
Abstract
Background
The rise in community-acquired urinary tract infections (UTIs) with extended-spectrum β-lactamase (ESBL)-producing Escherichia coli strains raises the question of how to treat these infections effectively in pediatric outpatients. Amikacin has shown promising in vitro activity against ESBL-producing urinary isolates of E. coli; however, clinical data are limited.
Objective
To investigate the clinical and microbiological outcomes of community-acquired lower UTIs caused by ESBL-producing E. coli treated with outpatient amikacin in children.
Materials and methods
A retrospective cohort study was performed on pediatric patients aged ≥2 to 18 years treated as outpatients with intramuscular amikacin (given at a dose of 15 mg/kg/day once daily) for community-acquired lower UTIs caused by ESBL-producing E. coli, between January 2015 and December 2016.
Results
A total of 53 pediatric patients (38 females) were enrolled in this study. The median age was 4.7 years (range 3–12 years). All E. coli isolates were susceptible to amikacin with minimum inhibitory concentrations of ≤4 mg/L. The median duration of amikacin treatment was 6 days (range 3–7 days). Favorable clinical and bacteriological responses were observed in 51 of 53 (96%) patients. Development of resistance during treatment with amikacin was seen in only 1 patient (2%), who failed to respond to amikacin treatment and developed acute pyelonephritis with bacteremia. Relapsed lower UTI after initial treatment response occurred in 1 patient (2%) 2 weeks after completion of amikacin treatment. All patients had normal serum creatinine values at baseline, and no significant nephrotoxicity or ototoxicity was observed in any of the patients.
Conclusion
Our study suggests that once-daily intramuscular amikacin could be an alternative option for outpatient treatment of community-acquired lower UTIs caused by amikacin-susceptible ESBL-producing E. coli in pediatric patients with normal renal function, when there are no suitable oral antibiotics.
Introduction
The rise in community-acquired urinary tract infections (UTIs) with extended-spectrum β-lactamase (ESBL)-producing Escherichia coli strains is becoming a therapeutic challenge in children since there are limited treatment options, especially in outpatient settings.Citation1–Citation5 ESBLs are enzymes that confer resistance to most β-lactam antibiotics, including penicillins, cephalosporins, and aztreonam. Infections with ESBL-producing organisms have been associated with poor outcomes, and the carbapenems are regarded as the drugs of choice for the treatment of severe infections caused by such organisms.Citation6 However, the increase in their use for less severe situations promoted the emergence and spread of resistant strains, especially carbapenemase-producing Enterobacteriaceae, resistant to most available antimicrobials.Citation7 Therefore, it has become imperative to investigate alternative carbapenem-sparing agents for treatment of UTIs caused by ESBL-producing E. coli.
Aminoglycosides can provide excellent coverage for UTI, and meta-analysis of available randomized evidence recommends adoption of a once-daily dosing in children for potential outpatient treatment.Citation8 Low resistance to amikacin in urinary isolates of ESBL-producing E. coli is described worldwide both in children and adults.Citation2,Citation9 However, there is limited clinical evidence supporting the use of amikacin for the treatment of UTIs caused by ESBL-producing bacteria in children. In this era of increasing antibiotic resistance, we therefore aimed to investigate the clinical and microbiological outcomes of community-acquired lower UTIs due to ESBL-producing E. coli treated with outpatient amikacin in children.
Material and methods
Study design and patients
This retrospective study was conducted between January 2015 and December 2016 in the pediatric infectious diseases outpatient clinic of Erzurum Research and Training Hospital, a tertiary-care hospital in Turkey. Pediatric patients treated with outpatient amikacin for community-acquired lower UTIs due to ESBL-producing E. coli were screened for study enrollment. Inclusion criteria were: 1) age ≥2 to 18 years, 2) presence of at least one of the typical lower UTI symptoms such as dysuria, frequency, urgency, new onset incontinence, hematuria, abdominal or suprapubic pain, 3) pyuria (≥10 white blood cells/high power field), 4) positive urine dipstick for nitrites and/or leukocyte esterase, 5) positive monomicrobial urine culture (≥100,000 colony-forming units [CFU]/mL for midstream urine, and ≥50,000 CFU/mL for catheter urine) for ESBL-producing E. coli, which was susceptible to amikacin but resistant to available oral antibiotics, 6) outpatient treatment with amikacin monotherapy at least 3 days.
Amikacin was given intramuscularly at a dose of 15 mg/kg once daily, as recommended by the American Academy of Pediatrics.Citation10 Urine specimens were obtained by transurethral bladder catheterization in children who were not toilet-trained and by midstream clean-catch method in toilet-trained children. Bag urine samples were not used for urinalysis and urine culture.
Community-acquired UTI was defined as a UTI episode in which, at the time the index urine sample was submitted, the patient was not hospitalized and had not been previously hospitalized during the preceding 30 days. The exclusion criteria were as follows: 1) positive urine culture ≥72 h after hospital admission or hospital stay within the preceding month, 2) asymptomatic bacteriuria (defined as a positive urine culture without any clinical manifestations of infection), 3) acute pyelonephritis (defined as having fever with body temperature ≥38°C and abdominal or flank pain in older children, and nonspecific signs such as irritability and vomiting in younger children), 4) complicated UTI (defined as an infection in the urinary tract with functional or structural abnormalities such as acute or chronic renal insufficiency, nephrolithiasis, vesicoureteral reflux, neurogenic bladder, and use of permanent urinary catheters or intermittent catheterization), 5) history of hypersensitivity or serious toxic reactions to aminoglycosides, 6) pre-existing renal insufficiency, 7) pre-existing hearing or vestibular dysfunction, 8) treatment with an empiric antimicrobial agent active against ESBL-producing E. coli or one that provides clinical improvement in UTI symptoms despite in vitro resistance, 9) patients with insufficient follow-up data.
Data collection
The following data were extracted from the patient’s electronic medical records, and Microbiology Laboratory database: baseline patient demographics (age, gender), presence and duration of signs and symptoms of UTI at admission, previous history of UTI, healthcare exposures or hospital stay within 3 months, previous antibiotic use within 3 months, use of empiric antibiotic therapy, use of antimicrobial prophylaxis, initial and control urinalysis, urine cultures and antimicrobial susceptibility test results, baseline renal function tests (serum creatinine, blood urea nitrogen) that were obtained before the initiation of amikacin treatment, follow-up serum creatinine levels, the duration of amikacin treatment, clinical and microbiological response to amikacin treatment, treatment-related adverse effects, and UTI-related hospital re-admission within 30 days after completion of amikacin treatment.
Microbiological methods
The urine samples were plated on Blood Agar and Eosin-Methylene Blue Agar (Biomerieux, Marcy l’Etoile, France) by the semi-quantitative plating method using the calibrated loop technique (0.001 mL). Inoculated plates were incubated aerobically at 37°C for 18 to 24 h. Identification and susceptibility testing of bacteria was performed by using the BD Phoenix automated microbiology system (Becton Dickinson Diagnostic Systems, Sparks, MD, USA) according to the manufacturer’s instructions. Antimicrobial susceptibilities and ESBL production were determined according to the European Committee on Antimicrobial Susceptibility Testing guidelines.Citation11 The Minimal Inhibitory Concentration (MIC) susceptibility breakpoints used for the antibiotics tested were as follows: ampicillin ≤8 mg/L, amoxicillin–clavulanate ≤8/2 mg/L, ceftriaxone ≤1 mg/L, cefuroxime ≤8 mg/L, ceftazidime ≤1 mg/L, cefepime ≤1 mg/L, aztreonam ≤1 mg/L, ciprofloxacin ≤0.5 mg/L, amikacin ≤8 mg/L, gentamicin ≤2 mg/L, netilmicin ≤2 mg/L, ertapenem ≤0.5 mg/L, imipenem ≤2 mg/L, meropenem ≤2 mg/L, piperacillin ≤8 mg/L, piperacillin–tazobactam ≤8/4 mg/L, trimethoprim-sulfamethoxazole (TMP-SMX) ≤2/38 mg/L, colistin ≤2 mg/L, tigecycline ≤1 mg/L. These methods and the breakpoints for susceptibility remained unchanged during the study period.
Outcomes
The primary outcomes of the study were clinical and microbiological outcomes of UTIs. As secondary outcome, we evaluated the development of nephrotoxicity and ototoxicity associated with amikacin. Follow-up medical records of patients were reviewed to assess the efficacy (based on clinical and microbiological outcomes) and adverse events (nephrotoxicity and ototoxicity) of amikacin treatment. All of the efficacy and toxicity outcomes were evaluated at outpatient clinic visits on the third day of and at the end of the treatment. Control urine cultures were obtained on the third day of the amikacin treatment. At the visits, the patients were encouraged to return whenever symptoms occur that could be related to UTI.
Clinical outcome was classified as favorable clinical response (resolution of presenting symptoms of UTI without requirement of any additional antibiotics at the end of the amikacin treatment) and poor clinical response (persistence or progression of presenting symptoms of UTI during amikacin treatment). Microbiological outcome was classified as favorable bacteriological response (eradication of the causative microorganism in the control urine culture) and poor bacteriological response (persistence of the causative microorganism on control urine culture). Relapse was defined as the development of a UTI with ESBL-producing E. coli within 30 days after completion of amikacin treatment.
Because of the potential nephrotoxicity associated with aminoglycosides use, renal function as determined by serum creatinine levels was measured before the administration of amikacin and at the end of treatment, as recommended in the product informationCitation12 and by the Infectious Diseases Society of America (IDSA) guidelines.Citation13 Nephrotoxicity was defined as doubling of baseline serum creatinine compared with treatment initiation and/or elevation of serum creatinine values beyond the estimated normal range for the patient’s age group.Citation14,Citation15 Ototoxicity was defined as any symptoms or signs of the following after amikacin use: nausea, vomiting, nystagmus, ataxia, dizziness, vertigo, tinnitus or hearing loss.Citation16 Monitoring of ototoxicity was made by the subjective patient assessment at outpatient clinic visits.
Ethics statement
The Ethical Committee of Erzurum Research and Training Hospital approved this study (approval number: 2017/04-31) with a waiver of informed consent for retrospective data collection under the condition of anonymously stored data collected.
Statistical analysis
Data were analyzed by frequency and percentage for qualitative variables, and mean ± SD, median, minimum, and maximum values for quantitative variables.
A paired t-test was carried out to assess whether there was a significant difference between the mean serum creatinine values that were obtained before and after the administration of amikacin. Statistical analyses were performed using SPSS 21 (IBM SPSS Inc, Chicago, IL, USA) and the significance was set at p<0.05.
Results
A total of 53 eligible patients (38 females) were enrolled in this study. The median age of the patients was 4.7 years (range 3–12 years). Of the 53 patients, 16 (30%) had a previous history of culture-positive UTI. Most of the patients (n=48, 90%) had received antibiotics in the last 3 months, including second- and third-generation cephalosporins (n=18), amoxicillin–clavulanate (n=17), and TMP-SMX (n=13), for either presumptive diagnosis of UTI without prior urine studies or treatment of other infections. Prophylactic antibiotic use was recorded in 16 of 53 (30%) patients for recurrent UTI: TMP-SMX in 8 patients, nitrofurantoin in 5 patients, and cephalexin in 3 patients. According to in vitro susceptibility test results, 18 of 53 (34%) patients received inappropriate empiric therapy that did not provide clinical improvement, including oral formulations of third-generation cephalosporin (n=11), amoxicillin–clavulanate (n=4), and TMP-SMX (n=3). The remaining 35 (66%) patients who did not receive empiric antimicrobial therapy, were initially seen in other outpatient clinics and consulted us with positive urine culture results for antibiotic treatment recommendation.
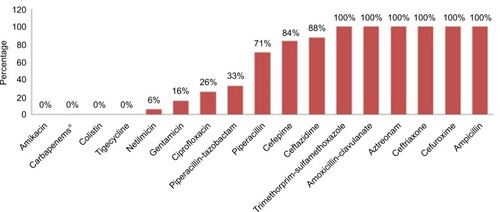
Amikacin was initiated as definitive treatment (after urine culture susceptibility results were made available) in all of the patients. All E. coli isolates were susceptible to amikacin with MICs of ≤4 mg/L but resistant to amoxicillin–clavulanate (MICs >32/2 mg/L) and TMP-SMX (MICs >4/76 mg/L) (). The median duration of amikacin treatment was 6 days (range 3–7 days). Treatment outcomes and adverse events of amikacin treatment are summarized in . Poor clinical and bacteriological responses were seen in only 1 patient who subsequently developed acute pyelonephritis and was hospitalized 3 days after the initiation of amikacin. Treatment was changed to intravenous ertapenem (15 mg/kg/dose twice daily). On hospital day 3, ESBL-producing E. coli that was resistant to amikacin (MIC >16 mg/L) but susceptible to ertapenem (MIC ≤0.25 mg/L) was isolated from urine and blood cultures. The patient was discharged in good condition on hospital day 10. No treatment changes were required for resolution of symptoms in all other patients. Relapsed lower UTI after initial treatment response was seen in another 12-year-old female patient 2 weeks after treatment completion. ESBL-producing E. coli susceptible to both amikacin (MIC ≤4 mg/L) and nitrofurantoin (MIC ≤16 mg/L) was isolated again from urine culture, and the patient was successfully treated with a 7-day course of nitrofurantoin (7 mg/kg/day orally in 4 divided doses). In this patient, we could not find any underlying functional or anatomic urinary tract abnormalities for the development of relapsed UTI, except for bladder and bowel dysfunction.
Table 1 Treatment outcomes and adverse events of outpatient amikacin therapy (n=53)
Figure 1 The antimicrobial resistance profiles of extended-spectrum β-lactamase-producing Escherichia coli isolates (n=53).
Note: *Carbapenems: meropenem, imipenem and ertapenem included.
There was no significant nephrotoxicity in any of the patients. All patients had normal serum creatinine values at baseline (median 0.4 mg/dL, range: 0.2–0.5 mg/dL), and differences between the mean serum creatinine levels before the initiation and at the end of amikacin treatment were not statistically significant (0.45±0.11 mg/dL vs 0.47±0.13 mg/dL, p=0.24). There were no subjective changes in hearing, tinnitus, and clinically apparent vestibular dysfunction in any of the patients.
Discussion
Given the limited treatment options available outside the hospital setting, management of UTI due to ESBL-producing E. coli is challenging in children. When choosing a treatment regimen, physicians should consider such factors as the local susceptibility pattern, adverse effects, cost effectiveness, and selection of resistant strains.Citation4,Citation5 In recent years, aminoglycosides are undergoing a resurgence in use because of widespread resistance to other therapeutic classes.Citation17 The results of the Study for Monitoring Antimicrobial Resistance Trends surveillance studies from different parts of the world indicate that amikacin maintains a high level of in vitro activity against ESBL-producing strains.Citation9,Citation18 However, clinical data for the use of amikacin for the treatment of UTIs due to ESBL-producing E coli are limited in children. Only 2 adult studies have reported the use of amikacin for outpatient treatment of UTIs caused by ESBL-producing strains.Citation19,Citation20 To the best of our knowledge, this is the largest and the first pediatric cohort to date that examines the clinical and microbiological outcomes of community-acquired lower UTIs due to ESBL-producing E. coli treated with outpatient amikacin.
Our study suggests that once-daily intramuscular amikacin could be an alternative option for outpatient treatment of children with community-acquired lower UTIs caused by amikacin-susceptible ESBL-producing E. coli strains. These findings are in agreement with those of previous adult studies.Citation19,Citation20 Park et alCitation21 reported on the clinical and microbiological effects of aminoglycosides in adults and children with UTIs caused by ESBL-producing strains, and the efficacy of aminoglycoside combination therapy has also been demonstrated in children with febrile UTIs due to ESBL-producing strains.Citation22
Based on identification and susceptibility results, alternatives to carbapenems should be used to treat uncomplicated UTIs caused by ESBL-producing organisms. The antimicrobial agents most commonly used to treat uncomplicated UTIs include the β-lactams, TMP–SMX, fluoroquinolones, fosfomycin, and nitrofurantoin.Citation4,Citation5 However, ESBL- producing E. coli strains are frequently resistant to commonly prescribed oral antibiotics such as TMP-SMX, penicillins, and cephalosporins.Citation23 This condition poses significant therapeutic challenges in children, in whom fewer antibiotics are approved for clinical use.Citation5 The high rates of TMP-SMX and amoxicillin–clavulanate resistance observed in our study are thought to be related to the excessive usage of these 2 antibiotics for the prophylaxis or treatment of UTIs and other common pediatric infections. Additionally, all of the patients in our study were aged ≤12 years, which limits the use of fluoroquinolones and fosfomycin. Fluoroquinolones are not recommended for routine use in children <18 years of age because of the osteoarticular side effects observed in juvenile animals. Indications for fluoroquinolone use in patients <18 years, as stated by the US Food and Drug Administration, include treatment of complicated UTIs and pyelonephritis due to E. coli.Citation24 Fosfomycin is an oral antimicrobial agent that has broad activity against multi-drug resistant pathogens, including ESBL-producing E. coli.Citation25 However, pediatric experience with fosfomycin is limited, since its safety and effectiveness in children aged ≤12 years have not been established.Citation26 Nitrofurantoin is another potential treatment option for lower UTI caused by ESBL-producing E. coli, if the isolate is known to be susceptible.Citation4,Citation5 However, during the study period, the susceptibility testings for nitrofurantoin and fosfomycin were not routinely performed by our microbiology laboratory, unless requested by the treating physician. Therefore, as in our patients, amikacin could be an alternative option for the outpatient treatment of lower UTIs caused by ESBL-producing E. coli, if there is no suitable oral antibiotic therapy. To prevent the development of resistance, carbapenems should only be used in patients with severe infections with ESBL-producing Enterobacteriaceae other than UTIs.
Amikacin monotherapy seems to be a useful alternative for the outpatient treatment of children with uncomplicated ESBL UTIs because of its high urinary excretion (aminoglycosides reach concentrations in the urine 25–100-fold that of serum), low resistance rates, easy intramuscular administration, and low cost.Citation5,Citation8,Citation16 Certain pharmacodynamic and kinetic properties of the aminoglycosides are important for their clinical application.Citation27 Aminoglycosides demonstrate both concentration-dependent killing and post-antibiotic effect that allow a once-daily administration schedule. A once-daily schedule produces longer post-antibiotic effect, significantly higher peak concentration and greater bactericidal activity. Compared with multiple-daily dosing, once-daily dosing causes similar or lower rates of nephrotoxicity.Citation8,Citation16
The main concerns with the use of aminoglycoside antibiotics are nephrotoxicity and ototoxicity. The risk of nephro- and ototoxicity is greater in patients with impaired renal function, and in patients with normal renal function treated at higher doses and/or for periods longer than those recommended.Citation12,Citation27 Aminoglycoside-induced ototoxicity may result in either vestibular or cochlear damage. Cochlear damage is manifested as tinnitus or high frequency hearing loss, whereas vestibular damage is associated with vertigo, nausea, vomiting, nystagmus, and ataxia.Citation16 Monitoring for ototoxicity involves subjective patient assessment for the presence of hearing and vestibular dysfunction.Citation13 The use of objective testing such as audiometry is generally reserved for patients who have subjective symptoms, pre-existing hearing dysfunction, and for those scheduled to receive prolonged therapy.Citation12,Citation13 In this study, although we did not routinely perform pre- and post-treatment audiometry, clinically detectable ototoxicity was not observed. There were no significant changes in serum creatinine levels. To prevent the development of nephro- and ototoxicity, we administered amikacin at the recommended doseCitation10,Citation12 and durationCitation12,Citation27 in patients with normal renal function. Current recommendations for once-daily dosing of all aminoglycosides are for only up to 5–6 days.Citation27 In the present study, amikacin was given in a total daily dose of 15 mg/kg and the treatment duration was median 6 days, and did not exceed 7 days. The duration of antibiotic treatment for afebrile children with presumed lower UTI has been controversial; however, 3 days of TMP-SMX or 5 days of other antibiotics is thought to be effective.Citation4 In our clinic, we usually treat children aged ≥2 years with uncomplicated lower UTI for at least 5 days.
In our outpatient clinic, there is only 1 follow-up visit for children with uncomplicated lower UTI and we do not routinely perform control urine culture if the patient responds well to antibiotic therapy. However, in the present study, control urine cultures were obtained in all children to ensure the bacteriological efficacy of amikacin against ESBL-producing E. coli isolates. In patients receiving aminoglycoside therapy, clinical monitoring for vestibular and hearing dysfunction at each visit and monitoring of serum creatinine levels at least twice a week are recommended by guidelines issued by the IDSA for the treatment of outpatient parenteral antimicrobial therapy (OPAT).Citation13 It was also recommended that patients should be seen after completion of OPAT to be sure they have responded to therapy, are doing well and have had no adverse events.Citation13 We therefore arranged the follow-up visits on the third day of and at the end of the treatment to monitor the efficacy and toxicity outcomes.
Although the prevalence of aminoglycoside resistance has remained relatively low compared with that for cephalosporins or fluoroquinolones, some investigators reported increased amikacin resistance following unrestricted use of this antibiotic.Citation28 One review of a large number of clinical trials found that development of resistance in Gram-negative bacteria during treatment with aminoglycosides resulted in treatment failure in 85% of the cases,Citation29 as in our 1 case who failed to respond to amikacin treatment due to development of resistance. The judicious use of existing antimicrobials to preserve their future effectiveness and the future development of novel agents effective against ESBL-producing strains in children will help expand the therapeutic repertoire available to pediatricians to treat resistant Gram-negative infections.
This study has the following limitations. First, this is single-center, retrospective study with a relatively small number of patients, and thus, cannot allow generalization of clinical and microbiological outcomes and adverse events. Second, ototoxicity was estimated only subjectively and routine audiometry was not performed. Third, there was no control group to compare the efficacy of amikacin versus other antimicrobials.
Despite these limitations, this is the first pediatric study that gives important data on whether the use of amikacin could be an alternative option for outpatient treatment of lower UTIs caused by ESBL-producing E. coli in areas where antibiotic resistance rate of the urinary pathogens is high.
Conclusion
The results of our study suggest that pediatric patients with community-acquired lower UTIs caused by amikacin-susceptible ESBL-producing E. coli, with no suitable oral antibiotic therapy, can be treated as outpatients with once-daily intramuscular amikacin, if patients are closely monitored for renal function and ototoxicity. Further randomized controlled studies, including a large number of cases are needed to exactly define the effectiveness and safety of once-daily dosing of amikacin in pediatric patients with UTIs due to ESBL-producing E. coli.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
- FanNCChenHHChenCLRise of community-onset urinary tract infection caused by extended-spectrum beta-lactamase-producing Escherichia coli in childrenJ Microbiol Immunol Infect201447539940523834784
- DayanNDabbahHWeissmanIAgaIEvenLGlikmanDUrinary tract infections caused by community-acquired extended-spectrum b-lactamase-producing and nonproducing bacteria: a comparative studyJ Pediatr201316351417142123919903
- MeggedOExtended spectrum b-lactamase-producing bacteria causing community acquired urinary tract infections in childrenPediatr Nephrol20142991583158724705795
- RobinsonJLLe SauxNManagement of urinary tract infections in children in an era of increasing antimicrobial resistanceExpert Rev Anti Infect Ther201614980981627348347
- HsuAJTammaPDTreatment of multidrug-resistant Gram-negative infections in childrenClin Infect Dis201458101439144824501388
- PitoutJDLauplandKBExtended-spectrum beta-lactamase-producing Enterobacteriaceae: an emerging public-health concernLancet Infect Dis20088315916618291338
- CantónRAkóvaMCarmeliYEuropean Network on CarbapenemasesRapid evolution and spread of carbapenemases among Enterobacteriaceae in EuropeClin Microbiol Infect201218541343122507109
- Contopoulos-IoannidisDGGiotisNDBaliatsaDVIoannidisJPExtended-interval aminoglycoside administration for children: a meta-analysisPediatrics20041141111118
- BouchillonSKBadalREHobanDJHawserSPAntimicrobial susceptibility of inpatient urinary tract isolates of gram-negative bacilli in the United States: results from the study for monitoring antimicrobial resistance trends (SMART) program: 2009–2011Clin Ther201335687287723623624
- American Academy of PediatricsAntimicrobial agents and related therapyKimberlinDWBradyMTJacksonMALongSSRed Book: 2015 Report of the Committee on Infectious Diseases30th edElk Grove Village, ILAmerican Academy of Pediatrics2015884
- The European Committee on Antimicrobial Susceptibility TestingBreakpoint tables for interpretation of MICs and zone diameters. Version 5.02015 Available from: http://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Breakpoint_tables/v_5.0_Breakpoint_Table_01.pdfAccessed April 18, 2017
- Amikacin: summary of product characteristicsEuropean Medicines Agency Available from: http://www.medicines.org.uk/emc/medicine/22773/SPC/AMIKIN+INJECTION+100MG+2MLAccessed April 18, 2017
- TiceADRehmSJDalovisioJRIDSAPractice guidelines for outpatient parenteral antimicrobial therapy. IDSA guidelinesClin Infect Dis200438121651167215227610
- SavoryDJReference ranges for serum creatinine in infants, children and adolescentsAnn Clin Biochem199027Pt 2991012327712
- KarbuzAÖzdemirHYamanAThe use of colistin in critically ill children in a pediatric intensive care unitPediatr Infect Dis J2014331e19e2424346607
- KrausDMPaiMPRodvoldKAEfficacy and tolerability of extended-interval aminoglycoside administration in pediatric patientsPaediatr Drugs20024746948412083974
- DrusanoGLAmbrosePGBhavnaniSMBertinoJSNafzigerANLouieABack to the future: using aminoglycosides again and how to dose them optimallyClin Infect Dis200745675376017712761
- LuPLLiuYCTohHSEpidemiology and antimicrobial susceptibility profiles of Gram-negative bacteria causing urinary tract infections in the Asia-Pacific region: 2009–2010 results from the Study for Monitoring Antimicrobial Resistance Trends (SMART)Int J Antimicrob Agents201240S37S4322749057
- IpekciTSeymanDBerkHCelikOClinical and bacteriological efficacy of amikacin in the treatment of lower urinary tract infection caused by extended-spectrum beta-lactamase-producing Escherichia coli or Klebsiella pneumoniaeJ Infect Chemother2014201276276725179392
- ChoSYChoiSMParkSHLeeDGChoiJHYooJHAmikacin therapy for urinary tract infections caused by extended-spectrum β-lactamase-producing Escherichia coliKorean J Intern Med201631115616126767869
- ParkSHChoiSMChangYKThe efficacy of non-carbapenem antibiotics for the treatment of community-onset acute pyelonephritis due to extended-spectrum β-lactamase-producing Escherichia coliJ Antimicrob Chemother201469102848285624928854
- HanSBLeeSCLeeSYJeongDCKangJHAminoglycoside therapy for childhood urinary tract infection due to extended-spectrum β-lactamase-producing Escherichia coli or Klebsiella pneumoniaeBMC Infect Dis20151541426464143
- PrakashVLewisJS2ndHerreraMLWickesBLJorgensenJHOral and parenteral therapeutic options for outpatient urinary infections caused by Enterobacteriaceae producing CTX-M extended-spectrum beta-lactamasesAntimicrob Agents Chemother20095331278128019124661
- American Academy of Pediatrics, Committee on Infectious DiseasesThe use of systemic and topical fluoroquinolonesPediatrics2011128410341045
- FalagasMEKastorisACKapaskelisAMKarageorgopoulosDEFosfomycin for the treatment of multi-drug resistant, including extended spectrum b-lactamase-producing, Enterobacteriaceae infections: a systematic reviewLancet Infect Dis2010101435020129148
- Monurol (fosfomycin tromethamine) oral suspension – FDA Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2011/050717s007lbl.pdfAccessed July 7, 2017
- CraigWAOptimizing aminoglycoside useCrit Care Clin201127110712121144989
- HarbarthSRohnerPSafranEGarbinoJAuckenthalerRPittetDResistance to amikacin and gentamicin among Gram-negative bloodstream isolates in a university hospital between 1989 and 1994Clin Microbiol Infect19984419920411864326
- MilatovicDBravenyIDevelopment of resistance during antibiotic therapyEur J Clin Microbiol1987632342443305004