
Abstract
Background
Clinicians use sputum culture conversion as an interim indicator of the efficacy of multi-drug resistant tuberculosis (MDR-TB) treatment and to determine treatment duration. Yet, limited studies have been published in Ethiopia.
Objective
The objective of this study was to determine the predictors of delayed culture conversion among patients receiving MDR-TB treatment at selected treatment centers in Ethiopia.
Patients and Methods
A multi-center observation study was conducted among MDR-TB patients in South and Southwestern Ethiopia from April 14 to May 14, 2019. The data of patients treated from January 2013 to July 2019 were reviewed using a data abstraction tool. The data were analyzed. Descriptive statistics was computed using SPSS version 21 software program. Cox regression was used to identify predictors of delayed culture conversion. Hazard ratios with a two-sided p-value <0.05 were considered statistically significant.
Results
Of 200 included MDR-TB patients, 108 (54%) were males. Majority,159 (79.5%) of the patients had a culture conversion time of less than two months, while 15 (7.5%) had delayed culture conversion (greater than 120 days). Patient’s registration group (after loss to follow- (adjusted hazard ratio (AHR)=16.215, 95% CI [3.839, 68.498]), after treatment failure (AHR=12.161, 95% CI [2.516, 58.793]), history of previous TB treatment (AHR=4.007, 95% CI [3.115, 62.990])) and low BMI (AHR= 1.257; 95% CI [0.725,1.547] were identified as a risk factors for delayed culture conversion.
Conclusion
Our finding showed that nearly 80% of the patients achieve sputum culture conversion by the second month of treatment. Delayed culture conversion was more likely among patients with malnutrition (BMI<18.5kg/m2), after treatment failure, previous TB treatment, and after lost to follow-up.
Introduction
Tuberculosis (TB) is the commonest infectious disease that is responsible for the death of approximately 2 million people every year, globally.Citation1 Although tremendous efforts have been made to control it, an alarmingly increasing Multi-drug resistant tuberculosis (MDR-TB) hampers the prevention and control of TB.Citation2 The global TB report showed that in 2018, there were 3.4% new cases and 18% previously treated cases of MDR-TB. Countries with the largest share of the global TB burden include the Republic of India, China, and the Russian Federation. In Africa, Nigeria and South Africa harbour the largest number of MDR-TB cases. With 2700 MDR-TB cases each year, Ethiopia is among the top 30 MDR-TB burden countries. A recent data in the country reported the prevalence of MDR-TB to be 0.71% and 16% among newly diagnosed and under retreatment, respectively.Citation3
The status of mycobacterial cultures plays an important role in guiding the treatment of MDR-TB and is an interim indicator of the efficacy of the treatment.Citation4,Citation5 Delayed/non-conversion of sputum culture after the end of 4 months of intensive phase treatment often suggests unfavorable outcomes, ie, treatment failure and death.Citation6,Citation7 Furthermore, prolonged sputum culture conversion has a negative impact on the economy, mainly through extending the period of therapy, sub-optimal adherence to treatment with consequent treatment failure.Citation6 Baseline radiological findings (lung cavitation), high bacillary load, resistance to ofloxacin (Ofx) or streptomycin, malnutrition, HIV co-infection, and therapeutic delay of greater than one month have been linked to a delay in sputum culture conversion in prior studies.Citation6,Citation8,Citation9
Despite the substantial use of sputum culture conversion as an interim indicator of treatment efficacy, limited studies have been conducted in Ethiopia. Hence, this multicenter observational study was designed to determine predictors of delayed sputum culture conversion among patients treated for MDR-TB at three treatment centers in Ethiopia.
Patients and Methods
Study Design and Study Area
A multi-center observational study was done among patients treated for MDR-TB at three treatment centers (Arbaminch, Butajira, and Shenengibe General Hospitals) located in South and Southwestern Ethiopia. The study was conducted from April 14 to May 14, 2019.
Arbaminch and Butajira General Hospitals are located in Southern Ethiopia, and they are currently serving around 11 million population. The former started its MDR-TB treatment service in 2014, while the latter started in 2015. Currently, there are 110 MDR-TB patients registered in both hospitals. Shenengibe Hospital is found in Southwestern Ethiopia, Jimma zone, and it’s 329Km away from the capital, Addis Ababa. It’s currently serving about 5 million population. The hospital started it’s service in 2013. So far, 98 MDR-TB patients were enrolled in the center.
Study Participants
We included all adult patients with confirmed diagnosis of MDR-TB (those with isoniazid and rifampicin resistance, but with or without resistance to other first-line drugs) based onXpert MTB/RIF® assay whose charts fulfilled the eligibility criteria (containing complete baseline and follow-up data) in the aforementioned treatment centers.Citation10 There is no special sampling technique employed. We excluded charts of patients with incomplete data on the outcome variables, and patients transferred to other treatment centers. Finally, 200 patients were included in the final analysis.
Data Collection
A structured checklist prepared from different literatures, WHO guidelines, and national MDR-TB treatment follow-up charts was used to collect the necessary data. The checklist contains several variables.Citation9–Citation12 The variables inlude Patient-related variables (gender, age, residence, pregnancy, marital status, smoking status, educational level, and body mass index (BMI)); Disease-related variables (category of MDR-TB, drug resistance status, and comorbidities); Drug-related data (type of medication, and drug regimen). The dependent variable was time to sputum culture conversion.
Definition of Terms
Sputum culture conversion was defined as a two sets of negative consecutive cultures taken at least 30 days apart after initiation of treatment. Delayed culture conversion was defined as a culture conversion time greater than 120 days. Previously treated: A patient who has a history of previous treatment for TB (four weeks or more), and is now diagnosed with recurrent TB. Treatment after failure: A patient whose treatment was failed at the end of the most recent treatment episode. Treatment after loss to follow up: A patient who has previous history of treatment for >1 month and returns to treatment following interruption of treatment for ≥2 consecutive months with positive test by GeneXpert MTB/RIF TB/RIF, culture or sputum smear microscopy. New/previously not treated for TB was defined as a patient who had no prior anti-TB treatment. Adherence was explained as the extent to which a patient continues the agreed upon medication as prescribed (Good Adherence: for adherence rate of >95%, Fair Adherence: adherence rate of 85–94% and Poor Adherence for <85% adherence level).
Data Quality
The questionnaire was carefully prepared to collect all important data in order to achieve the aim of the study. The appropriateness of each patient chart was reviewed for inclusion before data collection. Two pharmacists and physicians were recruited for data collection. The pharmacists were responsible for collecting drug-related data, while the patient-related clinical variables were collected by the physicians. At each treatment center, an infectious disease specialist supervised the data collection process. Supervisors followed the data collection process and helped by correlating diagnostic, and laboratory findings with the main outcome. Furthermore, a pretest was done on 5% (10) of patients’ charts to detect the effectiveness of the data collection tool. Based on the pretest finding, all necessary adjustment was made.
Data Analysis
Data were entered and cleaned in EpiData (v.4.2) and exported to SPSS software package (v.21) for statistical analysis. For categorical variables, proportions were computed and summarized as counts, graphs, and percentages. Pearson’s chi-square (χ2) was used to compare the baseline characteristics of the patients. For normally distributed variables, mean and standard deviation (SD) were used to summarize, while median and interquartile range (IQR) was utilized to report non-normally distributed variables. The Kaplan–Meier estimation was performed to compute the baseline survival experience of the patients. A bivariate Cox proportional hazard model was first fitted, and variables with p-value <0.25 in the bivariate analysis were further regressed using multivariable Cox proportional-hazard model. On multivariable Cox proportional-hazard regression model, variables with a p-value <0.05 were considered to declare statistical significance.
Results
Overview of the Included Patients
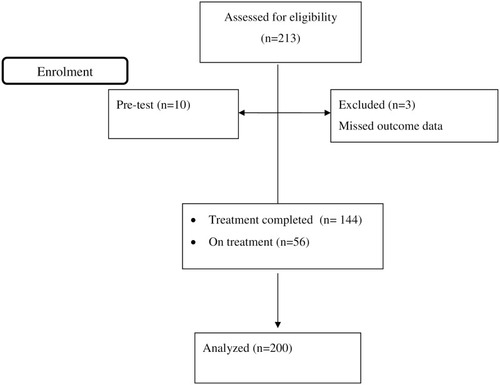
During the study period, 213 patient charts were reviewed for eligibility and 13 records were excluded. Finally, a total of 200 MDR-TB patients were included in the analysis ().
Figure 1 Flow chart for recruitment of patients treated for MDR-TB treatment, April 14 to May 14, 2019.
Socio-Demographic Characteristics
The mean ± SD age of the patients was 32.9±9.5years. More than half, 108(54%) of the patients were male and 111(55.5%) were rural dwellers, and 99(49.5%) of the patients were married. The highest proportion, 37%, have a secondary level of education ().
Table 1 Socio-Demographic Characteristics of the Patients Stratified by the Status of Delayed Culture Conversion Time from April 14 to May 14, 2019
Clinical Characteristics
Of the 200 patients, 156 (78%) were previously treated, 22 (11%) were new MDR-TB cases, 9 (4.5%) were lost to follow-up, 13 (6.5%) had treatment after failure. About 56 (28%) of the study participants were living with various comorbidities. The commonest comorbidities diagnosed were diabetes mellitus (DM), 9(4.5%), and renal problem, 7(3.5%), respectively. Most, 196 (98%) of the patients received vitamin B6 supplementation, and 173 (86.5%) had good adherence ().
Table 2 Clinical Characteristics of the Patients Stratified by Delayed Culture Conversion Time from April 14 to May 14, 2019
Time to Sputum Culture Conversion
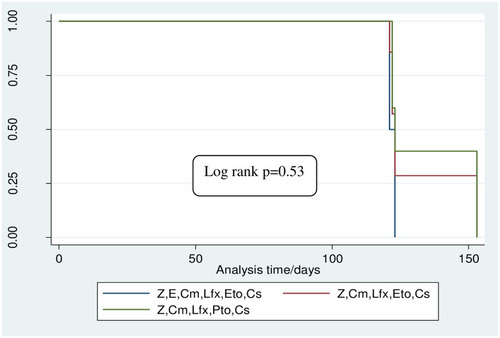
Majority,159 (79.5%) of the patients had a culture conversion time of less than two months, while 15 (7.5%) had delayed culture conversion (greater than 120 days). All patients had converted before 6-months. The median time to culture conversion was 31 (IQR: 30–61) days. There was no statistically significant difference in terms of culture conversion among the regimens (Log rank p=0.53) ().
Figure 2 Survival estimates of delayed culture conversion among MDR-TB treated patients January, 2013 to May, 2019.
Predictors of Delayed Sputum Culture Conversion
A Cox proportional-hazard regression analysis was performed to identify predictors of delayed culture conversion. On bivariate analysis, the presence of comorbidity, adherence status, HIV status, BMI, and patient’s registration group were significantly associated with delayed culture conversion. On multivariate cox-regression, patient’s registration group and BMI remained independent predictors of delayed culture conversion. Consequently, patients registered after loss to follow-up had 16 times higher hazard of delayed culture conversion (AHR=16.215, 95% CI [3.839, 68.498]). Similarly, patients who were registered after treatment failure had 12 times higher hazard of delayed culture conversion (AHR=12.161, 95% CI [2.516, 58.793]). Patients who had history of previous treatment also had 4 times higher hazard of delayed culture conversion (AHR=4.007, 95% CI [3.115, 62.990]). Moreover, the hazard of delayed culture conversion among underweight (BMI <18.5kg/m2) patients was 1.26 (AHR=1.257,95% CI [1.125, 1.547]) ().
Table 3 Crude and Adjusted Cox-Proportional Hazard Regression for Predictors of Delayed Culture Conversion of the Cohort, from April 14 to May 14, 2019
Discussion
In this study, time to sputum culture conversion and predictors of delayed sputum culture conversion were examined. Majority,159 (79.5%) of the patients had a culture conversion time of less than two months, while 15 (7.5%) had delayed culture conversion (>120 days). Patient’s registration group and BMI were independently associated with delayed culture conversion.
In the present study, 79.5% of patients had sputum culture converted at 2 months. This finding highlights an effective treatment of the patients with adequate regimens at the right dose, making the patient noninfectious rapidly, which ultimately results in favourable outcomes. Comparable findings have been reported in LatviaCitation13 and India,Citation14 in which 79% and 82% of patients had converted at 2 months, respectively. In contrary, our findings revealed a faster culture conversion in comparison with studies conducted by Kurbatova et alCitation6, and Rodriguez et al.Citation15 The variation could be attributed to the difference in sample size and the way time to culture conversion was defined. In this study, time to culture conversion was defined as two consecutive negative culture results, while it was defined by five consecutive negative culture results in the study by Kurbatova et al.Citation6
We found that MDR-TB patients with history of previous TB treatment had 4 times higher hazard of delayed culture conversion (AHR=4.007, 95% CI [3.115, 62.990]). This finding was in accordance with a study conducted in India, where patients with history of previous TB treatment had two times higher hazard of delayed culture conversion than new MDR-TB patients.Citation16
Similarly, patients registered after loss to follow-up (AHR=16.215, 95% CI [3.839, 68.498]), and after treatment failure (AHR=12.161, 95% CI [2.516, 58.793]) also had higher hazard of delayed culture conversion. Similar finding was reported from a multicenter study conducted in Peru, Latvia, Estonia, Russia, and Philippines by Kurbatova et al.Citation6
Moreover, MDR-TB patients with low body mass index (BMI <18.5kg/m2) had higher hazard of delayed culture conversion than their counterparts (AHR=1.257, 95% CI [1.125, 1.547]). This finding was in line with several studies conducted elsewhere that reported low BMI as a predictor of delayed culture conversion.Citation17–Citation19 Low BMI is an indicator of poor nutritional status; under nutrition. Under nutrition; an indicator of severe disease and poor socio-economic status, impairs host immunity against mycobacteria. The accompanying impairment in host immunity may increase susceptibility to various infectious diseases.Citation20 A study by Scrimshaw et alCitation21 particularly revealed that under nutrition (BMI <18.5kg/m2) reduced the concentrations of immunoglobulins, interleukin-2 receptors, and T-cell subsets (suppressor-cytotoxic, helper, and natural killer cells) among TB patients. This finding suggests that undernourished MDR-TB patients may remain infectious in the community for a long period.
Conclusion
In conclusion, our finding shows that nearly 80% of MDR-TB patients achieve sputum culture conversion by the second month of treatment. Delayed cultured conversion was more likely in those with malnutrition (BMI <18.5kg/m2), after treatment failure, previous TB treatment, and loss to follow-up.
Limitations of the Study
This study suffers from several limitations. Firstly, the retrospective nature of the data source limited us from capturing full information about the patients. Secondly, some important diagnostic and laboratory data were missed due to lack of sufficient registration. Hence, most of the patients have no data on sputum smear microscopy results. Thirdly, the method of patients’ adherence assessment was also subjective as it is based on patient reports. Lastly, although his was a multi-center survey, the number of hospitals included in the study was not sufficient to fully capture the data in Ethiopia.
Abbreviations
BMI, body mass index; Cm, capreomycin; E, ethambutol; Eto, ethionamide; MDR-TB, multidrug resistance tuberculosis; PZA, pyrazinamide; R, rifampici.
Data Sharing Statement
There are no material outputs from this study, and all data are those presented in the manuscript.
Ethical Approval
The study approved by the Ethical Review Board of Jimma University and given an IRB number of IHRPG1/565/2019. Because of the retrospective anonymous nature of the study, the need for informed consent was waived. Confidentiality was ensured by removing the name and address of the patients from the data. This study was conducted in accordance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. All authors have read and approved the manuscript.
Acknowledgments
The authors thank the data collectors and all staff members of the study settings for their valuable contribution. We also would like to thank Jimma University for providing this opportunity to conduct this research.
Disclosure
The authors declare no conflicts of interest for this work.
References
- World Health Organization. Global tuberculosis report. Geneva: World Health Organization. 2019; Available from: https://www.who.int/tb/publications/global_report/en/. Accessed 413, 2021.
- Ormerod LP. Multidrug-resistant tuberculosis (MDR-TB): epidemiology, prevention and treatment. Br Med Bull. 2005;73–74(1):17–24. doi:10.1093/bmb/ldh047
- Ismail N, Ismail F, Omar SV, et al. Drug resistant tuberculosis in Africa: current status, gaps and opportunities. 2016;7(2):1–11. Afr J Lab Med. 2018;7(2):1–11. doi:10.4102/ajlm.v7i2.781
- Laserson KF, Thorpe LE, Leimane V, et al. Speaking the same language: treatment outcome definitions for multi drug-resistant tuberculosis. Int J Tuberc Lung Dis. 2005;9(6):640–645.15971391
- World Health Organization. Guidelines for establishing DOTS-plus pilot projects for the management of Multidrug-Resistant Tuberculosis (MDR-TB). WHO/CDS/TB/2000.279. Geneva: World Health Organization; 2000
- Kurbatova E, Gammino V, Bayona J, et al. Predictors of sputum culture conversion among patients treated for multidrug-resistant tuberculosis. Int J Tuberc Lung Dis. 2012;6(10):1335–1343. doi:10.5588/ijtld.11.0811
- Kurbatova EV, Cegielski JP, Lienhardt C, et al. Sputum culture conversion as a prognostic marker for end-of-treatment outcome in patients with multidrug-resistant tuberculosis: a secondary analysis of data from two observational cohort studies. Lancet Respir Med. 2015;3(3):201–209. doi:10.1016/S2213-2600(15)00036-325726085
- Basit A, Ahmad N, Khan AH, et al. Predictors of two months culture conversion in multidrug-resistant tuberculosis: findings from a retrospective cohort study. PLoS One. 2014;9(4):e93206. doi:10.1371/journal.pone.009320624705411
- Putri FA, Burhan E, Nawas A, et al. Body mass index predictive of sputum culture conversion among MDR-TB patients in Indonesia. Int J Tuberc Lung Dis. 2014;18(5):564–570. doi:10.5588/ijtld.13.060224903794
- Alene K, Viney K, Mcbryde S, Tsegaye A. Treatment outcomes in patients with multidrug-resistant tuberculosis in Treatment outcomes in patients with multidrug-resistant tuberculosis in north-west Ethiopia. Trop Dis Med Vaccine. 2017;22(3):351–362.
- Caminero JA Guidelines for clinical and operational management of drug-resistant tuberculosis; 2013.
- Caminero JA. State of the ART multidrug-resistant tuberculosis: epidemiology, risk factors, and case finding. Int J Tuberc Lung Dis. 2010;14(4):382–390.20202293
- Holtz TH, Sternberg M, Kammerer S, et al. Time to sputum culture conversion in multidrug-resistant tuberculosis: predictors and relationship to treatment outcome. Ann Intern Med. 2006;144(9):650–659. doi:10.7326/0003-4819-144-9-200605020-0000816670134
- Joseph P, Desai VB, Mohan NS, et al. Outcome of standardized treatment for patients with MDR-TB from Tamil Nadu, India. Indian J Med Res. 2011;133(5):529–534.21623039
- Rodriguez M, Monedero I, Caminero JA, et al. Successful management of multidrug-resistant tuberculosis under programme conditions in the Dominican Republic. Int J Tuberc Lung Dis. 2013;17(4):520–525. doi:10.5588/ijtld.12.048123485386
- Katiyar SK, Bihari S, Prakash S, Mamtani M, Kulkarni H. A randomised controlled trial of high-dose isoniazid adjuvant therapy for multidrug-resistant tuberculosis. Int J Tuberc Lung Dis. 2008;12(2):139–145.18230245
- Park HO, Kim SH, Moon SH, et al. Association between body mass index and sputum culture conversion among South Korean patients with multidrug resistant tuberculosis in a tuberculosis referral hospital. Infect Chemother. 2016;48(4):317–323. doi:10.3947/ic.2016.48.4.31727883374
- Velayutham B, Nair D, Kannan T, et al. Factors associated with sputum culture conversion in multidrug-resistant pulmonary tuberculosis. Int J Tuberc Lung Dis. 2016;20(12):1671–1676. doi:10.5588/ijtld.16.009627931345
- Magee MJ, Kempker RR, Kipiani M, et al. Diabetes mellitus, smoking status, and rate of sputum culture conversion in patients with multidrug-resistant tuberculosis: a cohort study from the country of Georgia. PLoS One. 2014;9(4):e94890. doi:10.1371/journal.pone.009489024736471
- Lee YM, Kim SM, Park SJ. Factors associated with a strong response to the T-SPOT. TB in patients with extrapulmonary tuberculosis. Infect Chemother. 2014;46(4):248–252. doi:10.3947/ic.2014.46.4.24825566404
- Scrimshaw NS, SanGiovanni JP. Synergism of nutrition, infection, and immunity: an overview. Am J Clin Nutr. 1997;66(2):464S–477S. doi:10.1093/ajcn/66.2.464S9250134