsbad S Holst JJ Both GLP-1 and GIP are insulinotropic at basal and postprandial glucose levels and contribute nearly equally to the incretin effect of a meal in healthy subjects Regul Pept 2003 114 2–3 115 121 12832099
- Nauck MA Bartels E Orskov C Ebert R Creutzfeldt W Additive insulinotropic effects of exogenous synthetic human gastric inhibitory polypeptide and glucagon-like peptide-1–(7–36) amide infused at near-physiological insulinotropic hormone and glucose concentrations J Clin Endocrinol Metab 1993 76 4 912 917 8473405
- Holst JJ The physiology of glucagon-like peptide 1 Physiol Rev 2007 87 4 1409 1439 17928588
- Deacon CF Nauck MA Toft-Nielsen M Pridal L Willms B Holst JJ Both subcutaneously and intravenously administered glucagon-like peptide I are rapidly degraded from the NH2-terminus in type II diabetic patients and in healthy subjects Diabetes 1995 44 9 1126 1131 7657039
- Nauck MA Heimesaat MM Behle K Effects of glucagon-like peptide 1 on counterregulatory hormone responses, cognitive functions, and insulin secretion during hyperinsulinemic, stepped hypoglycemic clamp experiments in healthy volunteers J Clin Endocrinol Metab 2002 87 3 1239 1246 11889194
- Egan JM Bulotta A Hui H Perfetti R GLP-1 receptor agonists are growth and differentiation factors for pancreatic islet beta cells Diabetes Metab Res Rev 2003 19 2 115 123 12673779
- Buteau J El-Assaad W Rhodes CJ Rosenberg L Joly E Prentki M Glucagon-like peptide-1 prevents beta cell glucolipotoxicity Diabetologia 2004 47 5 806 815 15095038
- Larsson H Holst JJ Ahrén B Glucagon-like peptide-1 reduces hepatic glucose production indirectly through insulin and glucagon in humans Acta Physiol Scand 1997 160 4 413 422 9338524
- Hare KJ Knop FK Incretin-based therapy and type 2 diabetes Vitam Horm 2010 84 389 413 21094909
- Flint A Raben A Astrup A Holst JJ Glucagon-like peptide 1 promotes satiety and suppresses energy intake in humans J Clin Invest 1998 101 3 515 520 9449682
- Nauck MA Kemmeries G Holst JJ Meier JJ Rapid tachyphylaxis of the glucagon-like peptide 1-induced deceleration of gastric emptying in humans Diabetes 2011 60 5 1561 1565 21430088
- Nikolaidis LA Mankad S Sokos GG Effects of glucagon-like peptide-1 in patients with acute myocardial infarction and left ventricular dysfunction after successful reperfusion Circulation 2004 109 8 962 965 14981009
- Nikolaidis LA Elahi D Hentosz T Recombinant glucagon-like peptide-1 increases myocardial glucose uptake and improves left ventricular performance in conscious dogs with pacing-induced dilated cardiomyopathy Circulation 2004 110 8 955 961 15313949
- Nyström T Gutniak MK Zhang Q Effects of glucagon-like peptide-1 on endothelial function in type 2 diabetes patients with stable coronary artery disease Am J Physiol Endocrinol Metab 2004 287 6 E1209 E1215 15353407
- Lønborg J Vejlstrup N Kelbæk H Exenatide reduces reperfusion injury in patients with ST-segment elevation myocardial infarction Eur Heart J 2012 33 12 1491 1499 21920963
- Meier JJ Gethmann A Götze O Glucagon-like peptide 1 abolishes the postprandial rise in triglyceride concentrations and lowers levels of nonesterified fatty acids in humans Diabetologia 2006 49 3 452 458 16447057
- Yerram P Whaley-Connell A Novel role for the incretins in blood pressure regulation Curr Opin Nephrol Hypertens 2012 21 5 463 468 22871675
- Nyström T Gonon AT Sjöholm A Pernow J Glucagon-like peptide-1 relaxes rat conduit arteries via an endothelium-independent mechanism Regul Pept 2005 125 1–3 173 177 15582729
- Carraro-Lacroix LR Malnic G Girardi AC Regulation of Na+/H+ exchanger NHE3 by glucagon-like peptide 1 receptor agonist exendin-4 in renal proximal tubule cells Am J Physiol Renal Physiol 2009 297 6 F1647 F1655 19776173
- Becker R Kapitza C Stechl J Ruus P Msihid J Restitution of glucose disposition with lixisenatide in subjects with type 2 diabetes [Abstract] Diabetologia 2012 55 Suppl 1 S335 S336
- Distiller L Ruus P Pharmacokinetics and pharmacodynamics of GLP-1 agonist AVE0010 in type 2 diabetes patients [Abstract] Diabetes 2008 57 Suppl 1 520-P
- Meier JJ Nauck MA Kranz D Secretion, degradation, and elimination of glucagon-like peptide 1 and gastric inhibitory polypeptide in patients with chronic renal insufficiency and healthy control subjects Diabetes 2004 53 3 654 662 14988249
- Stechl J Becker R Kapitza C Msihid J Augmentation of 1st-phase insulin release with lixisenatide in non-diabetic subjects [Abstract] Diabetologia 2012 55 Suppl 1 S336
- European Medicines Agency Byetta: EPAR – Product Information London European Medicines Agency 2009 [updated March 25, 2013; cited January 10, 2013]. Available from: http://www.emea.europa.eu/ema/index.jsp?curl=pages/medicines/human/medicines/000698/human_med_000682.jsp&mid=WC0b01ac058001d124#product-info Accessed April 20, 2013
- Liu YH Ruus P Pharmacokinetics and safety of the GLP-1 Agonist AVE0010 in patients with renal impairment [Abstract] Diabetes 2009 58 Suppl 1 557-P
- Liu YH Ruus P Effect of the GLP-1 Agonist AVE0010 on absorption of concomitant oral drugs [Abstract] Diabetes 2009 58 Suppl 1 495-P
- Liu YH Ruus P Steinstraesser A Teichert L Effect of the GLP-1 agonist lixisenatide on the pharmacokinetics of warfarin [Abstract] Diabetes 2010 59 Suppl 1 2128-PO
- Thorkildsen C Neve S Larsen BD Meier E Petersen JS Glucagon-like peptide 1 receptor agonist ZP10A increases insulin mRNA expression and prevents diabetic progression in db/db mice J Pharmacol Exp Ther 2003 307 2 490 496 12975499
- Werner U Haschke G Herling AW Kramer W Pharmacological profile of lixisenatide: A new GLP-1 receptor agonist for the treatment of type 2 diabetes Regul Pept 2010 164 2–3 58 64 20570597
- Ratner RE Rosenstock J Boka G DR16012 Study Investigators Dose-dependent effects of the once-daily GLP-1 receptor agonist lixisenatide in patients with Type 2 diabetes inadequately controlled with metformin: a randomized, double-blind, placebo-controlled trial Diabet Med 2010 27 9 1024 1032 20722676
- Meier JJ GLP-1 receptor agonists for individualized treatment of type 2 diabetes mellitus Nat Rev Endocrinol 2012 8 12 728 742 22945360
- Makris K Spanou L Is there a relationship between mean blood glucose and glycated hemoglobin? J Diabetes Sci Technol 2011 5 6 1572 1583 22226280
- Rosenstock J Forst T Aronson R Once-daily lixisenatide added on to consistently titrated insulin glargine plus oral agents in type 2 diabetes: the getgoal-duo 1 study [Abstract] Diabetologia 2012 55 Suppl 1 S333
- Aronson R Riddle M Home P Efficacy and safety of once-daily lixisenatide in type 2 diabetes insufficiently controlled with basal insulin ± metformin: GetGoal-L study [Abstract] Diabetologia 2012 55 Suppl 1 S8
- Seino Y Min KW Niemoeller E Takami A EFC10887 GETGOAL-L Asia Study Investigators Randomized, double-blind, placebo-controlled trial of the once-daily GLP-1 receptor agonist lixisenatide in Asian patients with type 2 diabetes insufficiently controlled on basal insulin with or without a sulfonylurea (GetGoal-L-Asia) Diabetes Obes Metab 2012 14 10 910 917 22564709
- Rosenstock J Raccah D Korányi L Efficacy and safety of lixisenatide once-daily versus exenatide twice-daily in patients with type 2 diabetes insufficiently controlled on metformin (GetGoal-X) [Abstract] Diabetologia 2011 54 Suppl 1 S317 S318
- Kapitza C Forst T Coester HV Poitiers F Ruus P Hincelin-Méry A Pharmacodynamic characteristics of lixisenatide once daily versus liraglutide once daily in patients with type 2 diabetes insufficiently controlled on metformin Diabetes Obes Metab 2013 Epub 1 31 2013
- Ahrén B Leguizamo Dimas A Miossec P Saubadu S Aronson R Efficacy and safety of lixisenatide once-daily morning or evening injections in type 2 diabetes inadequately controlled on metformin (GetGoal-M) Diabetes Care 3 27 2013
- Raccah D Miossec P Esposito V Niemoeller E Cho M Gerich J Efficacy and safety of lixisenatide in elderly (≥65 years) and very elderly (≥75 years) patients with type 2 diabetes: an analysis from the GetGoal phase 3 program [Poster] 48th EASD Annual Meeting 1–5 October 2012 P815
- Fonseca VA Alvarado-Ruiz R Raccah D Boka G Miossec P Gerich JE EFC6018 GetGoal-Mono Study Investigators Efficacy and safety of the once-daily GLP-1 receptor agonist lixisenatide in monotherapy: a randomized, double-blind, placebo-controlled trial in patients with type 2 diabetes (GetGoal-Mono) Diabetes Care 2012 35 6 1225 1231 22432104
- Lorenz M Pfeiffer C Steinstraesser A Ruus P Becker R Effects of lixisenatide once daily on gastric emptying and its relationship to postprandial glycemia in type 2 diabetes mellitus Diabetes 2012 61 A212 A344 [Abstract 1085-P]
- Bolli G Munteanu M Dotsenko S Niemoeller E Boka G Hanefeld M Efficacy and safety of lixisenatide once-daily versus placebo in patients with type 2 diabetes mellitus insufficiently controlled on metformin (GetGoal-F1) [Abstract] Diabetologia 2011 54 Suppl 1 S316 S317
- Ratner RE Hanefeld M Shamanna P Post-meal pharmacodynamic profile of lixisenatide once daily vs placebo in T2DM insufficiently controlled on SU ± metformin (GetGoal-S) [Abstract D-0743] Proceedings of the World Diabetes Congress 2011 December 4–8, 2011 Dubai, United Arab Emirates
- Horowitz M Rayner CK Jones KL Mechanisms and clinical efficacy of lixisenatide for the management of type 2 diabetes Adv Ther 2013 30 2 81 101 23423907
- Bolli G Munteanu M Dotsenko S Niemoeller E Wardęcki M Hanefeld M Long-term (up to 2 Years) safety of lixisenatide once daily vs placebo in t2dm insufficiently controlled on metformin (GetGoal-F1) [Abstract O-0595] Proceedings of the World Diabetes Congress 2011 December 4–8, 2011 Dubai, United Arab Emirates
- Pinget M Goldenberg R Niemoeller E Muehlen-Bartmer I Aronson R Efficacy and safety of lixisenatide once daily versus placebo in patients with type 2 diabetes insufficiently controlled on pioglitazone (GetGoal-P) [Abstract] Diabetologia 2012 55 Suppl 1 S334
- De Heer J Holst JJ Sulfonylurea compounds uncouple the glucose dependence of the insulinotropic effect of glucagon-like peptide 1 Diabetes 2007 56 2 438 443 17259389
- European Medicines Agency Byetta: EPAR – Scientific Discussion London European Medicines Agency 2006 Available from: http://www.emea.europa.eu/ema/index.jsp?curl=pages/medicines/human/medi-cines/000698/human_med_000682.jsp&mid=WC0b01ac058001d124 Accessed April 20, 2013
- De La Loge C Trudeau E Marquis P Responsiveness and interpretation of a quality of life questionnaire specific to upper gastrointestinal disorders Clin Gastroenterol Hepatol 2004 2 9 778 786 15354278
- Russell S Incretin-based therapies for type 2 diabetes mellitus: a review of direct comparisons of efficacy, safety and patient satisfaction Int J Clin Pharm 2013 35 2 159 172 23263796
- Madsbad S Exenatide and liraglutide: different approaches to develop GLP-1 receptor agonists (incretin mimetics) – preclinical and clinical results Best Pract Res Clin Endocrinol Metab 2009 23 4 463 477 19748064
- Aroda VR Henry RR Han J Efficacy of GLP-1 receptor agonists and DPP-4 inhibitors: meta-analysis and systematic review Clin Ther 2012 34 6 1247 1258 22608780
- Peter R Okoseime OE Rees A Owens DR Postprandial glucose – a potential therapeutic target to reduce cardiovascular mortality Curr Vasc Pharmacol 2009 7 1 68 74 19149642