
Abstract
The effective management of OFF episodes remains an important unmet need for patients with Parkinson’s disease (PD) who develop motor complications with long-term levodopa therapy. Istradefylline is a selective adenosine A2A receptor antagonist for the treatment of patients with PD experiencing OFF episodes while on levodopa/decarboxylase inhibitor. Originally approved in Japan, istradefylline was recently approved in the USA. In this article, we provide a specific review of the four clinical studies that the FDA included in the approval of istradefylline in the USA, and discuss common clinical scenarios, based on our experience, where treatment with istradefylline may benefit patients experiencing motor fluctuations.
Introduction
Despite advances in dopaminergic medications since the introduction of levodopa over 50 years ago, control of OFF episodes remains an important unmet need in the management of patients with Parkinson’s disease (PD).Citation1 After 5 years of levodopa therapy, about half (54%) of patients will experience OFF time,Citation2–4 increasing to nearly 100% at 10 years.Citation4,Citation5 Despite increasing levodopa dose and frequency, OFF time remains in many patients. Indeed, even some patients using continuous jejunal and subcutaneous infusions of levodopa continue to experience significant OFF time.Citation6,Citation7 Current adjunctive therapies, such as the dopamine agonists (pramipexole, ropinirole, and rotigotine), catechol-O-methyltransferase (COMT) inhibitors (entacapone, opicapone, and tolcapone), monoamine oxidase-B (MAO-B) inhibitors (selegiline, rasagiline, and safinamide), and amantadine, reduce OFF time by up to an hour per day but do not fully eliminate OFF episodes.Citation8–11 Furthermore, these adjunctive therapies may be accompanied by dose-limiting adverse events,Citation8,Citation12,Citation13 particularly in the elderly and in patients with advanced disease, including dyskinesia, nausea, somnolence, orthostatic hypotension, hallucinations, and impulse control disorders. As a consequence, the risk–benefit profile of each medication should be chosen according to the patient’s individual motor and non-motor symptoms. Recent research has focused on finding novel non-dopaminergic pathways that might improve OFF time without dose-limiting dopaminergic adverse effects.Citation14,Citation15
In the healthy brain, the direct (stimulatory, “Go”) pathway and the indirect (inhibitory, “Stop”) striatal outflow pathways lead to normal movement. The direct (“Go”) pathway is predominantly D1 receptor mediated, while the indirect (“Stop”) pathway is predominantly D2 receptor mediated. In PD, dopamine depletion in the striatum results in reduced direct pathway “Go” activity and increased indirect pathway “Stop” activity, resulting in bradykinesia. Dopamine replacement via its precursor levodopa acts on both pathways,Citation16 improving bradykinesia by increasing direct pathway “Go” activity and reducing indirect pathway “Stop” activity. This can be described by analogy to an automobile gas and brake: in PD, the reduced direct “Go” pathway as too little gas and the increased indirect “Stop” pathway activity as the emergency brake. Dopamine replacement leads to “pressing on the gas pedal” (ie, increased direct “Go” pathway activity) and also “releases the emergency brake” (ie, decreased indirect pathway activity).
Other neurochemicals also play a role in modulating these striatal outflow pathways, including adenosine.Citation17,Citation18 Adenosine A2A receptors are selectively expressed on medium spiny neurons that give rise to the indirect “Stop” pathway, but not on those of the direct pathway.Citation19–22 Concomitant with progressive nigrostriatal degeneration is an upregulation of A2A receptors on these medium spiny neurons, increasing during the disease course.Citation23 Importantly, A2A receptors exhibit constitutive activity, and thus the upregulation of A2A receptors in PD further increases indirect “Stop” pathway activity. By the automobile analogy, this leads to excessive braking (ie, increased indirect “Stop” pathway activity), increasing bradykinesia despite dopaminergic pathways “pressing on the gas pedal.”
Istradefylline is a selective adenosine A2A antagonist that has high affinity and specificity for striatal adenosine A2A receptors.Citation24 Since striatal adenosine A2A receptors are upregulated in PD and have intrinsic activity, antagonism of these receptors by istradefylline reduces the indirect “Stop” striatal output pathway overactivity (ie, “releases the emergency brake”) to improve bradykinesia.Citation23 The efficacy and safety of istradefylline in reducing OFF time when given as an adjunct to levodopa were evaluated in eight double-blind, placebo-controlled trials,Citation25–32 and this extensive istradefylline clinical development program has recently been reviewed in detail.Citation33–35 While istradefylline has been approved for use in patients with PD in Japan since 2013,Citation36 the regulatory history for istradefylline in the USA and in Europe is complex and has been well described elsewhere.Citation33,Citation35 In brief, while the US Food and Drug Administration (FDA) found that the balance of evidence supports the use of istradefylline as adjunctive treatment to carbidopa/levodopa in adult patients with PD experiencing OFF episodes, the European Medicines Agency (EMA) has not given its approval, primarily because of negative findings in the European setting.Citation37 US market authorization (2019) was based on four studies,Citation25,Citation27,Citation30,Citation31 which the FDA considered sufficientCitation38 to demonstrate that istradefylline reduces OFF time, increases ON time without troublesome dyskinesia, and is generally well tolerated relative to placebo.Citation34,Citation39 The FDA wrote that it considered that “it is not uncommon to encounter negative studies in clinical development programs, and that their presence alone does not preclude a conclusion that substantial evidence of effectiveness has been demonstrated”.Citation38
Although the clinical experience with the routine use of istradefylline in Japan has been well described,Citation36 discussion of its clinical utility in the USA since approval has not. In this article, we first provide a specific review of the four clinical studiesCitation25,Citation27,Citation30,Citation31 that led to FDA approval in the USA, as only these four studies are included in the Prescribing Information for istradefylline in the USA and the evidence from these four studies is important to clinicians as it forms the primary evidence for using istradefylline in patients with motor fluctuations in the US population. We then discuss common clinical scenarios where non-dopaminergic treatment with istradefylline may be incorporated in routine clinical practice to treat motor fluctuations, based on our collective experience at two specialized PD centers in the USA. As the first non-dopaminergic therapy approved for the treatment of OFF episodes in the USA, it is of interest to describe the clinical use of istradefylline since FDA approval.
Review of Istradefylline Clinical Studies Leading to FDA Approval in the USA
The US FDA granted regulatory approval based on rigorous examination of all eight trials, with results from four of the trials included in the US Prescribing Information (6002-US-005, 6002-US-013, 6002-0608, and 6002-009).Citation38 These four 12-week studies all enrolled patients with moderate to advanced PD (Hoehn and Yahr stages 2–4 during OFF) currently taking levodopa/dopa decarboxylase inhibitor therapy who had motor fluctuations with ≥2–3 hours of daily OFF time. Levodopa and other adjunctive treatment regimens were stable for ≥4 weeks before randomization into double-blind treatment.Citation5,Citation30,Citation31 Patients were randomized to the addition of placebo or istradefylline 20 or 40 mg/day. The primary efficacy measure was reduction in daily OFF time from baseline as assessed by patient home diaries (in hours or as a percentage of daily awake time); ON time without troublesome dyskinesia was assessed as a secondary outcome.
Trial 1 (study 6002-US-005 study) was a phase IIb clinical trial conducted in 195 patients in North America (USA and Canada). The study evaluated the efficacy and safety of 40 mg/day of istradefylline versus placebo (2:1 ratio) in PD patients who were receiving levodopa therapy and experiencing ≥2 hours of OFF time per day. In this study, most patients were already receiving adjunctive treatment: 86% were treated with a dopaminergic agonist and 41.0% were receiving entacapone.Citation25 Patients treated with adjunctive istradefylline showed a significant reduction of −1.8 hours [95% CI: −1.28, −0.08] in OFF time compared with a reduction of −0.6 hours [−2.26, −1.26] with placebo (p=0.005).Citation25 The reductions in the total hours of daily awake time spent in the OFF state correlated with the increases in the total hours of daily awake time spent in the ON state without troublesome dyskinesia.Citation25 Treatment-emergent adverse effects (TEAEs) with istradefylline were generally mild. Of the most frequently reported drug-related TEAEs, dyskinesia occurred more often for patients treated with istradefylline (30.2%) than for patients who received placebo (15.2%), and accidents involving falls were more frequent for patients in the placebo group (9.1%) than for those in the istradefylline group (3.1%).Citation25
Trial 2 (study 6002-US-013) was a phase III clinical trial that enrolled levodopa-treated patients experiencing ≥3 hours of daily OFF time. In this North American study, 231 patients were randomized 1:1 to placebo or istradefylline 20 mg/day. Once again, ≥90% patients were receiving adjunctive antiparkinsonian medication. Compared to baseline, patients treated with istradefylline experienced a mean±SD reduction in daily OFF time of 1.6±3.0 hours compared with 0.9±2.6 hours in the placebo group (placebo-adjusted treatment effect of 0.7 [−1.4, −0.1] hours, p=0.03). Neither ON time with troublesome dyskinesia nor ON time without troublesome dyskinesia was increased significantly between placebo and istradefylline. Dyskinesia (22.6% vs 12.2%), lightheadedness (7.8% vs 3.5%), tremor (5.2% vs 2.6%), constipation (5.2% vs 0.9%), and weight decrease (6.1% vs 2.6%) were reported more often with istradefylline than with placebo.
Trial 3 (study 6002-0608) was conducted in Japan. This was a phase IIb, randomized clinical trial evaluating the efficacy and safety of istradefylline at doses of 20 and 40 mg/day versus placebo in 363 patients with PD and experiencing ≥2 hours of OFF time with their current levodopa-based therapy plus any adjunctive medications. As in the prior studies, most patients (89–96% per group) were already receiving adjunct therapy to levodopa. Placebo-adjusted reductions in OFF time were 0.65 hours for the istradefylline 20 mg/day dose (p=0.013) and 0.92 hours (p<0.001) for the 40 mg/day dose.Citation30 The most commonly reported drug-related TEAE was dyskinesia (placebo, 2.5%; istradefylline 20 mg/day, 8.5%; istradefylline 40 mg/day, 6.4%).Citation30
The fourth trial was conducted in Japan (study 6002-009) and evaluated the efficacy and safety of both the 20 and 40 mg/day doses of istradefylline compared to placebo in patients receiving levodopa, with 83.7–91.1% (per group) of patients receiving other adjunct medications.Citation31 In this study, similar reductions in OFF time were observed with the 20 and 40 mg/day istradefylline doses. At 12 weeks, treatment with istradefylline reduced OFF time by 0.76 hours for the 20 mg/day (p=0.003) and 0.74 hours for the 40 mg/day regimen (p=0.003) versus placebo.Citation31 Once again, the most common TEAE was dyskinesia (placebo, 4.0%; istradefylline 20 mg/day, 13.0%; istradefylline 40 mg/day, 12.1%).
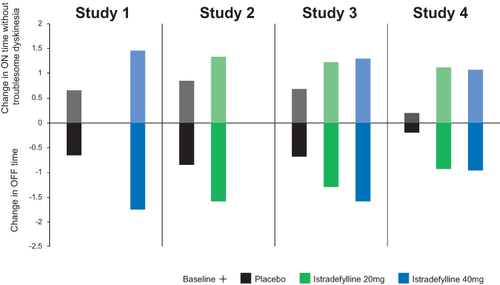
shows the change from baseline over 12 weeks in each of the studies (OFF and ON without troublesome dyskinesia, descriptive data only) as reported in patient diaries (see Supplementary Table e1 for full data). While the FDA considered the results of each study separately for the regulatory approval, a pooled analysis of the same four trials provided further insights into the data supporting the US label for istradefylline.Citation34 When analyzed together, the placebo-adjusted reduction in OFF time was –0.75 [–1.10, –0.40] hours for the istradefylline 20 mg/day dose and –0.82 [–1.17, –0.47] hours for 40 mg/day dose (). Pooled analysis of patient-level data allowed analysis of “good” ON time (defined as ON time without troublesome dyskinesia) at week 12, which was not reported in the original publications of the individual trials. This analysis showed that treatment with istradefylline increased good ON time by 0.68 [0.31, 1.06] hours with the 20 mg/day dose and by 0.69 [0.32, 1.07] hours with the 40 mg/day dose adjusted for placebo. Thus, the placebo-adjusted effect of istradefylline on the increase from baseline in ON time without troublesome dyskinesia was comparable to the decrease in daily OFF time.
Table 1 Treatment-Emergent Adverse Events (>5% and of Special Interest) in the Pooled Analysis of Four Clinical Trials of Istradefylline Versus Placebo
Figure 1 Reduction in OFF time and increases in good ON time (ON without troublesome dyskinesia) from the four randomized controlled studies (istradefylline versus placebo) that led to FDA approval. Study 1, 6002-US-005;Citation25 Study 2, 6002-US-013; Study 3, 6002-0608;Citation30 Study 4, 6002-009.Citation31
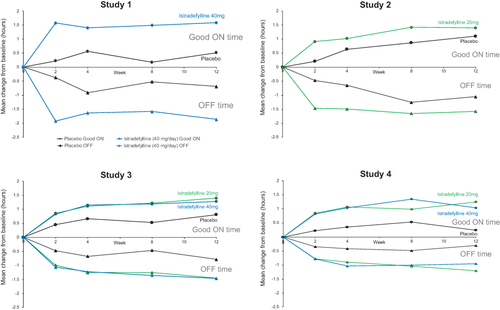
Figure 2 Summary of efficacy outcomes from the four randomized controlled studies (istradefylline versus placebo) that led to FDA approval. Study 1, 6002-US-005;Citation25 Study 2, 6002-US-013;40 Study 3, 6002-0608;Citation30 Study 4, 6002-009.Citation31
Across the four studies, istradefylline demonstrated discontinuation rates similar to placebo. The most common reasons for discontinuation were adverse events (20 mg/day, 4–6% and 40 mg/day, 4.8–7.7% vs placebo, 1.7–7.6%) and withdrawal of consent (20 mg/day, 1.2–4.9% and 40 mg/day, 2.4–3.2% vs placebo, 1.3–5.9%).Citation34 The most frequent TEAEs were dyskinesia (20 mg/day, 14.6% and 40 mg/day, 16.7% vs placebo, 7.5%), nausea (4.2% and 6.3% vs 4.7%), and dizziness (3.1% and 5.6% vs 3.8%) ().Citation34 The mean onset of dyskinesia was around 16 days after starting istradefylline (ie, around the time istradefylline reaches steady state)Citation40 and did not appear to be a common cause for study discontinuation.Citation35 The incidence of other side effects (eg, somnolence, orthostatic hypotension, nausea, hallucinations, confusion, and impulse control disorders) was similar for patients receiving istradefylline and those receiving placebo. Thus, when taken together, the efficacy, tolerability, and safety demonstrated in these trials support that istradefylline’s risk–benefit profile is favorable in doses of 20 and 40 mg/day and is a useful adjunct to levodopa therapy in PD patients experiencing OFF episodes.
Clinical Scenarios
Istradefylline is currently approved in the USA for adjunctive treatment to carbidopa/levodopa in adult patients with PD experiencing OFF episodes.Citation40 The recommended dosage is 20 mg orally once daily, which may be increased to a maximum of 40 mg once daily dependent on patient response. Istradefylline can be considered for any patient on carbidopa/levodopa who experiences OFF episodes, but in our experience, istradefylline may have particular clinical utility for certain common clinical scenarios. The following hypothetical case descriptions have been developed to represent common clinical scenarios based on the authors’ experience.
Clinical Scenario 1: Early Emergence of OFF Episodes
Typical case description: 63-year-old woman with PD for 3 years and recent emergence of OFF episodes. Carbidopa/levodopa 25/100 three times daily was begun 2 years ago, with robust improvement in her symptoms. At her current visit, she reports that symptoms return before her next dose of carbidopa/levodopa. During the clinic visit, she is observed in an OFF episode. Examination reveals right-hand rest tremor, right more than left bradykinesia and rigidity, and slow gait.
In this patient scenario, end-dose wearing-off has emerged after 3 years of levodopa therapy. Multiple options to treat end-dose OFF episodes can be considered, including adjusting levodopa dosing or frequency, adding adjunctive dopaminergic therapy, or adding non-dopaminergic medication. The advantages and disadvantages for each of these need to be considered. Simply increasing levodopa dose may led to peak-dose side effects, including somnolence and dyskinesia, and daily doses >400–600 mg are associated with increased risks of motor complications.Citation41 Likewise, while inexpensive, dose-fractionation strategies can be difficult for patients to manage the ever-shortening intervals between doses, leading to poor complianceCitation42 and suboptimal efficacy.Citation43 Fractionating the dose into more frequent small doses can also lead to unpredictable effects, with the patient’s response becoming more fragile with intermittent symptom re-emergence due to suboptimal levodopa exposure.Citation43,Citation44 Adding adjunctive dopaminergic medication may be limited by the emergence of dopaminergic adverse effects. Rescue or on-demand therapies can be used to treat an OFF episode only after it occurs.
Non-dopaminergic treatment with istradefylline is another option to manage early OFF episodes. In a pooled analysis of 12-week, double-blind studies, patients receiving istradefylline (20–40 mg/day) as their first-line adjunct to levodopa (n=41) showed an adjusted mean [95% CI] reduction in OFF time of −1.53 [−2.59, −0.46] hours versus baseline compared to an increase of 0.30 [−0.93, 1.53] with placebo (n=34).Citation45 The adjusted mean difference between istradefylline and placebo was −1.82 [−3.45, −0.20] hours (p=0.029), which is larger than the magnitude of effect reported for the entire study population,Citation34 and supports the suggestion that istradefylline may be more effective when given earlier in the disease course.Citation35
Clinical Scenario 2: Dopaminergic Therapy Efficacy is Limited by Tolerability
Typical case description: 55-year-old woman diagnosed with PD 6 years ago. She was initially treated with rasagiline, with later addition of pramipexole to good effect. Later increasing the dosage of pramipexole led to pedal edema and daytime somnolence and was tapered back down. Four years ago, extended-release (ER) carbidopa/levodopa was added three times daily, with robust improvement in motor symptoms. Two years ago, ER carbidopa/levodopa was increased to four times daily for OFF episodes between doses, and 1 year ago a fifth dose was added at bedtime. During her routine clinic visit, she describes OFF symptoms that occur between doses.
This patient has had a good response to dopaminergic polypharmacy. However, OFF episodes have re-emerged. Options to manage OFF episodes in this patient include further increasing levodopa frequency or dose, adding another adjunctive dopaminergic therapy, or adding a non-dopaminergic medication. For this patient, past attempts to increase the dopamine agonist dose have led to intolerable side effects. Another option could be to add a COMT inhibitor; the most common adverse event with COMT inhibitors is new onset of dyskinesia, which occurs as a result of increased levodopa bioavailability and has to be managed with levodopa dose reductions.Citation46 In the istradefylline trials, a majority of patients were already receiving other adjunctive therapy and had improvement in OFF time when istradefylline was added. In their pooled analysis of two randomized controlled trials, Hattori et alCitation47 showed that the new onset of dyskinesia (ie, in patients without dyskinesia at baseline, n=356) initiated on istradefylline (20 and 40 mg) was similar to placebo (4–6% with istradefylline vs 3% with placebo), highlighting the relevance of using a non-dopaminergic approach in the polypharmacy mix.
Clinical Scenario 3: OFF Episodes Associated with OFF Symptoms During ON (Suboptimal ON)
Typical case description: 71-year-old man diagnosed with PD 10 years ago. He was started on carbidopa/levodopa with good improvement in symptoms. He is currently taking carbidopa/levodopa 25/100 1.5 tablets every 3 hours with adjunctive COMT and MAO-B enzyme inhibitors (opicapone 50 mg and rasagiline 1 mg, respectively). However, he continues to have OFF episodes and also reports that he feels slow even during ON periods.
Despite increasing dose and frequency of levodopa and combining with peripheral COMT inhibitors to improve the pharmacokinetics and central selective MAO-B metabolism inhibition, some patients continue to have OFF episodes and bradykinesia during ON. It is thought that when dopaminergic strategies fail to resolve OFF symptoms (to use the analogy, when “pressing on the gas” is not enough), then using the adenosine antagonist istradefylline (to “release the brake”) offers a pharmacologically distinct mechanism of action to improve OFF symptoms such as bradykinesia.
Of relevance, despite being on a comprehensive background of therapy, treatment with istradefylline has been shown not only to reduce OFF time, as discussed in the Introduction, but also to improve the quality of ON time, as assessed by the Movement Disorder Society Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) Part III (motor) scale. In the pooled analysis of the four studies included in the US label, week 12 UPDRS Part III (ON) scores demonstrated a significant improvement at both 20 mg/day (–1.36 points [–2.34, –0.38]; p=0.006) and 40 mg/day (–1.82 points [–2.80, –0.84]; p<0.001) istradefylline relative to placebo.Citation34 Moreover, in patients who are on two or more other adjunct therapies, the favorable safety and tolerability of istradefylline makes it a good option for adding another layer of oral therapy before considering more advanced therapeutic approaches.
Clinical Scenario 4: OFF Management Limited by Prior or Current Dyskinesia
Typical case description: 68-year-old woman with PD for 7 years, who developed OFF episodes after 4 years. She initially responded to the addition of MAO-B inhibitor, but OFF time re-emerged 1 year later. Increasing the levodopa dose led to peak dose dyskinesia and lowering the levodopa dose increased OFF time.
As PD progresses, the therapeutic window for reducing motor fluctuations without increasing dyskinesia narrows. This can lead to a dopaminergic “trade-off”, where the decision is between accepting a decrease in OFF time and accepting increased dyskinesia. Adenosine A2A antagonists act through a mechanism beyond the damaged dopaminergic system that avoids an interaction with the direct output pathway, which is implicated in dyskinesia.Citation35 Preclinical studies in MPTP primate models of PD indicate that A2A antagonists do not themselves induce dyskinesia, and that the chronic coadministration of an A2A antagonist with levodopa does not worsen the severity of existing dyskinesia while improving motor function.Citation48–51 Clinical observations support this notion, where the likelihood of developing new-onset dyskinesia is similar to placebo in patients without pre-existing dyskinesia,Citation47 and treatment with istradefylline increases ON time without troublesome dyskinesia overall irrespective of the presence of baseline dyskinesia.Citation25,Citation31,Citation52 While one study has shown a small but statistically significant increase in ON time with troublesome dyskinesia (15 minutes) with istradefylline 40 mg/day,Citation30 changes in this measure were not significant in the other studies. Of note, while the incidence of dyskinesia was higher with istradefylline than placebo (15–17% vs 8%) in the pooled clinical trials,Citation25,Citation27,Citation30,Citation31 just 1% of patients discontinued istradefylline treatment because of dyskinesia.Citation40
Clinical Scenario 5: Daytime Somnolence Limiting Dopaminergic Therapies for OFF Episodes
Typical case description: 75-year-old man with PD diagnosed 4 years ago. Treatment with carbidopa/levodopa 25/100 three times daily resulted in marked improvement in his symptoms. Two years ago, pramipexole was added owing to the emergence of predictable OFF episodes, but was stopped because of increased daytime somnolence. One year ago, sleep apnea was diagnosed.
Sleep disturbances and excessive daytime sleepiness are very common in PD, worsen with the progression of the disease, and require a range of different therapeutic approaches. Daytime somnolence exerts a negative impact on quality of life in addition to increasing the risk of falls.Citation53 Dopamine agonists are well known to significantly increase the risk of sudden uncontrollable somnolence in a dose-related manner,Citation54,Citation55 and inappropriate daytime sleep episodes have also been reported with COMT inhibitors as a result of increased levodopa exposure.Citation56–58
While the incidence of somnolence was 9–22% with the dopamine agonist pramipexoleCitation59 and 20–40% with ropinirole, it was not an adverse event with a reported incidence rate ≥5%, or more frequently occurring with istradefylline than with placebo.Citation40 In a pooled analysis of the four istradefylline trials included in the US label, rates of somnolence with the istradefylline 20 mg/day and 40 mg/day doses were similar to placebo (4.2% and 2.1% vs 3.1%, respectively).Citation34 Two patients treated with istradefylline (n=1 per dose group) experienced a sleep attack/sudden-onset sleep during the studies. Moreover, unlike available dopamine agonists and COMT inhibitors, the FDA label does not include any warning for istradefylline regarding somnolence.Citation40 Indeed, considering its mechanism of action, it has been suggested that treatment with istradefylline should be useful in reducing somnolence in PD.Citation60 Adenosine is a potent endogenous somnogen that modulates the sleep–wake cycle through a variety of mechanisms in a range of brain areas,Citation61 and it is well accepted that adenosine A2A receptors play a dominant role in the induction and gating of sleep.Citation62 While much more work is needed to understand the benefits of adenosine A2A receptor inhibition on sleep, two small clinical studies have shown benefits in reducing excessive daytime sleepiness (as assessed by the Epworth Sleepiness Scale) without affecting nocturnal sleep (as assessed by the PD Sleep Scale).Citation63,Citation64
Clinical Scenario 6: OFF Symptoms of Tremor and Fatigue
Typical case description: 72-year-old woman diagnosed with PD 5 years ago. She was started on carbidopa/levodopa with good improvement in symptoms over 4 years. However, she now complains of the re-emergence of tremor (during ON periods) and says she is very fatigued at certain times of day.
Tremor-dominant PD refers to patients who present initially with tremor with relatively mild bradykinesia and rigidity and who often progress slowly over many years with tremor remaining the most prominent clinical symptom.Citation65 Unfortunately, tremor may be less responsive to levodopa treatment than the other cardinal symptoms of the disease, with some patients requiring higher levodopa doses,Citation14 and thus a non-dopaminergic approach may be sought. In a post-hoc analysis, Pagan et al used tremor items from the UPDRS to evaluate the efficacy of istradefylline in patients who showed a profile consistent with tremor-dominant PD.Citation66 In this important subgroup of patients, the analysis confirmed significant differences in UPDRS tremor scores (sum of UPDRS items assessing kinetic and postural tremor in the right and left hands and resting tremor of the face/lips or chin/arms/legs) versus placebo for both istradefylline doses tested. Placebo-adjusted mean differences in UPDRS tremor scores were −2.60 [95% CI −4.57, −0.62] for the 20 mg/day dose and −1.83 [−3.55, −0.11] for the 40 mg/day dose, indicating a good response to istradefylline for this often difficult-to-treat symptom in patients already on dopamine-targeting therapies.Citation66
While previously overlooked, fatigue is now accepted as one of the most common PD symptoms and is often considered by patients with PD to be one of the most disabling symptoms affecting daily activities and quality of life.Citation67,Citation68 Studies have reported no effect of dopamine agonists on fatigueCitation69 and mild to moderate effects for the MAO-B inhibitor rasagiline.Citation70,Citation71 In a small study, treatment with istradefylline resulted in a significant improvement in fatigue over 8 weeks; fatigue severity scores improved from 62.8±7.1 at baseline to 52.3±9.3 (p=0.049).Citation72 Similar positive benefits have been reported in a small case series, where patients showed a reduction on the Parkinson Fatigue Scale.Citation73 However, a subanalysis of another 52-week open-label study found that the benefits of istradefylline on fatigue (MDS-UPDRS Part 1, item 13) did not reach statistical significance.Citation74
Clinical Scenario 7: Elderly PD with OFF Episodes Concerned with the Neuropsychiatric Side Effects of Other Adjunctive Medication
Typical case description: 80-year-old man with PD diagnosed 6 years ago. Has responded well to carbidopa/levodopa treatment, including Stalevo®, over the years, but now his wearing-off is not well controlled by adjusting the levodopa regimen. He has suffered depression in the past and his family are concerned about his risk of developing neuropsychiatric complications.
Because of the higher risks of cognitive and neuropsychiatric complications, clinicians tend to avoid using dopamine agonists in older patientsCitation55,Citation75 and there often comes a point when dopaminergic adjunct therapies to levodopa are no longer sufficient for symptomatic control. Here, the safety and tolerability profile of istradefylline again differentiates it from the dopaminergic therapies as its benefits in reducing OFF time were seen with little to no increase in the cognitive and neuropsychiatric adverse events typically associated with dopaminergic antiparkinsonian therapies. For example, unlike the dopamine agonists,Citation59,Citation76,Citation77 istradefylline was not associated with increased rates of confusion, dream abnormalities, delusions, or anxiety versus placebo.Citation40 Of relevance, however, is that the istradefylline label notes that the incidence of hallucinations was 2% for the 20 mg dose, 6% for the 40 mg dose, and 3% for placebo.Citation40 Such rates are similar to those reported in the Prescribing Information for Stalevo (4%)Citation58 and opicapone (3%)Citation57, and lower than the 17% reported for pramipexoleCitation59 and 10% for ropinirole in advanced disease.Citation76
Clinical Scenario 8: PD with Orthostatic Hypotension Complicating Adjunctive Medication
Typical case description: 85-year-old man diagnosed with PD 7 years ago. He was started on carbidopa/levodopa with improvement in his symptoms. Over the years, the dosing frequency of carbidopa/levodopa was increased owing to OFF periods. He presents to the clinic with complaints of OFF periods and occasional light-headedness. He is currently receiving carbidopa/levodopa every 3 hours and carbidopa/levodopa-ER at bedtime. His sitting blood pressure is 128/78 mmHg and after standing for 3 min is 110/70 mmHg.
Orthostatic hypotension (OH) is a common non-motor symptom of PD and has been associated with unexplained falls, syncope, light-headedness, cognitive impairment, dyspnea, fatigue, blurred vision, and shoulder, neck, or low-back pain upon standing. Symptomatic OH occurs in approximately 20–30% of PD patients and increases with PD duration, disease severity, age, and levodopa dose.Citation78–80 Dopamine agonists can markedly reduce blood pressure in up to a third of patientsCitation81 and changes can occur as early as the first dose.Citation80–83 Although the levodopa dose can be fractionated if orthostatic symptoms occur at peak dose, this is often associated with suboptimal symptom control and exacerbation of OFF episodes.Citation80 In such cases, istradefylline offers a non-dopaminergic alternative with little or no increase in the incidence of OH. Across the four clinical studies considered by the FDA, rates of OH reported as an adverse event (istradefylline 20 mg/day and 40 mg/day vs placebo) were 6.7% and 6.9% versus 5.4%.Citation34 In addition, there was no evidence of orthostasis or hypotension by analysis of vital signs.Citation38
Discussion
In PD, non-dopaminergic approaches can be useful in the clinical management of patients with OFF episodes. Istradefylline is the only adenosine A2A antagonist to reach clinical practice, and while it has a complex regulatory history, the evidence base for istradefylline in the four clinical trials in the US Prescribing Information, and in pooled analyses of all eight trials, reflects its overall efficacy, safety, and tolerability.Citation8,Citation38
Since istradefylline is the first adenosine antagonist to reach market approval, continued experience with this drug in routine clinical practice is important to better understand its role in treating motor fluctuations. We hope the described clinical scenarios are helpful to begin to define the clinical utility of istradefylline in the USA. Observational studies in Japanese patients with motor fluctuations and other common PD symptoms indicate that istradefylline may be useful in patients with postural abnormalities and gait disorders, as well as those experiencing non-motor symptoms of urinary disturbances and mood disorders ().
Table 2 Post-Marketing Clinical Research to Evaluate Parkinson’s Disease Symptoms in Japan
Conclusions
We have presented herein a US-centric view of istradefylline in the management of OFF episodes, with specific reference to its approved US label and to some common clinical scenarios in which we have found it to be particularly useful in our US clinical experience. Istradefylline is an important additional option in the management of OFF episodes, and provides a reduction in OFF time and an increase in good ON time (ON without troublesome dyskinesia) in the range of other drugs approved for a similar indication in the USA, but with a safety and tolerability profile that reflects its non-dopaminergic mechanism of action. The long-term benefit–risk profile of any agent is best explored in clinical practice, where its overall clinical effectiveness can be evaluated in a broader population of patients over longer periods of time than in a randomized clinical trial. Further clinical experience will continue to define the therapeutic role of istradefylline in motor fluctuations.
Disclosure
Stuart H. Isaacson reports honoraria for CME, consultant, research grants, and/or promotional speaker on behalf of AbbVie, Acadia, Acorda, Adamas, Addex, Affiris, Alexza, Allergan, Amarantus, Amneal, Aptinyx, Axial, Axovant, Benevolent, Biogen, Biovie, Britannia, Cadent, Cala, Cerecor, Cerevel, Cipla, Eli Lilly, Enterin, GE Healthcare, Global Kinetics, Impax, Impel, Intec Pharma, Ipsen, Jazz, Kyowa Kirin, Lundbeck, Merz, Michael J. Fox Foundation, Mitsubishi Tanabe, Neuralys, Neurocrine, Neuroderm, Novartis, Parkinson Study Group, Pharma2B, Praxis, Prilenia, Promentis, Revance, Roche, Sage, Sanofi, Scion, Stoparkinson, Sunovion, Sun Pharma, Supernus, Teva, Theravance, Transposon, and UCB. Sagari Betté has nothing to report. Dr. Pahwa serves as a consultant for Abbott, AbbVie, ACADIA, Acorda, Adamas, Amneal, CalaHealth, DisperSol technologies, Global Kinetics, Impel, Jazz, Neuropharma, Kyowa, Lundbeck, Mitsubishi, Neurocrine, Orbis Bioscience, PhotoPharmics, Prilenia, Sage, Scineuro, Sunovion, and Supernus. He receives research support from Abbott, AbbVie, Addex, Biogen, Biohaven, Boston Scientific, EIP, Global Kinetics, Impax, Intec, Lilly, Neuroderm, Neuraly, Parkinson’s Foundation, Pharma 2B, Prelinia, Roche, Sage, SIS, Sun Pharma, Sunovion, Theranexus, Theravance, and Voyager. The authors report no other conflicts of interest in this work.
Acknowledgments
We thank Anita Chadha-Patel of ACP Clinical Communications Ltd (funded by Kyowa Kirin) for medical writing support (literature searching, referencing, and editing) in the development of this article.
References
- LeWitt PA, Chaudhuri KR. Unmet needs in Parkinson disease: motor and non-motor. Parkinsonism Relat Disord. 2020;80(Suppl 1):S7–S12. doi:10.1016/j.parkreldis.2020.09.024
- Bjornestad A, Forsaa EB, Pedersen KF, Tysnes OB, Larsen JP, Alves G. Risk and course of motor complications in a population-based incident Parkinson’s disease cohort. Parkinsonism Relat Disord. 2016;22:48–53. doi:10.1016/j.parkreldis.2015.11.007
- Scott NW, Macleod AD, Counsell CE. Motor complications in an incident Parkinson’s disease cohort. Eur J Neurol. 2016;23(2):304–312. doi:10.1111/ene.12751
- Kim H-J, Mason S, Foltynie T, Winder-Rhodes S, Barker RA, Williams-Gray CH. Motor complications in Parkinson’s disease: 13-year follow-up of the CamPaIGN cohort. Mov Disorders. 2020;35(1):185–190. doi:10.1002/mds.27882
- Mizuno Y, Shimoda S, Origasa H. Long-term treatment of Parkinson’s disease with levodopa and other adjunctive drugs. J Neural Transm. 2018;125(1):35–43. doi:10.1007/s00702-016-1671-x
- Poewe W, Stocchi F, Arkadir D, et al. Subcutaneous levodopa infusion for Parkinson’s disease: one-year data from the open-label BeyoND study. Mov Disord. 2021;36(11):2687–2692. doi:10.1002/mds.28758
- Antonini A, Isaias IU, Canesi M, et al. Duodenal levodopa infusion for advanced Parkinson’s disease: 12-month treatment outcome. Mov Disord. 2007;22(8):1145–1149. doi:10.1002/mds.21500
- Stowe R, Ives N, Clarke CE, et al. Meta-analysis of the comparative efficacy and safety of adjuvant treatment to levodopa in later Parkinson’s disease. Mov Disord. 2011;26(4):587–598. doi:10.1002/mds.23517
- Ferreira JJ, Lees A, Rocha JF, Poewe W, Rascol O, Soares-da-Silva P. Long-term efficacy of opicapone in fluctuating Parkinson’s disease patients: a pooled analysis of data from two phase 3 clinical trials and their open-label extensions. Eur J Neurol. 2019;26(7):953–960. doi:10.1111/ene.13914
- Giossi R, Carrara F, Mazzari M, et al. Overall efficacy and safety of safinamide in Parkinson’s disease: a systematic review and a meta-analysis. Clin Drug Invest. 2021;41(4):321–339. doi:10.1007/s40261-021-01011-y
- Hauser RA, Lytle J, Formella AE, Tanner CM. Amantadine delayed release/extended release capsules significantly reduce OFF time in Parkinson’s disease. NPJ Parkinsons Dis. 2022;8(1):29. doi:10.1038/s41531-022-00291-1
- Chou KL. Adverse events from the treatment of Parkinson’s disease. Neurol Clin. 2008;26(3Suppl):S65–83,vi. doi:10.1016/j.ncl.2008.05.003
- Olanow CW, Stern MB, Sethi K. The scientific and clinical basis for the treatment of Parkinson disease (2009). Neurology. 2009;72(21 Suppl 4):S1–136. doi:10.1212/WNL.0b013e3181a1d44c
- Gonzalez-Latapi P, Bhowmick SS, Saranza G, Fox SH. Non-dopaminergic treatments for motor control in Parkinson’s disease: an update. CNS Drugs. 2020;34:1025–1044. doi:10.1007/s40263-020-00754-0
- Hung AY, Schwarzschild MA. Treatment of Parkinson’s disease: what’s in the non-dopaminergic pipeline? Neurotherapeutics. 2014;11(1):34–46. doi:10.1007/s13311-013-0239-9
- Riederer P, Gerlach M, Muller T, Reichmann H. Relating mode of action to clinical practice: dopaminergic agents in Parkinson’s disease. Parkinsonism Relat Disord. 2007;13(8):466–479. doi:10.1016/j.parkreldis.2007.06.015
- Fuxe K, Ferré S, Genedani S, Franco R, Agnati LF. Adenosine receptor-dopamine receptor interactions in the basal ganglia and their relevance for brain function. Physiol Behav. 2007;92(1–2):210–217. doi:10.1016/j.physbeh.2007.05.034
- Schiffmann SN, Fisone G, Moresco R, Cunha RA, Ferre S. Adenosine A2A receptors and basal ganglia physiology. Prog Neurobiol. 2007;83(5):277–292. doi:10.1016/j.pneurobio.2007.05.001
- Jarvis MF, Williams M. Direct autoradiographic localization of adenosine A2 receptors in the rat brain using the A2-selective agonist, [3H]CGS 21680. Eur J Pharmacol. 1989;168(2):243–246. doi:10.1016/0014-2999(89)90571-2
- Rosin DL, Robeva A, Woodard RL, Guyenet PG, Linden J. Immunohistochemical localization of adenosine A2A receptors in the rat central nervous system. J Comp Neurol. 1998;401(2):163–186. doi:10.1002/(SICI)1096-9861(19981116)401:2<163::AID-CNE2>3.0.CO;2-D
- Svenningsson P, Hall H, Sedvall G, Fredholm BB. Distribution of adenosine receptors in the postmortem human brain: an extended autoradiographic study. Synapse. 1997;27(4):322–335. doi:10.1002/(SICI)1098-2396(199712)27:4<322::AID-SYN6>3.0.CO;2-E
- Ishiwata K, Mishina M, Kimura Y, Oda K, Sasaki T, Ishii K. First visualization of adenosine A2A receptors in the human brain by positron emission tomography with [11C]TMSX. Synapse. 2005;55(2):133–136. doi:10.1002/syn.20099
- Mori A. How do adenosine A(2A) receptors regulate motor function? Parkinsonism Relat Disord. 2020;80(Suppl 1):S13–s20. doi:10.1016/j.parkreldis.2020.09.025
- Saki M, Yamada K, Koshimura E, Sasaki K, Kanda T. In vitro pharmacological profile of the A2A receptor antagonist istradefylline. Naunyn Schmiedebergs Arch Pharmacol. 2013;386(11):963–972. doi:10.1007/s00210-013-0897-5
- LeWitt PA, Guttman M, Tetrud JW, et al. Adenosine A2A receptor antagonist istradefylline (KW-6002) reduces “off” time in Parkinson’s disease: a double-blind, randomized, multicenter clinical trial (6002-US-005). Ann Neurol. 2008;63(3):295–302. doi:10.1002/ana.21315
- Stacy M, Silver D, Mendis T, et al. A 12-week, placebo-controlled study (6002-US-006) of istradefylline in Parkinson disease. Neurology. 2008;70(23):2233–2240. doi:10.1212/01.wnl.0000313834.22171.17
- Hauser RA, Shulman LM, Trugman JM, et al. Study of istradefylline in patients with Parkinson’s disease on levodopa with motor fluctuations. Mov Disord. 2008;23(15):2177–2185. doi:10.1002/mds.22095
- Pourcher E, Fernandez HH, Stacy M, Mori A, Ballerini R, Chaikin P. Istradefylline for Parkinson’s disease patients experiencing motor fluctuations: results of the KW-6002-US-018 study. Parkinsonism Relat Disord. 2012;18(2):178–184. doi:10.1016/j.parkreldis.2011.09.023
- Kyowa Hakko Kirin UK L. A 16-week, double-blind, placebo-controlled, randomised, parallel-group, multicentre, international study to evaluate the efficacy and safety of 40 mg/day KW-6002 (istradefylline) and that of entacapone versus placebo as treatment for Parkinson’s disease in patients with motor response complications on levodopa therapy; 2005. Available from: https://clinicaltrials.gov/ct2/show/study/NCT00199394. Accessed June 29, 2022.
- Mizuno Y, Hasegawa K, Kondo T, Kuno S, Yamamoto M; Japanese Istradefylline Study Group. Clinical efficacy of istradefylline (KW-6002) in Parkinson’s disease: a randomized, controlled study. Mov Disord. 2010;25(10):1437–1443. doi:10.1002/mds.23107
- Mizuno Y, Kondo T; Japanese Istradefylline Study Group. Adenosine A2A receptor antagonist istradefylline reduces daily OFF time in Parkinson’s disease. Mov Disord. 2013;28(8):1138–1141. doi:10.1002/mds.25418
- Kyowa Hakko Kirin Pharma I. A phase 3, 12-week, double-blind, placebo-controlled, randomized, multicenter study to evaluate the efficacy of oral istradefylline 20 and 40 mg/day as treatment for subjects with moderate to severe Parkinson’s disease; 2016. Available from: https://www.clinicaltrials.gov/ct2/show/NCT01968031. Accessed June 29, 2022.
- LeWitt PA, Aradi SD, Hauser RA, Rascol O. The challenge of developing adenosine A(2A) antagonists for Parkinson disease: istradefylline, preladenant, and tozadenant. Parkinsonism Relat Disord. 2020;80(Suppl 1):S54–s63. doi:10.1016/j.parkreldis.2020.10.027
- Hauser RA, Hattori N, Fernandez H, et al. Efficacy of istradefylline, an adenosine A2A receptor antagonist, as adjunctive therapy to levodopa in Parkinson’s disease: a pooled analysis of 8 phase 2b/3 trials. J Parkinsons Dis. 2021;11(4):1663–1675. doi:10.3233/JPD-212672
- Jenner P, Mori A, Aradi SD, Hauser RA. Istradefylline - a first generation adenosine A2A antagonist for the treatment of Parkinson’s disease. Expert Rev Neurother. 2021;21(3):317–333. doi:10.1080/14737175.2021.1880896
- Takahashi M, Fujita M, Asai N, Saki M, Mori A. Safety and effectiveness of istradefylline in patients with Parkinson’s disease: interim analysis of a post-marketing surveillance study in Japan. Expert Opin Pharmacother. 2018;19(15):1635–1642. doi:10.1080/14656566.2018.1518433
- EMA Nouryant Assessment report. Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/nouryant. Accessed June 29, 2022.
- Center for Drug Evaluation and Research. Summary review: 022075Orig1s000. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2019/022075Orig1s000SumR.pdf. Accessed June 29, 2022.
- Center for Drug Evaluation and Research. Clinical review: NDA 022075. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2019/022075Orig1s000MedR.pdf. Accessed June 29, 2022.
- NOURIANZ™ (istradefylline) tablets, for oral use. US Prescribing information. Available from: https://www.nourianz.com/assets/pdf/nourianz-full-prescribing-information.pdf. Accessed June 29, 2022.
- Olanow CW, Kieburtz K, Rascol O, et al. Factors predictive of the development of Levodopa-induced dyskinesia and wearing-off in Parkinson’s disease. Mov Disord. 2013;28(8):1064–1071. doi:10.1002/mds.25364
- Grosset KA, Bone I, Grosset DG. Suboptimal medication adherence in Parkinson’s disease. Mov Disord. 2005;20(11):1502–1507. doi:10.1002/mds.20602
- Stocchi F. The levodopa wearing-off phenomenon in Parkinson’s disease: pharmacokinetic considerations. Expert Opin Pharmacother. 2006;7(10):1399–1407. doi:10.1517/14656566.7.10.1399
- Stocchi F, Jenner P, Obeso JA. When do levodopa motor fluctuations first appear in Parkinson’s disease? Eur Neurol. 2010;63(5):257–266. doi:10.1159/000300647
- Lewitt P, Hattori N, Mori A, et al. Efficacy of istradefylline, an A2A receptor antagonist, when added to levodopa (LD) and other medications for Parkinson’s disease (PD) [abstract]. Mov Disord. 2019;34(suppl 2):e54.
- Kaakkola S. Problems with the present inhibitors and a relevance of new and improved COMT inhibitors in Parkinson’s disease. Int Rev Neurobiol. 2010;95:207–225.
- Hattori N, Nomura M, Salzman P, et al. Frequency of dyskinesia as a function of baseline dyskinesia in patients with Parkinson’s disease treated with istradefylline, an adenosine A2A receptor antagonist. Mov Disord Clin Pract. 2020;7(S1):S13–S111.
- Bibbiani F, Oh JD, Petzer JP, et al. A2A antagonist prevents dopamine agonist-induced motor complications in animal models of Parkinson’s disease. Exp Neurol. 2003;184(1):285–294. doi:10.1016/S0014-4886(03)00250-4
- Kanda T, Jackson MJ, Smith LA, et al. Adenosine A2A antagonist: a novel antiparkinsonian agent that does not provoke dyskinesia in parkinsonian monkeys. Ann Neurol. 1998;43(4):507–513. doi:10.1002/ana.410430415
- Kanda T, Jackson MJ, Smith LA, et al. Combined use of the adenosine A(2A) antagonist KW-6002 with L-DOPA or with selective D1 or D2 dopamine agonists increases antiparkinsonian activity but not dyskinesia in MPTP-treated monkeys. Exp Neurol. 2000;162(2):321–327. doi:10.1006/exnr.2000.7350
- Grondin R, Bedard PJ, Hadj Tahar A, Gregoire L, Mori A, Kase H. Antiparkinsonian effect of a new selective adenosine A2A receptor antagonist in MPTP-treated monkeys. Neurology. 1999;52(8):1673–1677. doi:10.1212/WNL.52.8.1673
- Elmer L, Toyama K, Parno J, Braccia D, Ristuccia R, Mori A. Safety and efficacy of istradefylline, an adenosine A2A receptor antagonist, as a function of baseline dyskinesia (BL-dyskinesia) in Parkinson’s disease (PD): a pooled analysis of 4 studies [abstract]. Mov Disord. 2020;35(suppl 1):S393–S394.
- Zuzuárregui JRP, During EH. Sleep issues in Parkinson’s disease and their management. Neurotherapeutics. 2020;17(4):1480–1494. doi:10.1007/s13311-020-00938-y
- Avorn J, Schneeweiss S, Sudarsky LR, et al. Sudden uncontrollable somnolence and medication use in parkinson disease. Arch Neurol. 2005;62(8):1242–1248. doi:10.1001/archneur.62.8.1242
- Antonini A, Tolosa E, Mizuno Y, Yamamoto M, Poewe WH. A reassessment of risks and benefits of dopamine agonists in Parkinson’s disease. Lancet Neurol. 2009;8(10):929–937. doi:10.1016/S1474-4422(09)70225-X
- Bares M, Kanovský P, Rektor I. Excessive daytime sleepiness and ‘sleep attacks’ induced by entacapone. Fundam Clin Pharmacol. 2003;17(1):113–116. doi:10.1046/j.1472-8206.2003.00120.x
- ONGENTYS (opicapone) capsules, for oral use. Full prescribing information. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/212489s000lbl.pdf. Accessed June 29, 2022.
- STALEVO (carbidopa, levodopa and entacapone) tablets, for oral use. Full prescribing information. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/021485s042lbl.pdf. Accessed June 29, 2022.
- Mirapex® (pramipexole dihydrochloride). Full prescribing information. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2008/020667s014s017s018lbl.pdf. Accessed June 29, 2022.
- Jenner P, Mori A, Kanda T. Can adenosine A2A receptor antagonists be used to treat cognitive impairment, depression or excessive sleepiness in Parkinson’s disease? Parkinsonism Relat Disord. 2020;80(Suppl 1):S28–S36. doi:10.1016/j.parkreldis.2020.09.022
- Lazarus M, Oishi Y, Bjorness TE, Greene RW. Gating and the need for sleep: dissociable effects of adenosine A(1) and A(2A) receptors. Front Neurosci. 2019;13:740. doi:10.3389/fnins.2019.00740
- Huang ZL, Zhang Z, Qu WM. Roles of adenosine and its receptors in sleep-wake regulation. Int Rev Neurobiol. 2014;119:349–371.
- Suzuki K, Miyamoto M, Miyamoto T, et al. Istradefylline improves daytime sleepiness in patients with Parkinson’s disease: an open-label, 3-month study. J Neurol Sci. 2017;380:230–233. doi:10.1016/j.jns.2017.07.045
- Matsuura K, Kajikawa H, Tabei KI, et al. The effectiveness of istradefylline for the treatment of gait deficits and sleepiness in patients with Parkinson’s disease. Neurosci Lett. 2018;662:158–161. doi:10.1016/j.neulet.2017.10.018
- Baumann CR. Epidemiology, diagnosis and differential diagnosis in Parkinson’s disease tremor. Parkinsonism Relat Disord. 2012;18:S90–S92. doi:10.1016/S1353-8020(11)70029-3
- Pagan F, Parno J, Ristuccia R, Mori A, Istradefylline T-Y-Y. Effects on tremor dominant (TD) and postural instability and gait difficulty (PIGD) motor subtypes (4540). Neurology. 2021;96(15 Supplement):4540.
- Beiske AG, Loge JH, Hjermstad MJ, Svensson E. Fatigue in Parkinson’s disease: prevalence and associated factors. Mov Disord. 2010;25(14):2456–2460. doi:10.1002/mds.23372
- Stocchi F, Abbruzzese G, Ceravolo R, et al. Prevalence of fatigue in Parkinson disease and its clinical correlates. Neurology. 2014;83(3):215–220. doi:10.1212/WNL.0000000000000587
- Oved D, Ziv I, Treves TA, Paleacu D, Melamed E, Djaldetti R. Effect of dopamine agonists on fatigue and somnolence in Parkinson’s disease. Mov Disord. 2006;21(8):1257–1261. doi:10.1002/mds.20929
- Stocchi F. Benefits of treatment with rasagiline for fatigue symptoms in patients with early Parkinson’s disease. Eur J Neurol. 2014;21(2):357–360. doi:10.1111/ene.12205
- Lim TT, Kluger BM, Rodriguez RL, et al. Rasagiline for the symptomatic treatment of fatigue in Parkinson’s disease. Mov Disord. 2015;30(13):1825–1830. doi:10.1002/mds.26429
- Abe K, Fujita M, Yoshikawa H. Effectiveness of istradefylline for fatigue and quality of life in Parkinson’s disease patients’ and of their caregivers’. Adv Parkinson Dis. 2016;5:24–28. doi:10.4236/apd.2016.52004
- Ito H, Kamei T. Adenosine A2A receptor antagonist istradefylline might have efficacy to fatigue and depression in some patients of Parkinson’s disease [abstract]. Mov Disord. 2016;31(suppl 2):S626–S626.
- Shimo Y, Maeda T, Chiu S-W, et al. Influence of istradefylline on non-motor symptoms of Parkinson’s disease: a subanalysis of a 1-year observational study in Japan (J-FIRST). Parkinsonism Relat Disord. 2021;91:115–120. doi:10.1016/j.parkreldis.2021.09.015
- Pringsheim T, Day GS, Smith DB, et al. Dopaminergic therapy for motor symptoms in early Parkinson disease practice guideline summary: a report of the AAN guideline subcommittee. Neurology. 2021;97(20):942–957. doi:10.1212/WNL.0000000000012868
- REQUIP® (ropinirole hydrochloride) tablets. Prescribing information. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2008/020658s018s020s021lbl.pdf. Accessed June 29, 2022.
- Neupro (Rotigotine Transdermal System). Full prescribing information. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/021829s001lbl.pdf. Accessed June 29, 2022.
- Senard JM, Raï S, Lapeyre-Mestre M, et al. Prevalence of orthostatic hypotension in Parkinson’s disease. J Neurol Neurosurg Psychiatry. 1997;63(5):584–589. doi:10.1136/jnnp.63.5.584
- Ha AD, Brown CH, York MK, Jankovic J. The prevalence of symptomatic orthostatic hypotension in patients with Parkinson’s disease and atypical parkinsonism. Parkinsonism Relat Disord. 2011;17(8):625–628. doi:10.1016/j.parkreldis.2011.05.020
- Isaacson SH, Skettini J. Neurogenic orthostatic hypotension in Parkinson’s disease: evaluation, management, and emerging role of droxidopa. Vasc Health Risk Manag. 2014;10:169–176. doi:10.2147/VHRM.S53983
- Kujawa K, Leurgans S, Raman R, Blasucci L, Goetz CG. Acute orthostatic hypotension when starting dopamine agonists in Parkinson’s disease. Arch Neurol. 2000;57(10):1461–1463. doi:10.1001/archneur.57.10.1461
- Lang AE. Acute orthostatic hypotension when starting dopamine agonist therapy in Parkinson disease: the role of domperidone therapy. Arch Neurol. 2001;58(5):835. doi:10.1001/archneur.58.5.835
- Senard JM, Brefel-Courbon C, Rascol O, Montastruc JL. Orthostatic hypotension in patients with Parkinson’s disease: pathophysiology and management. Drugs Aging. 2001;18(7):495–505. doi:10.2165/00002512-200118070-00003
- Suzuki K, Miyamoto T, Miyamoto M, Uchiyama T, Hirata K. Could istradefylline be a treatment option for postural abnormalities in mid-stage Parkinson’s disease? J Neurol Sci. 2018;385:131–133. doi:10.1016/j.jns.2017.12.027
- Fujioka S, Yoshida R, Nose K, et al. A new therapeutic strategy with istradefylline for postural deformities in Parkinson’s disease. Neurol Neurochir Pol. 2019;53(4):291–295. doi:10.5603/PJNNS.a2019.0036
- Iijima M, Orimo S, Terashi H, et al. Efficacy of istradefylline for gait disorders with freezing of gait in Parkinson’s disease: a single-arm, open-label, prospective, multicenter study. Expert Opin Pharmacother. 2019;20(11):1405–1411. doi:10.1080/14656566.2019.1614167
- Kitta T, Yabe I, Kanno Y, et al. Long-term outcome of adenosine A2A receptor antagonist on lower urinary tract symptoms in male Parkinson disease patients. Clin Neuropharmacol. 2018;41(3):98–102. doi:10.1097/WNF.0000000000000281
- Nagayama H, Kano O, Murakami H, et al. Effect of istradefylline on mood disorders in Parkinson’s disease. J Neurol Sci. 2019;396:78–83. doi:10.1016/j.jns.2018.11.005