
Abstract
Background
Vertical transmission of Human Immunodeficiency Virus (HIV) is the primary route of infection among children. Ethiopia is among the top ten countries in the world with the highest burden of HIV infections among children. Therefore we aimed to assess mother to child transmission (MTCT) of HIV and associated factors among HIV exposed infants (HEIs).
Methods
A cross-sectional study was conducted using retrospective data collected from HEIs paired with their mothers who had received the services in prevention of mother to child transmission (PMTCT) programs from January 2014 to December 2017 in public health facilities in Dessie town. Data of a total of 313 HEIs paired with their mothers were obtained by using semi-structured data extraction proforma from their medical records. The data were processed in Epi-info version 7.1.2.0 and analyzed using SPSS version 22. Crude and adjusted odds ratios with their 95% confidence intervals and p-value were used to identify significant factors.
Results
The prevalence of HIV among exposed infants was 3.8%. Absence of maternal antenatal care visit (AOR = 4.6, 95% CI: 1.17–17.99), home delivery (AOR = 4.2, 95% CI: 1.04 −16.76), absence of antiretroviral intervention to the mother (AOR= 5.7, 95% CI: 1.10–29.36), and failure to initiate nevirapine prophylaxis for the infant (AOR = 5.3, 95% CI: 1.11 −25.44) were significant factors of MTCT of HIV.
Conclusion
Prevalence of MTCT of HIV was low (3.8%) in Dessie town public health facilities. Having ANC visit, delivery at health facility, maternal ARV drug intake, and infant ARV prophylaxis were the significant protective factors against MTCT of HIV. Promoting ANC service utilization among pregnant women and providing counseling as well as setting up linkage with PMTCT and giving ARV intervention to all HIV positive pregnant women and timely initiation of NVP prophylaxis to all HEIs should be recommended by the minister of health and health facilities.
Introduction
Human immunodeficiency virus (HIV) continues to be a major global public health issue. Globally, an estimated 36.7 million people have died from AIDS-related illnesses since the start of the epidemic. In 2015, 1.1 million people died from HIV-related causes and 2.6 million children were living with HIV and the majority were found in Africa.Citation1–Citation3 Children < 15 years old accounted for an estimated 190,000 new HIV infections and 130,000 deaths due to HIV/AIDS in 2014.Citation4 In Ethiopia also, an estimated 753,100 people are living with HIV with a declining national HIV prevalence from 1.5% in 2011 to estimated 1.15 in 2015; urban areas are more affected than rural areas while females are twice affected than male population with HIV.Citation5
Mother to child transmission (MTCT) of HIV is the passing of HIV from the mother to her child during pregnancy, labor, delivery or breast-feeding and it is the primary method of infection among children. Over 90 percent of new infections in infants and young children occur through MTCT. A higher percentage of HIV-infected children (70–80%) acquire the virus during intrapartum, intrauterine infection accounts for 20–30% and breastfeeding is responsible for as much as 40% of infections in resource-limited countries.Citation6 A study conducted in Brazil with 1200 HIV-exposed children showed that MTCT rate of HIV was 9.16%.Citation7 Another study in China showed that MTCT rate of HIV was 4.8%.Citation8 Meanwhile the rates of MTCT of HIV in the breast feeding population were 2.9% in Uganda, 4.1% in Namibia, and 3.3% in Swaziland.Citation9 Among infants born to HIV-infected mothers, the highest MTCT of HIV rates (34%) were reported in Africa, Congo and the lowest rate (2%) was reported in Botswana whereas the rate in Ethiopia was 25%Citation10 and the rate in Tanzania was 9.6%.Citation11
In Ethiopia MTCT rates of HIV among HIV exposed infants (HEIs) were 15.7%, 17%, and 10% in Dire Dawa City Dilchora referral hospital,Citation12 Jimma University specialized hospital,Citation13 and Gondar University referral hospital,Citation14 respectively.
Several risk factors influence the rate of vertical transmission which includes advanced disease (stage 3 and 4), absence of antiretroviral (ARV) intervention to the mother and the infant, vaginal delivery, mastitis, nipple fissures, breast abscess, mixed breast and bottle feeding, and long duration of breastfeeding (>12 months).Citation15
The World Health Organization (WHO) promotes a comprehensive approach for the prevention of mother to child transmission (PMTCT) of HIV programs which includes, preventing new HIV infections among women of childbearing age, preventing unintended pregnancies among women living with HIV, preventing HIV transmission to the baby and providing appropriate treatment, care, and support to mothers living with HIV, their children, and families.Citation16 Without PMTCT interventions, the likelihood of HIV passing from mother-to-child is 15% to 45%. Moreover, antiretroviral treatment and other effective PMTCT interventions can reduce this risk to below 5%.Citation16
Services for PMTCT of HIV have been implemented in Ethiopia since 2001.Citation17 WHO had implemented option A (women receive antenatal and intra partum antiretroviral prophylaxis along with an antiretroviral postpartum “tail” regimen to reduce risk of drug resistance, while infants receive postpartum antiretroviral prophylaxis throughout the duration of breastfeeding), option B (all pregnant and lactating women with HIV initially are offered ART – beginning in the antenatal period and continuing throughout the duration of breastfeeding. At the end of breastfeeding those women who do not yet require ART for their own health would discontinue the prophylaxis and continue to monitor their CD4 count, eventually re-starting ART when the CD4 falls below 350 cells/mm3) and option B+ (in which all pregnant women living with HIV are offered life-long ART, regardless of their CD4 count) PMTCT guidelines at different times.Citation18 Ethiopia launched option B+ in 2013.Citation19
HIV/AIDS continues to be one of the top priorities on the health sector's agenda for Ethiopia.Citation5 Ethiopia is among the top ten countries in the world with the highest burden of HIV infections among children due to MTCT,Citation20 even though Ethiopia reached a 97% target achievement in implementing PMTCT at national level and has seen significant gains in PMTCT since the start of the program.Citation21 MTCT of HIV has remained a challenge for the country.Citation17
Further studies and investigation of different factors associated with MTCT of HIV are needed to achieve national PMTCT program goals of reducing MTCT of HIV to < 2% by 2020.Citation22 Therefore, the aim of this study was to assess the prevalence of MTCT of HIV and associated factors among HEIs in public health facilities at Dessie town, Ethiopia. The study will provide baseline data for the country in light of current option B+ PMTCT interventions being undertaken in reducing MTCT of HIV.
Materials and Methods
Study Area Design and Period
The study was conducted in Dessie town, Amhara regional state, which is 401 km away from Addis Ababa, the capital city of Ethiopia. The study was conducted in public health facilities in Dessie town namely, Dessie referral hospital, Borumeda hospital, and three health centers (Dessie, Segno Gebaya, and Buanbuawha health center).
A health facility-based cross-sectional study was conducted using retrospective data collection by reviewing the medical records of HEIs paired with their mothers who had received PMTCT service from January 2014 to December 2017 in public health facilities in Dessie town.
Populations and Samples
Study population comprised all 347 HEIs paired with their mothers who had enrolled at PMTCT clinic in public health facilities from January 2014 to December 2017 in Dessie town, South Wollo zone, Amhara regional state, Ethiopia. Samples comprised 313 HEIs who had a final confirmed HIV test and whose medical records could be assessed (of both mother and infant).
Method of Data Collection and Data Quality Assurance
The data were collected using a semi-structured form developed from the national HEI follow-up card and maternal intake forms. Five experts checked the content validity of the research tool. Data were collected for a period of two weeks by five trained nurses with two supervisors. Final result of HIV test and medical records of HEIs were obtained from HEIs recording logbooks and maternal medical records were taken from HEI follow up cards. Data collectors checked the presence of both HEI follow up card and maternal intake forms before collecting the data. The quality of the data was ensured through training of data collectors, regular supervision, immediate feedback, and spot-checking. Pretest was done on 5% of the population.
Research Tools
The research tool used for data collection was a pretested semi-structured questionnaire, and the study variables included the following.
Dependent Variable
Mother to child HIV transmission.
Independent Variables
Socio-demographic characteristics of HEIs and their mothers (age of the mother, sex of the infant, maternal educational status, maternal occupation, residence). Prenatal factors (ANC follow up, number of ANC visits). Intrapartum factors (place of delivery, weight of the infant at delivery, mode of delivery). Post-natal factors (breast infection/crack, infant's age at diagnosis, age at enrollment in PMTCT clinic, infants feeding practice)'. ARV intervention and clinical factors (maternal ARV intervention, abnormal findings suggesting HIV, infants' ARV prophylaxis, duration of intervention, WHO clinical stage near/at delivery).
Operational Definition
Abnormal Breast Condition
Any breast conditions like mastitis, ulcer, cracks, Candida infection, engorgement or fissures.Citation15
Abnormal Findings Suggesting HIV Infection
Generalized lymphadenopathy, oral candidiasis, purulent ear discharge, pneumonia or lower respiratory tract infection, persistent diarrhea, hepatosplenomegaly, severe skin lesions, persistent fever etc.Citation15
HIV Exposed Infants (HEIs)
Infant born to HIV-infected mother or HIV antibody positive infant <18 months of age.Citation6
Mother to Child Transmission (MTCT) of HIV
Determined by infant’s final (confirmed) HIV test result which was divided into the following two groups.
For non-breast-fed infant: - HIV DNA/PCR result for infants aged <18 months or HIV antibody test result for infants aged ≥ 18 months.
For breast-fed infant: - HIV DNA/PCR result for infants aged <18 months after cessation of breast feeding or HIV antibody test result for infants aged ≥ 18 months 6 weeks after cessation of breast feeding.Citation15
Data Processing and Analysis
All data collection forms were checked for completeness and consistency thereafter, the data were processed in EPI info (version 7.1.2.0) and analyzed using SPSS (Statistical Package for Social Sciences) version 22. Descriptive statistics (frequency, percentage, mean) were used to describe the studied variables. Bivariate logistic regression and multiple logistic regressions, in which crude and adjusted odds ratio with 95% CI and p-value were computed to prove the association between and among variables. A p-value less than 0.05 was considered as a significant association.
Ethical Statement
Ethical clearance was obtained from Addis Ababa university Institutional review board and after approval by Institutional review board, a supporting letter was written to each health facility namely Dessie referral hospital, Borumeda hospital, Dessie health center, Segno Gebayahealth center, and Buanbuawha health center. Since the study was a retrospective chart review, patient consent to review their medical records was not required by the Institutional Review Board of Addis Ababa University, but consent to review medical records was secured from respective study facilities and since the outcome of the study will be disseminated for the facility as feedback, Addis Ababa university Institutional Review Board requested a waiver of patient consent requirement and patient data confidentiality and compliance was ensured in accordance with the Declaration of Helsinki.
Result
Prevalence of Mother to Child Transmission of HIV
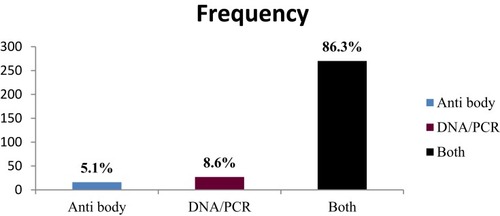
The proportion of MTCT of HIV was 3.8% (95% CI: 1.6–5.75). Majority (86.3%) of infants were diagnosed using DNA/PCR and a large proportion (91.7%) of HEIs were diagnosed by the age of > 6 months ( and ).
Figure 1 The age of HIV exposed infants during final diagnosis of HIV, at public health facilities in Dessie town, Ethiopia, 2017 (n =313).
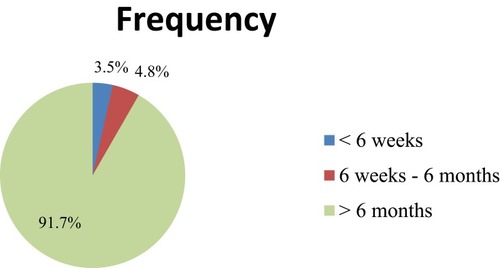
Figure 2 Method of HIV diagnosis for HIV exposed infants, at public health facilities in Dessie town, Ethiopia, 2017 (n = 313).
Socio-Demographic Characteristics of HEIs and Their Mothers
Nearly half (52.4%) of HEIs were males. Majority of mothers (78.6%) were in the age group of 25–35 years and 70.3% of them lived in urban areas ().
Table 1 Socio-Demographic Characteristics of HEIs and Their Mothers at Public Health Facilities in Dessie Town, Ethiopia, 2017 (n = 313)
Prenatal, Intrapartum, and Post-Natal Findings
Majority (82.1%) of mothers had ANC visit, 83.7% of them had given birth at hospital, 97.6% of them had SVD and all breast-feeding mothers had normal breasts. Five-sixths (84.3%) of HEIs had ≥ 2500 g birth weight and only 4.8% of infants received supplementary food during the first 6 months ().
Table 2 Frequency and Percentage of Prenatal, Intranatal, and Postnatal Findings of MTCT of HIV at Public Health Facilities in Dessie Town, Ethiopia, 2017 (n = 313)
ARV Intervention and Clinical Findings
Almost all mothers (92.7%) received ARV, of which 64.5% received ARV prior to pregnancy, 95.5% during childbirth, and 93.3% of HEIs had received NVP prophylaxis ().
Table 3 Frequency of Anti-Retroviral Intervention and Clinical Finding of HEIs and Their Mothers at Public Health Facilities in Dessie Town, Ethiopia, 2017 (N= 313)
Factors Associated with MTCT of HIV
Bivariate and Multivariate Analysis of Factors Associated with MTCT of HIV
In the bivariate analysis, factors associated with MTCT of HIV (p – value < 0.2) were education of mother, residence, ANC visit, place of delivery, supplementary feeding practice in the first 6 months, age of the infant at enrollment in the PMTCT clinic, maternal ARV before giving birth and NVP intervention to the infant.
After controlling the effects of all the other variables using multivariate logistic regression, mothers who did not attend ANC follow up were 4.6 times more likely to transmit the virus to their infants than mothers who had ANC visit (AOR = 4.6, 95% CI: 1.17–17.99, p = 0.029).
Mothers who had home delivery were 4.2 times more likely to transmit the virus to their infants compared with mothers who delivered in a health facility (AOR = 4.2, 95% CI: 1.04–16.76, P = 0.044).
The other variable, which showed significant association in the multivariate analysis was ARV intervention to the mother and the infant. The odds of viral transmission to the infant were 5.7 times higher in mothers without ARV intervention compared with ARV intervention prior to delivery (AOR = 5.7, 95% CI: 1.10–29.36, P = 0.038). Likewise, the odds of being HIV positive were 5.3 times higher among infants without NVP intervention than infants who received NPV (AOR =5.3, 95% CI: 1.11–25.44, P= 0.037) ().
Table 4 Bivariate and Multivariate Logistic Regression Analysis of Factors Associated with MTCT of HIV Among HEIs at Public Health Facilities in Dessie Town, Ethiopia, 2017 (n = 313)
Discussion
The prevalence of MTCT of HIV was low, which is comparable with the study conducted in North West Ethiopia (3.8% and 4.16%, respectively).Citation23 But lower than in other studies conducted in the other areas of Ethiopia (15.7% in Dire Dawa,Citation12 17% in Jimma,Citation13 10% in Gondar,Citation14 and 10.1% in south Gondar).Citation24 The low prevalence of MTCT of HIV may be due to option of PMTCT interventions in HEIs. This study was conducted on HEIs who received intervention with option B+ which resulted in a low MTCT of HIV as compared with previously implemented options. This finding was also supported by option B+ implementation in Malawi which resulted in a very low vertical transmission of HIV.Citation25 This was concordant with option B+ implementation in Uganda (2%), Namibia (4.1%), and Swaziland (3.3%).Citation1 Similarly, this study was also comparable with the finding of a study conducted in China (4.8%).Citation8
ANC visits were significantly associated with MTCT of HIV. HEIs whose mothers had no ANC visit were more likely to have a positive result than infants whose mothers attended ANC. This might be because routine HIV testing at ANC visit enablesearly identification and initiation of ARV drugs for HIV positive pregnant mothers and continued counseling for institutional delivery readiness during follow up. But other studies conducted in Ethiopia showed no significant association between ANC visit and MTCT of HIV.Citation13,Citation26 This might be as a resulted of lack of integration of the PMTCT interventions with ANC services in option B, whereas with option B+ there is good linkage (if the mother is HIV infected she will be linked to ART clinic to initiate ARV regardless of her CD4 count and stage).
Place of delivery was significantly associated with MTCT of HIV. The odds of MTCT of HIV were higher in home delivery than health facility delivery. This was concordant with the study conducted in south Gondar zone (AOR = 6.1), South west Ethiopia (AOR=8.1), and in Dire Dawa (AOR = 3.35).Citation12–Citation14 This might be due to HIV testing for mothers with unknown HIV status who delivered at health facility and immediate ARV intervention for mothers and their infants if the test was positive. In addition, safe delivery practice and appropriate post-natal care during health facility delivery might support this significant association. But place of delivery did not show significant association in a case control study conducted at Assela, Adama, and Bishoftu hospitals.Citation27
Maternal ARV drug intake was also significantly associated with MTCT of HIV. Absence of maternal ARV drug intake prior to labor/delivery (during perinatal period) seemed to increase the MTCT of HIV, which is similar to the studies conducted in Ethiopia,Citation14,Citation23 as well as in Brazil and China which indicated that maternal ARV drug intake was a significant determinant of MTCT of HIV.Citation7 This might be as a result of maternal ARV drug intake causing the reduction of maternal viral load and reduced risk of viral transmission to their infants.
The MTCT of HIV was higher in infants who did not receive NVP prophylaxis than in those who received NVP. This was in agreement with studies conducted in Ethiopia as well as in Brazil which found that ARV prophylaxis for infants was a significant determinant of MTCT of HIV.Citation12,Citation23,Citation28 This might be due to the viral suppression effect of NVP, which is a non nucleoside reverse transcriptase inhibitor, by binding to reverse transcriptase, thereby blocking RNA and DNA dependent DNA polymerase actions including HIV replication. On the other hand, a study conducted in Gondar referral hospital, Ethiopia, found that infant ARV intervention was not significantly associated with MTCT of HIV.Citation14 This might be due to inadequacy of samples, or due to uncontrolled confounders.
Conclusion
Prevalence of MTCT of HIV was 3.8%. Having ANC visit, delivery at health facility, maternal ARV drug intake, and infant ARV prophylaxis were the significant protective factors against MTCT of HIV. Promoting ANC service utilization among pregnant women and providing counseling as well as setting up linkage with PMTCT and giving ARV intervention to all HIV positive pregnant women and timely initiation of NVP prophylaxis to all HEIs should be recommended by minister of health and health facilities.
Limitation of the Study
Since this research retrospectively collected data from secondary sources, studied factors were based on routinely recorded information, which may not have covered all risk factors of MTCT.
Abbreviations
3TC, Lamivudine; ABC, Abacavir; AIDS, Acquired Immunodeficiency Virus; ANC, Antenatal Care; AOR, Adjusted odds ratio; ART, Antiretroviral Therapy; ARV, Antiretroviral; AZT, Zidovudine; CI, confidence interval; CS, Cesarean Section; EDHS, Ethiopian Demographic and Health Survey; HEI, HIV Exposed Infant; HIV, Human Immunodeficiency Virus; MTCT, Mother to Child Transmission; NVP, Nevirapine; PCR, Polymerase Chain Reaction; SVD, Spontaneous Vaginal Delivery; WHO, World Health Organization.
Ethics Approval and Consent to Participate
Ethical clearance and ethical approval were obtained from Institutional Review Board of Addis Ababa University, for four authors on December 2017.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Author Information
Yibeltal Asmamaw Yitayew is a lecturer in the Department of Nursing, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia. Daniel Mengistu Bekele is a lecturer in the School of Nursing and Midwifery, College of Health Science, Addis Ababa University, Addis Ababa, Ethiopia. Birhanu Wondimeneh Demissie is a lecturer in the Department of Nursing, College of Medicine and Health Science, Wolaita Sodo University, Wolaita Sodo, Ethiopia. Zeleke Argaw Menji is a lecturer in the School of Nursing and Midwifery, College of Health Science, Addis Ababa University, Addis Ababa, Ethiopia.
Author Contributions
All authors had substantial contributions to conception and design, acquisition of data, analysis and interpretation of data; drafting the article and revising it critically for important intellectual content; have read and approved the final manuscript version to be published; and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Acknowledgments
The authors would like to thank Addis Ababa University for funding this study. We would also like to thank all study participants, supervisors, and data collectors for their unreserved efforts and willingness to take part in this study.
Disclosure
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- UNAIDS. Global HIV statistics fact sheet 2016. Available from: www.unaids.org.resources.fact.sheetaccessed. Accessed 2016.
- UNICEF. Annual report 2015. Available from: www.unicef.org.index.92018. Accessed 2017.
- AIDS.gov. global statistics. Available from: www.aids.gov. Accessed 2016.
- UNAIDS. How AIDS changed everything—MDG6: 15 years, 15 lessons of hope from the AIDS response 2015. Available from: www.unaids.org.files.media.asset. Accessed 2016.
- WHO. Ethiopia update sheet on HIV/AIDS 2015. Available from: www.afro.who.int. Accessed 2017.
- Robert MBF, Joseph W, Nina F, Richard E. Nelson Textbook of Pediatrics. 20th ed. Philadelphia: Elsevier; 2016.
- da Cruz Gouveia PA, da Silva GAP, de Fatima Pessoa Militão de Albuquerqu M, Pedro Alves da Cruz Gouveia. Factors associated with mother-to-child transmission of the human immunodeficiency virus in Pernambuco, Brazil, 2000–2009. Trop Med Int Health. 2013;18(3):276–285. doi:10.1111/tmi.1204223279690
- Qian Wang LW, Marchetti L, Parlanti P, et al. Timely antiretroviral prophylaxis during pregnancy effectively reduces HIV mother-to-child transmission in eight counties in China: a prospective study during 2004–2011. Sci Rep. 2016;6:1–8. doi:10.1038/s41598-016-0001-828442746
- UNAIDS. On the fact - track to an AIDS free generation - UNAIDS 2016. Available from: www.unaids.org.global.plan. Accessed2016.
- Andrew Hill TD, Levi J. Katherine heath and Carmen Pérez Casas higher risks of mother-to-child HIV transmission in countries with lower HIV prevalence. J Virus Eradication. 2015;1(4):257
- Mwendo EM, Mtuy TB, Renju J, et al. Effectiveness of prevention of mother-to-child HIV transmission programmes in Kilimanjaro region, northern Tanzania. Trop Med Int Health. 2014;19(3):267–274. doi:10.1111/tmi.1225524386998
- Fisseha W, Damtew B. Mother-to-child transmission of hiv infection and its determinants among exposed infants on care and follow-up in Dire Dawa City, Eastern Ethiopia. AIDS Res Treat. 2016;2016:6.
- TAD BB, Sisay K, Gurmessa A, Seyoum D, Tadesse M. Mother to child HIV transmission and its predictors among HIV-exposed infants: a retrospective follow-up study in Southwest Ethiopia. J AIDS Clin Res. 2016;7(9):1–7.
- Digsu M. Mother - to - child transmission of HIV - and its predictors among HIV - exposed infants at aPMTCT clinic in Nortwest Ethiopia. BioMed Center. 2013;13:398.
- Ethiopia M. National Comprehensive PMTCT Training Manuals. Addis Ababa: Minister of Health; 2016.
- WHO. PMTCT stratagic vision 2010–2015. Available from: www.who.int.hiv.mtct.strategy. Accessed 2016.
- USAID. Accelerated plan for scaling up of MTCT service in ethiopia 2014. Available from: www.usaid.gov.pdf.docs. Accessed 2017.
- WHO. Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection. Geneva: 2013 Available from: www.who.int.arv2013.download. Accessed 2016.
- UNICEF. Ethiopia launched option B+ 2014. Available from: www.unicef.org.ethiopia. Accessed 2016.
- IATT. Ethiopia national EMTCT plan 2012. Available from: www.emtct.iatt.org.uploads. Accessed 2017.
- MOH. health sector transformation plan - ethiopian midwive association 2015. Available from: www.midwives.org.et.sites.default.files. Accessed 2017.
- Health EMo. PMTCT 2015 Available from: http://www.moh.gov.et/pmtct. Accessed 2016.
- Tariku Tadele AT, Tadele T. Incidences and predictors of HIV positivity among infants who born from HIV positive mother who have follow up at two hospitals of southern Ethiopia. Sci J Public Health. 2014;2(5):431–439. doi:10.11648/j.sjph.20140205.19
- Berhan Z, Abebe F, Gedefaw M, Tesfa M. Prevalence of HIV and associated factors among infants born to HIV positive women in Amhara Region, Ethiopia. Int J Clin Med. 2014;5:464–474. doi:10.4236/ijcm.2014.58065
- Leach-Lemens C Option B+ cuts mother-to-child HIV transmission dramatically in Malawi. Available from: AIDS map.www.msh.org/news-events/stories/option-b-in-malawi. Accssessed 2017.
- Olana T, Bacha T, Worku W, Tadesse BT. Early infant diagnosis of HIV infection using DNA-PCR at a referral center: an 8 years retrospective analysis. AIDS Res Ther. 2016;13:29. doi:10.1186/s12981-016-0112-027617023
- Burusie A Deyessa N. Determinants of mother to child HIV transmission (HIV MTCT), A case control study in Assela, Adama and Bishoftu Hospitals, Oromia Regional State,Ethiopia. Cell & Developmental Biology. 2015;4(2):1–12.
- Ligia MD, de Lemos JL, Rutherford GW, et al. Maternal risk factors for HIV infection in infants in northeastern Brazil. Int J Inf Dis. 2013;17:913–918. doi:10.1016/j.ijid.2013.04.015