
Abstract
Since the emergence of COVID 19, the authentic SARS-CoV-2 has evolved into a range of novel variants that are of more global concern. In late November 2021, the Omicron (lineage B.1.1.529) variant was identified as a new variant and considered as the fifth variant of concern. Omicron harbors a genetic profile that is exceedingly unusual, with a huge number of mutations. Above thirty mutations are localized in the S protein, while some are found in other structural and non-structural proteins. Half of the mutations in the S protein are in the RBD, which is a major target of antibodies, showing that Omicron mutations may affect antibody binding affinity to the S protein. The Omicron variant has been found to result in immune escape, therapeutic or vaccine escape, as well as increased transmissibility and reinfection risk, explaining its rapid international spread that sparks a global alarm even more serious than the previously reported variants. Omicron has the capability to bypass at least some of the multi-faceted immune responses induced by prior infection or vaccination. It is shown to extensively escape neutralizing antibodies while evading cell mediated immune defense to a lesser extent. The efficacy of COVID 19 vaccines against Omicron variant is decreased with primary vaccination, showing that the vaccine is less efficient in preventing Omicron infections. However, after receiving a booster vaccine dose, the immunological response to Omicron significantly improved and hold promising results. Despite the mild nature of the disease in most vaccinated people, the rapid spread of Omicron, as well as the increased risk of re-infection, poses yet another major public health concern. Therefore, effort should be devoted to maintaining the existing COVID 19 preventive measures as well as developing new vaccination strategies in order to control the fast dissemination of Omicron.
Introduction
The coronavirus disease of 2019 (COVID-19), which is caused by severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), was first emerged in the Wuhan province of China, in December 2019. SARS-CoV-2 is a 30 kilobase enveloped single-stranded RNA virus that has been found to be the third beta coronavirus pandemic after severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS).Citation1–3 Despite many attempts to contain its spread, COVID-19 continues to become a significant public health concern and inflict enormous burdens of morbidity and mortality while seriously challenging the globe to unprecedented strain on health system, economies, and social life.Citation4,Citation5 This challenge could be due to comorbidities (complications) associated with COVID 19, such as hypertension, neurological disorders, diabetes, cancer, endothelial injury, CVDs, or hypercoagulability conditions, such as gangrene, stroke, and pulmonary embolism. These comorbidities have been observed in 75% of hospitalized COVID-19 patients and reported to increase the global burden of COVID 19.Citation6 The surging of the COVID-19 pandemic, which is largely due to the advent of new SARS-CoV-2 variants that are linked with enhanced transmissibility and infectivity as well as compromised vaccine efficacy, could be another of challenge of COVID 19.Citation7 As per 8 March 2022 World Health Organization (WHO) report, COVID-19 is continuing to spread around the world, with more than 446 million confirmed cases and above 6 million deaths across almost 224 countries.Citation8
Constant evolution of the authentic SARS-CoV-2 through high rates of mutations of different viral genes has been suggested to result in the emergence of new SARS-CoV-2 variants.Citation9 Previously, many SARS-CoV-2 variants that are associated with increased transmissibility and infectivity were identified. More recently, a novel variant of SARS-CoV-2 has been discovered in South Africa, known as Omicron. The emergence of the Omicron variant has posed new hurdles in the fight against SARS-CoV-2, putting the entire scientific community in jeopardy by affecting the transmissibility, disease severity, immunity, and diagnosis or therapy of COVID 19.Citation10 It is therefore of utmost importance to look at the mutational pattern of the Omicron variant and its negative impacts, as well as possible preventive strategies against the novel SARS-CoV-2 variant. This review therefore primarily explores the mutational pattern, negative impacts, and potential preventive strategies of Omicron SARS-CoV-2 variant infection. The information provided in the present review will be useful in providing current, up-to-date information regarding the Omicron variant, as well as pinpointing the negative effects of this new variant and its preventive strategies to tackle the spread of SARS-CoV-2, thus reducing the burden of the COVID-19 pandemic and preventing the emergence of novel variants in the future.
Overview of the Omicron SARS CoV-2 Variant
Several new strains of SARS-CoV-2 have been propagating around the world since the outbreak of the COVID 19 pandemics.Citation7,Citation11 The Alpha, Beta, Gamma, Delta, Epsilon, Eta, Theta, Iota, Kappa, Lambda, and Mu variants have been previously identified as SARS-CoV-2 variants. For the purpose of monitoring and research priority of these variants, the WHO has classified them into four categories: variants of high consequence (VOHC), variants of concern (VOCs), variants of interest (VOIs), and variants under monitoring (VUMs).Citation11,Citation12 VOCs are variants of global concern as they are linked with increased transmissibility, pathogenicity, disease severity (increased hospitalization and death), immune escape, diagnostic failure, and vaccine (therapeutic) escape.Citation13
Until late November 2021, there were four VOCs, namely, Alpha (lineage B.1.1.7 or UK variant), Beta (lineage B.1.351 or South Africa variant), Gamma (lineage P.1 or Brazil variant), and Delta (lineage B.1.617.2 variants) that substantially results in new waves of pandemic, causing significant number of cases and deaths across several countries of the globe.Citation14 At the end of November 2021, a novel SARS-CoV-2 variant known as the Omicron variant (lineage B.1.1.529), was identified and designated as the fifth VOC by the WHO. The Omicron variant was discovered for the first time in the Gauteng province of South Africa on 24 November 2021 using genomic sequencing and epidemiological data. Initially, it was considered as a variant under monitoring (VUM) and then, two days later, on 26 November 2021, the WHO declared B.1.1.529 as a VOC based on evidence that it contains numerous mutations influencing its characteristics and designated as “Omicron” from the 15th letter of the Greek alphabet.Citation14 The Omicron variant is now causing fast dissemination in human populations and has become a major global concern, showing its significant transmission potential.
Research done using whole genome sequencing unveiled the existence of three sub lineages of Omicron (lineage B.1.1.529). The standard sub lineage of Omicron is designated as BA.1 (B.1.1.529.1), whereas the other two new sub lineages of Omicron are referred to as BA.2 (B.1.1.529.2) and BA.3 (B.1.1.529.3).Citation15 While BA.1 is the dominant strain discovered first, the BA.2 and BA.3 sublineages are rare subvariants of Omicron that have been announced later. The BA.2 subvariant is nearly 30% more transmissible than the BA.1, and it is currently showing a sign of rapid growth, with BA.2 cases accounting for roughly one-fifth of all global COVID-19 infections.Citation16 As of the 31 January 2022 report, this subvariant has been detected in 57 countries worldwide.Citation17 Although these sublineages of Omicron variants overlap several mutations, they are vastly different, even as distinct as other variants, and some scientists believe that they deserve their own Greek letter. While BA.1 and BA.2 possess 32 mutations in common, they differ by 28 mutations.Citation18 Unlike the BA.2 sub lineage, both the BA.1 and BA.3 sublineages have S gene target failure (SGTF) from Δ69-70 deletion that aids in their detection by SGTF-based PCR diagnostics.Citation15
Mutational Patterns of the Omicron Variant
Omicron variant exceptionally contains the largest number of mutations among all SARSCoV-2 variants characterized by far.Citation19 Structural analysis indicated that this variant was found to have 60 mutations, 50 of which are non-synonymous mutations, 8 are synonymous mutations, and two are non-sense mutations, resulting in amino acid substitution, deletion, and insertion into the proteins of the Omicron variant ().Citation20–22 Omicron unusually contains 34 mutations in the S protein, which is about 3–4 times higher than the prior four widely circulating VOCs, each possessing twelve or fewer mutations in the S protein.Citation19 Compared with the original strain, Omicron was identified to contain thirty non-synonymous substitutions that change the amino acid sequence in the S protein. These substitutions in S protein of Omicron are A67V, T95I, Y145D, L212I, G339D, S371L, S373P, S375F, K417N, N440K, G446S, S477N, T478K, E484A, Q493R, G496S, Q498R, N501Y, Y505H, T547K, D614G, H655Y, N679K, P681H, N764K, D796Y, N856K, Q954H, N969K, and L981F. There are also three additional small deletions, including deletions of H69/V70 (Δ69-70), G142/V143/Y144 (Δ142-144) and N211 (Δ211), as well as an insertion of three amino acids (EPE) at position 214 (214EPE) in the S protein of the Omicron variant.Citation21,Citation23,Citation24 The majority of mutations in various SARS-COV-2 variants, including Omicron, are found in the S protein, likely as a result of selection for immune evasion.
Figure 1 The schematic illustration of the mutational pattern of Omicron SARS-CoV-2 variant. Omicron variant harbors 60 mutations that can be substitution, deletion and insertion of amino acids. Most (thirty-four) of these mutations are concentrated in the S protein; of which nearly half of mutations (fifteen) are localized in RBD (a key part of S protein) and three mutations are found in S1/S2-cleavage site (required for viral entry). These mutations are linked with increased transmission potential, reinfection risk, immune or vaccine evasion, and diagnostic problem. The remaining Omicron mutations, which are less likely associated with the impacts of Omicron variant, are found in other non-S protein genomic region, including other structural proteins (E-, M-, and N-protein) and non-structural proteins (nsp) in ORF1ab region, as well as in ORF9b.
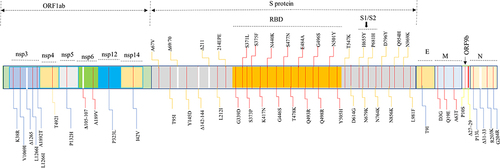
The receptor binding domain (RBD) is a small patch at the tip of the S protein that binds directly to human angiotensin converting enzyme 2 (ACE2) for SARS-CoV-2 entry into human cells.Citation25 While there is one RBD mutation in alpha, three in Beta and Gamma, and two in Delta, the Omicron variant uniquely harbors fifteen mutations. The critical mutations at the RBD of the S protein of the Omicron variant are G339D, S371L, S373P, S375F, K417N, N440K, G446S, S477N, T478K, E484A, Q493R, G496S, Q498R, N501Y, and Y505H.Citation20 Mutations in this particular region of S protein enhance the affinity of RBD to ACE2 and hence the transmissibility by 7-folds for alpha, 19-folds for both beta and gamma, and 2-folds for Delta.Citation26 According to the study by Kumar et al, the Omicron variant has a higher affinity for ACE2 than the Delta variant due to a significant number of mutations in RBD.Citation27 Based on docking studies, the Q493R, N501Y, S371L, S373P, S375F, Q498R, and T478K mutations greatly contribute to increased RBD binding with ACE2, transmission potential, pathogenicity, and immune escape of Omicron.Citation27–29 Three mutations (H655Y, N679K, and P681H) have been identified in the S1-S2 furin cleavage site, which is one of two cleavage sites in the S protein of SARS-CoV-2 during viral entry, and are linked with enhanced transmissibility and infectivity of the Omicron variant.Citation27,Citation30,Citation31
Moreover, the remaining mutations (substitutions and deletions) of omicron are found in non-S protein genomic regions, though they are assumed to be of less significance with regard to the transmissibility and infectivity of SARS-CoV-2.Citation32 In addition to the S protein, Omicron mutations are present in other structural proteins, including one substitution (T9I) in the envelope (E), three substitutions (D3G, Q19E, and A63T) in the membrane (M), and three substitutions (P13L, R203K, and G204R) and a three-residue deletion (Δ31-33) in the nucleocapsid (N) proteins.Citation19 In the Omicron variant, N protein mutations may result in enhanced sub genomic RNA expression and increased viral loads.Citation33,Citation34
The Omicron variant also harbors nine substitutions (K38R, V1069I, L1266I, A1892T, T492I, P132H, A189V, P323L, and I42V) and two deletions (Δ1265 and Δ105-107) within ORF1ab. In particular, this variant has five mutations (K38R, V1069I, Δ1265, L1266I, A1892T) in non-structural protein (nsp) 3, One mutation (T492I) in nsp4, a single mutation (P132H) in nsp5, two mutations (Δ105-107, A189V) in nsp6, as well as one mutation (P323L) in nsp12 and a single mutation (I42V) within nsp14 of ORF1ab involving ORF1a and ORF1b. Besides, a P10S substitution and a three-residue deletion (Δ27–29) are observed in ORF9b.Citation31,Citation35 These mutations may escape innate immunity, presumably by hampering the ability of infected cells to degrade viral components.
Phylogenetic analysis showed that Omicron is closely related to other variants and carries several mutations that have also appeared in previous mutated strains, such as alpha, beta, gamma, delta, kappa, zeta, lambda, and mu, suggesting its shared characteristics to all other variants, at least at the molecular level.Citation36,Citation37 The newly emerged Omicron variant coincides with several key mutations (D614G, Δ69-70 deletion, T95I, Δ142–144, K417N, T478K, N501Y, N655Y, N679K, and P681H) with previously identified VOCs, leading to increased transmissibility, viral binding affinity, and antibody escape.Citation38,Citation39 Omicron has a D614G change in its S protein, which is common in all other VOCs and increases its infectivity and pathogenicity.Citation40–42 Omicron shares the Δ69-70 deletion with the Alpha variant and causes SGTF.Citation36 Omicron also carries similar mutations with Beta and Gamma variants (K417N, T478K, N501Y) and Delta variant (T478K), conferring resistance to neutralizing antibodies.Citation36,Citation43 Despite the fact that most of the mutations in the Omicron variants are shared with other VOCs, there are 23 unique omicron mutations that are not found in any of the prior variants, some of which raise serious concerns by increasing transmissibility.Citation32,Citation37,Citation39
Negative Impacts of Omicron SARS‐CoV‐2 Variant
Currently, Omicron SARS‐CoV‐2 variant is becoming more concerning due to its impact on the virus’s transmissibility, pathogenicity, risk of reinfection, immune response as well as diagnostic equipment performance and vaccine effectiveness.Citation28,Citation29,Citation44 The significant sets of genetic mutations observed in the S protein of the newly emerged omicron variant, particularly those mutations shared with other VOCs, are associated with higher viral binding, transmissibility, pathogenicity, re-infection risk, as well as a wide spread immune escape and diagnostic failure.Citation37,Citation39 The possible negative influences of the Omicron variant on immune response, vaccination efficacy, transmissibility, re-infection, disease severity, and diagnostic modalities are all discussed in this section of the review.
Impacts of Omicron on the Body’s Immune Response
Multi-faceted protective immune responses involving T cell-mediated and antibody led immune defenses have been developed against SARS-CoV-2 natural infection or vaccination.Citation45–48 The viral ligand S protein, which interacts with the ACE2 receptor of the host cells, is the principal target of infection and vaccine induced immune responses. Omicron variants with S protein mutations have been shown to circumvent at least some of the multi-faceted immune response (humoral and cellular immunity) induced by prior infection or vaccination.Citation49
Humoral Immune Evasion
Humoral immunity is a key part of adaptive immunity for the anti-viral defense, including SARS-CoV-2.Citation50,Citation51 Several studies showed a severely reduced serum neutralizing capacity of vaccinated and convalescent patients against the omicron variant, demonstrating its potential for humoral immune evasion.Citation52 Omicron has been found to exhibit an unprecedented degree of neutralizing antibody escape compared with previously reported SARS-CoV-2 variants.Citation53 This is supported by recent studies reporting a substantially reduced neutralizing activity of the human serum against Omicron in COVID-19 convalescent donors in comparison to the original Wuhan, Beta, and Delta variants.Citation54,Citation55 Compared to the D614G strain, the mean neutralization of the sera of COVID-19 convalescent patients (infected with the original strain) against Omicron was found to be about 8.4-folds lower, though the neutralization of other VOCs was only about 1.2–4.5-folds lower.Citation52,Citation56
Moreover, the Omicron variant has been proven to defy therapeutic monoclonal antibody (mAb) therapy that has been used to treat other VOCs.Citation44,Citation57,Citation58 This is also evident from the failed neutralization of Omicron by mAb (imdevimab, casirivimab, bamlanivimab, and etesevimab) while they efficiently prevented Delta or other variant infections, highlighting its capability to bypass humoral immunity.Citation59
Overall, Omicron has a substantial ability to evade humoral immune protection developed after vaccination, mAb treatment, or prior infection (by the original strain or other variants), likely due to the heavily mutated RBD in Omicron compared to other VOCs.Citation27,Citation52 RBD is the most important part of the S protein for SARS-CoV-2 neutralization (targeted by more than 90% of neutralizing antibodies from mAb treatment and vaccines) and operates like a “grappling hook” for Omicron SARS-CoV-2 virus entry and immune escape.Citation60–63
Cell Mediate Immune Evasion
Viruses generally have a high capacity to evade humoral immunity, while they encounter difficulty to escape T-cell mediated immunity due to the broad and adaptable response produced in a given individual, as well as the variety of human leukocyte antigen (HLA) haplotypes between individuals.Citation49,Citation64 The Omicron SARS-CoV-2 variant, on the other hand, appears to elude the cell mediated immune defense to a lesser extent while extensively escaping neutralizing antibodies.Citation65 Many preliminary evidence suggests that Omicron reduces cellular immunity only mildly, but more significantly than other VOCs, owing to a heavily mutated S protein.Citation65,Citation66 A report by May et al showed that Omicron partially escapes the T-cell mediated immunity generated by the COVID 19 vaccines.Citation65 About 20% of CD4+ T-cell epitopes were reported to be affected by Omicron mutations, but nearly one third of the T-cell immunity was reduced and the rest two-thirds remained preserved as the higher immunogenicity of some epitopes produces a more robust T-cell response.Citation65
In contrast, some studies showed that despite the substantial number of mutations in the Omicron, there was no extensive accumulation of mutations for CD8+ T-cell escape, and thus, convalescent individuals (27 to 62 days after symptom resolution) elicited a broad range of immune responses to combat Omicron.Citation67,Citation68 A very minimal cross-over was observed with the identified epitopes associated with mutations in the original strain and other VOCs, suggesting that the CD8+ T cell response in the earlier infection would almost certainly remain effective against the Omicron variants.Citation68 In line with this, another study indicates that the existing CD8+ T-cell responses induced by prior SARS-CoV-2 infection and vaccination still recognize the Omicron variant and provide a significant level of protection from severe disease.Citation49 Collectively, cellular immune responses elicited by infection or vaccination partially offset the abrogation of humoral immunity and likely play a relatively more important role in protection against novel variants to control infection and limit progression to severe disease.Citation65,Citation69
Impacts of Omicron Variant on COVID-19 Vaccine Efficacy
As of December 2021, WHO has approved the use of ten COVID 19 vaccines: mRNA-1273 (Moderna), BNT162b2 (Pfizer-BioNTech), AZD1222 (AstraZeneca), Ad26.COV2.S (Johnson and Johnson), NVX-CoV2373 (Novavax), COVOVAX, Covaxin (Bharar Biotech), Covishield, BBIBP-CorV, Sinopharm (Beijing), and Sinovac (CoronaVac).Citation70 These COVID 19 vaccines are designed based on the ancestral SARS-CoV-2 strain and are prepared to elicit primarily protective antibody responses against the S protein and, to a lesser extent, T-cell responses.Citation44
Several prior works have indicated that the humoral response induced by the current COVID 19 vaccine was reduced against the previous widely circulating VOCs.Citation71,Citation72 Many recent preprint and published research results also indicate dramatically reduced neutralization titers against Omicron and hence it has the most significant escape from the sera of subjects recently vaccinated with licensed COVID-19 vaccines ().Citation52,Citation56,Citation73,Citation74 Even in people who have been immunized, it is found to resist the vaccine-elicited immune response by extensively impairing humoral immunity and, to a lesser degree, cellular immunity.Citation71–73,Citation75–77 Overall, Omicron has been shown to have a cumulative effect on diminishing the efficacy of COVID 19 vaccines, although it may partially protective vaccinated persons from severe diseases, hospitalization, and death likely due to T-cell mediated immunity.
Table 1 Summary on the Efficacy of Different COVID 19 Vaccines Against Omicron SARS-CoV-2 Variant
The vaccination escape in Omicron is associated with key mutations in the S protein of Omicron shared with other VOCs, such as D614G, K417N, E484A, P681H, and N501Y, as well as other mutations that are thought to be vaccine efficacy-reducing mutations that evade the immune protection conferred by COVID-19 vaccines.Citation78,Citation79 As compared to other VOCs, Omicron also possesses several additional RBD mutations that are expected to boost its ability to escape neutralizing antibodies and signal a major risk of vaccine escape than the prior variants.Citation32,Citation37,Citation39 The efficacy of COVID 19 vaccines with primary and booster immunization is discussed below.
COVID 19 Vaccine Efficacy Against Omicron with Primary Immunization
A study on PIKA-adjuvanted recombinant S protein subunit vaccine (YS-SC2-010) by Liu and his coworkers showed that the neutralizing antibody in the serum of animals inoculated with YS-SC2-010 was reported to be lower than other variants in neutralizing the Omicron variant.Citation10 Though immunization with YS-SC2-010 achieved high and long lasting (up to 20 months) neutralization against the Omicron variant, the neutralization effect of immune serum on Omicron decreased by 6.29-folds as compared to D614G and other mutant strains.Citation10 Particularly, the antibody titer against Omicron was observed to decrease by more than 90% when compared with the Delta strain.Citation52
Omicron was also shown to escape antibody neutralization by the BNT162b2 vaccine from Pfizer-BioNTech.Citation80 Several recent studies involving neutralization assays showed a highly reduced neutralization of the Omicron variant by human sera from two dose BNT162b2 vaccinated persons.Citation52,Citation73,Citation81,Citation82 A study by Wilhelm et al also indicated that the neutralization capacity of Omicron was reduced by 32.8-fold using sera from double BNT162b2-vaccinated individuals.Citation52 Another study also showed that the vaccine effectiveness after two BNT162b2 doses was 88.0% after 2–9 weeks of the second dose, lowering to 34–37% after 15 weeks of post dose two.Citation71 Similarly, Dejnirattisai et al also reported that vaccination with two BNT162b2 doses confers no or little protection against symptomatic disease with the Omicron variant.Citation44 A highly decreased neutralization of Omicron by the sera from BNT162b2 vaccinated people linked with reduced binding to the RBD has also been reported by Schubert et al.Citation63
Several other recent studies have also confirmed a substantial reduction in the neutralizing activity of the human serum against Omicron in fully BNT162b2 vaccinated people when compared to the original Wuhan strain, Beta, and Delta variants.Citation54,Citation55,Citation83,Citation84 Many studies indicate a 20–40-fold reduction in neutralizing activity of the sera from two dose BNT162b2 vaccine recipients compared to early pandemic viruses, and at least a 10-fold reduction compared to the Delta variant.Citation7,Citation52,Citation73,Citation85 Collie et al have documented 50–70% of vaccine protection against the Omicron variant after two doses of the BNT162b2 vaccine, which is lower than Delta (90–95%).Citation80
A substantial decrement in neutralization titers in individuals vaccinated with two BNT162b2 or ChAdOx1 (Vaxzevria, AstraZeneca) doses has also been observed by some other studies. According to a prospective study, post-vaccination antibody levels significantly increase after the second dose of the BNT162b2 mRNA COVID-19 vaccine, followed by a significant and rapid decay of anti-SARS-CoV-2 antibodies in infection-naïve healthcare workers four months after vaccination, suggesting that the vaccine offers little protection against the new variants.Citation86 Vaccination with two homologous BNT162b2 or ChAdOx1 doses provides no or limited protection against the Omicron variant. Neutralizing titers on sera from homologous ChAdOx1 dropped to below the detectable level, while neutralizing titers on sera from homologous BNT162b2 were above the detection threshold but reduced by 29.8-fold.Citation44 A greater reduction in neutralizing activity was observed from two doses of the ChAdOx1 or heterologous ChAdOx1/BNT162b2 vaccinations.Citation52,Citation73 Andrews et al indicated that 15 weeks after two ChAdOx1 doses showed no effect against Omicron.Citation71 On the other hand, no vaccine efficacy against Omicron was observed using sera from heterologous ChAdOx1/BNT162b2 vaccinated individuals, while poor neutralization against Delta was reported.Citation52 In contrary, neutralization of Omicron antibodies induced upon heterologous ChAdOx1/BNT162b2-vaccination was more efficient.Citation85
The sera of Ad26.COV2.S (from Johnson and Johnson), mRNA-1273 (from Moderna), or AZD1222 (from the Oxford/AstraZeneca)-vaccinated individuals showed lower RBD binding and thereby neutralization against Omicron.Citation63,Citation87 The neutralizing antibody titers against Omicron were low, even below the limit of detection in a considerable fraction of Ad26 or double dose mRNA vaccine recipients.Citation53 The neutralization capacity of Omicron was 20-fold reduced using sera from double mRNA1273-vaccinated individuals without any booster.Citation52 Another report also found that antibodies against Omicron are 4.5 times less potent than those against Delta, and the vaccine protection against symptomatic Omicron infection fell below 20% after two doses.Citation7
COVID 19 Vaccine Efficacy Against Omicron with Booster Immunization
Despite the low vaccine effectiveness after primary vaccination, there are some promising results that the booster dose of a COVID-19 vaccine does indeed significantly ameliorate SARS CoV-2 neutralizing antibody titers and improve vaccine effectiveness against the omicron variant.Citation7 The booster dose of COVID 19 vaccines after primary immunization increases the protection against Omicron but with a reduced level of antibody neutralization titers, suggesting that the Omicron variant may escape from vaccine elicited immune protection to a greater extent than other variants.Citation88
A plethora of recent studies revealed that sufficient neutralization (albeit with reduced neutralization) conferred improved protection against Omicron in recipients of the third booster doses of BNT162b2 when compared to the double doses of vaccinations.Citation54,Citation55,Citation83,Citation84 In spite of the fact that booster dose vaccine-induced responses surpass naturally-acquired immunity, different studies have reported that the neutralization and protection against this variant remain low. Basile and his coworkers demonstrated that neutralization titer is boosted from the third dose of the BNT162b2 vaccine, though it is still reduced by up to 4-folds compared to other variants.Citation81 This is supported by Wilhelm et al showing a significant increase in neutralizing titers from the BNT162b2-booster dose, though there was a 27.1-fold reduction in neutralization against Omicron.Citation52
A higher neutralizing activity was also demonstrated by Andrews et al after a BNT162b2booster dose for ChAdOx1/BNT162b2 primary course recipients. From two weeks after a BNT162b2 booster, vaccine efficacy was increased to 71.4% and 75.5% for ChAdOx1 and BNT162b2 primary course recipients, respectively.Citation71 In contrast, a study by Schubert et al demonstrated no change in the interaction of RBD with ACE2 and hence immune response by the BNT162b2 booster vaccination as compared to BNT162b2 fully vaccinated people. The serum of both BNT162b2 vaccinated and booster vaccinated persons showed a reduced binding to Omicron RBD, revealing no improvement in immune response with booster dose.Citation63
Recipients of the third booster dose of mRNA-1273 have been shown to significantly increase serum neutralizing activity and protection against Omicron compared to the two doses vaccinations.Citation54,Citation83 This is in corroboration with Schmidt et al showing those individuals who have received three doses of mRNA vaccines have substantial neutralizing antibody titers against Omicron after about one month of a booster jab.Citation53 A report from the UK has also shown that the protection given by the vaccine against Omicron infection is about 55–80% after a booster dose, but the vaccine effectiveness against Omicron after 60 days of a booster is 80–86%.Citation7
Neutralization against the Omicron variant has also been enhanced by the booster BBIBP-CorV vaccine following two-dose priming vaccination.Citation88 Yu and his coworkers showed that a booster dose of BBIBP-CorV results in a significant rebound in neutralizing immune response against SARS-CoV-2, which is 6.1 times greater in neutralization titer than the level after 28 days of the second dose. Nevertheless, it is reduced by 20.1-fold as compared with the wild-type strain, implying that the Omicron variant still has the ability to partially escape from booster-enhanced neutralization.Citation88
Collectively, booster immunizations with COVID 19 vaccines after primary immunization may be critical to substantially improve the humoral immune response against the Omicron variant, but to a much lesser extent than any other VOCs ().Citation54,Citation71,Citation82 Thus, the observation that the primary immunization is insufficient to neutralize Omicron warrants the rapid administration of a booster vaccine dose to prevent contracting with Omicron infection.Citation55,Citation83,Citation84
Transmissibility of Omicron SARS-CoV-2 Variant
Although further supporting evidence is required, available data indicated that omicron is likely to be highly transmissible.Citation19 Initially, the Omicron outbreak has been first identified in the Gauteng provinces of South Africa. Studies showed that the percentage of Omicron infections reached nearly 90% within about 25 days in South Africa, while the percentage of Beta and Delta variant infections was 50% and 80% respectively, within 100 days since its outbreak in South Africa, indicating its faster dissemination in the population.Citation19 Omicron was observed to have a doubling time of 1.2 days, which is faster than that of the Beta and Delta variants, that have doubling times of about 1.7 and 1.5 days, respectively.Citation36
At the beginning of this outbreak, the Omicron variant was swiftly substituting other circulating variants, including the dominant Delta variant in the Gauteng provinces of South Africa, and was rapidly spreading in other provinces of South Africa.Citation89 Then this variant was expanded to other African countries and disseminated outside of Africa as of 24 November 2021. Hong Kong was the first place outside Africa that had confirmed a case of Omicron from a person who traveled from South Africa in November 2021. One confirmed Omicron case was identified in Israel from a traveler returning from Malawi on 25 November 2021. The first Omicron case was detected in Romania on December 2021, in previously vaccinated individuals who developed mild symptoms shortly after returning from the UK and had undergone multiple rapid antigen tests with negative results, even after being tested by RT-PCR for 7 days in a row.Citation90 Currently, the Omicron variant is highly expanding to involve several other countries in the world such as Belgium, Germany, Italy, Netherlands, Australia, Denmark, Czech Republic, Canada, Singapore, Portugal, Sweden, Japan, the UK, Scotland, Malaysia, New Zealand, and South Korea.Citation91 As of 8 March 2022, WHO report, a total of 2.4 million confirmed cases of Omicron infection have been identified in 170 nations across the six continents of the globe.Citation14
Altogether, Omicron is believed to be far more infectious than prior VOCs, including the Delta and Beta variants. Omicron has been found seven times more contagious than the Delta variant, indicating that Omicron is turned out to be the most transmissible virus yet seen.Citation29 It is now rapidly outcompeting even the most dominant Delta variant and is resulting in an unprecedented surge in cases, raising great public health worries.Citation92 Thus far, Omicron has apparently become the most prevalent variant in countries like South Africa, the UK, the Canadian province of Ontario, Denmark, Switzerland, Germany, Scotland, the US, Belgium, Portugal, Norway, Italy, France, Romania, and the Netherlands.Citation91
The presence of key mutations in the S protein of Omicron, particularly D614G, N501Y, E484 N679K, P681H, and T478K mutations, has been demonstrated to induce higher transmissibility or infectivity.Citation93,Citation94 Omicron, like Alpha, Beta, and Gamma variants, has D614G and N501Y mutations that are believed to enhance the binding of S protein to ACE2 and thereby transmissibility.Citation94,Citation95 Similar to the Alpha variant, the transmissibility of Omicron could be further increased by Δ69-70 deletion.Citation29 Besides, the incorporation of basic amino acids around the furin cleavage site of Omicron’s S protein as a result of N679K and P681H mutations could facilitate the cleavage of the S protein into S1 and S2, thus enhancing fusion and infectivity similar to the Alpha variant.Citation30,Citation31,Citation96 A higher binding of Omicron to ACE2 and more infectivity than the Delta variant could be due to E484 mutations.Citation30 As the T470-T478 loop and Y505 of RBD are required for ACE2 binding, mutations like T478K may improve the infectivity of Omicron like Delta strains.Citation63,Citation97
Risk of Reinfection with Omicron Variant
The Omicron variant has been proven to have a substantial ability to defy prior infection induced immunity, suggesting an increased risk of reinfection.Citation57,Citation58 Omicron could show a higher risk of reinfection not observed in other variants, even in people having immunity to prior infection or vaccination.Citation57 There is documented evidence showing that omicron has a substantially greater propensity to infect individuals who have received vaccines or who have had COVID than earlier VOCs.Citation89 There is more than five times high likelihood of reinfection of people with the Omicron variant compared with Delta.Citation98 This could be owing to the greater ability of the Omicron variant to escape immune defense induced by prior infection or vaccination due to its heavily mutated S protein. The immune evasion in turn may hamper its capacity to combat omicron, leading to a high incidence of breakthrough infection or re-infection with omicron strains.
Clinical Presentation and Disease Severity of Omicron Infection
Despite the fact that Omicron is a VOC capable of breaking natural and vaccine-induced immune defenses, there is no evidence so far indicating that it causes different symptoms from other variants.Citation14,Citation20 Omicron infection has similar clinical presentations to past variants, such as fever, fatigue, body aches, sore throat, cough, and rhinorrhea, but it uniquely manifests with repeated episodes of extreme night sweats, soaking clothes and sheets.Citation57,Citation99 The Omicron infections that were first reported in South Africa were milder than other variants, and raised no alarming clinical concerns.Citation29 This has now been turned out to be real, as proved by a growing body of data demonstrating the Omicron variant is less virulent than the previous VOCs, including the Delta strain.Citation57,Citation100 This is evident by the fact that there have been few or no reports of serious sickness, hospitalization, or death from Omicron infection. According to a recent report, COVID 19 caused by the omicron variant is 50–70% less likely to result in hospitalization than COVID 19 by Delta variant.Citation93 In line with this, a report from the UK found that hospital admissions with Omicron were nearly half of those for Delta variant.Citation7 Another study from Southern California also confirmed that Omicron infection is 91% less fatal than the Delta variant and has a 51% lower chance of hospitalization.Citation101 A 70-fold quicker proliferation of Omicron in the bronchi than Delta strain but less capability of penetrating the lung suggested to be the less risk of developing severe illness and hospitalization by Omicron infection compared to the prior VOCs.Citation100,Citation102 This could be due to the immune response like non-neutralizing antibodies and cellular immunity, which are less likely to be severely affected by this variant and may confer some degree of protection against severe disease.Citation44
Even though Omicron infections are reported to be clinically milder, those with comorbidities, immunocompromised patients as well as unvaccinated individuals may behave differently and are at high risk for complications or severe COVID 19.Citation103 This supported by Malik et al that reported ICU admissions and deaths are being driven by patients with comorbidities, people who are immunocompromised, and the aged.Citation6 Regardless of the type variants, people with comorbidities are the most vulnerable during SARS-CoV-2 infection, even for the Omicron variant.
Impacts of Omicron Variants on Diagnostic Equipment Performance
Like Alpha and Eta variants, the Δ69-70 deletion in Omicron is helpful for easy detection with PCR testing.Citation36,Citation104 Just as it did for the Alpha variant, the PCR diagnostics use the deleted S-gene as a marker for early detection of Omicron known as SGTF or S gene dropout.Citation105 The SGTF serves as a proxy indicator to ascertain whether or not it is the Omicron variant.Citation15 However, serious concerns have been raised with regard to the diagnostic equipment performance in identifying the Omicron variant due to its high number of mutations. Thus, the B.1.1.529 variant currently poses detection uncertainty in diagnostic laboratories, and the existing molecular tests that are widely used to diagnose SARS-CoV-2 infection are thought to be less effective in detecting this variant.Citation32 Epidemiological evidence also showed an increased detection failure by S-gene targeted-PCR testing for the Omicron variant.Citation19 The SGTF based diagnosis may result in false-negative readings in the S gene assay of the commonly used PCR test (TaqPath, Thermo Fisher Scientific, Waltham, MA, USA).Citation29,Citation104,Citation106 Specifically, the BA.2 subvariant of Omicron, which does not show the SGTF feature, potentially leads to detection problems and underestimation by SGTF-based PCR diagnostics, thus it is also named as stealth Omicron. However, the BA.1 and BA.3 sublineages do not result in potential detection problems associated with SGTF based PCR diagnostics since they have the characteristics of SGTF.Citation15,Citation105 Therefore, PCR testing using SGTF is inadequate to detect and monitor Omicron variant.Citation107
To rule out the presence of other variants and to definitively confirm the Omicron variant, whole genome sequencing, sanger sequencing of the S gene, or a variant-specific PCR could be employed.Citation29,Citation105 The ultimate diagnostic method for detecting gene mutations in Omicron is whole genome sequencing, though sanger sequencing and variant-specific PCR are less expensive but provide less sequencing information.Citation105 The N501Y-specific PCR, which was used to diagnose alpha variant, could be an option to detect Omicron variant since alpha variant is currently almost negligible. On the other hand, the L417N, L452R or E484A-specific PCR assays, can be used as alternative targets specific for omicron diagnosis.Citation29,Citation105 Otherwise, molecular diagnostic assays targeting conserved genomic sequences with the least risk of mutating should be developed to ensure that the existing circulating variants continue to bind efficiently with a primer.Citation105
Despite diagnostic ambiguities associated with Omicron detection, accumulated evidence shows that the current SARS-CoV-2 PCR diagnostics are still effective for detecting Omicron variant without getting delayed by the long process of comprehensive genome sequencing. The PCR test can, therefore, be used to identify the Omicron variant as early as possible, allowing for prompt therapy while awaiting for sequencing confirmation.Citation29,Citation105 In fact, the Omicron variant is currently becoming a dominant variant throughout several countries of the world.Citation17 Thus confirmation of Omicron is more a matter of curiosity than concern. Extensive sequence changes in Omicron are being studied to see if they have any effect on other types of diagnostic tools, such as rapid antigen detection tests.
Preventive Strategies to Curb the Spread of the Omicron Variant
Neutralizing antibody titers against Omicron were found to be low, even below the threshold of detection, in a substantial number of convalescent or vaccinated people.Citation53 The immune protection elicited by prior SARS-CoV-2 infection and primary immunization with authorized COVID 19 vaccines reported to be less effective in preventing Omicron infections.Citation44 Furthermore, Omicron may have evolved to be more easily spread among people and resistant to currently available mAb treatments.Citation44,Citation52,Citation53 Overall, as a result of its antigenic distance from ancestral strains, omicron leads to a high rate of dissemination and evasion of the body’s immunity and vaccine-induced immune response, making it a grave public health concern, even worse than other VOCs.Citation63 Therefore, modern public (social) health preventive strategies, as well as vaccination strategies, are required to battle current pandemics or prevent the occurrence of future pandemics.Citation19
Public Health Prevention Measures
To curb the spread of Omicron, efforts should be made to maintain existing public health prevention measures.Citation19 The same preventive measures that have been utilized to stop the spread of prior SARS-CoV-2 variants, such as wearing masks, adequate ventilation, social distancing, and hand washing, should be employed to effectively interrupt the transmission of the Omicron variant. Besides, early case detection using improved diagnostic tools, treatment of diagnosed patients, and timely isolation and strict quarantine of suspected or confirmed cases are also crucial to curb the spread of this variant.Citation19,Citation108
Appropriate and timely treatment of COVID 19 caused by Omicron SARS-CoV2 variant is of paramount importance to curb the spread of this variant to other individuals.Citation19,Citation108 Multiple reports, however, have revealed substantial therapeutic resistance to the available mAb agents such as imdevimab, casirivimab, bamlanivimab, and etesevimab that are used to treat other variants.Citation59 Hence, in light of the most recent available data, the Food and Drug Administration (FDA) has banned many mAbs for use in treating Omicron infection in the US as of January 24, 2022.Citation109 It is because most of the COVID 19 cases are due to Omicron variants and non-omicron variants are rare, and the therapeutic activities of these mAbs against the omicron variant are markedly reduced.
Although most mAbs are evaded by Omicron, Hoffmann et al found that Sotrovimab remains efficient against Omicron infection, possibly because sotrovimab targets a part of the S protein that is unchanged across many related coronaviruses.Citation85 But several other mAbs, such as Paxlovid, Veklury (remdesivir), and molnupiravir, are also expected to work against the omicron variant, and are approved by the FDA to treat patients with mild-to-moderate COVID-19 who are at high risk of progression to severe disease, including hospitalization or death.Citation109,Citation110 In addition, as of February 25, 2022, the FDA has authorized the use of bebtelovimab as an emergency treatment for COVID-19 patients who are at risk of progressing to severe disease or requiring hospitalization.Citation111 Generally, the concentration of mAbs required to halve viral replication is higher for Omicron than for other variants, and their potency is significantly reduced. Hence, designing a variant specific mAb treatment approach could be employed as an option to treat the Omicron variant.Citation52
However, the acceptance of these public health measures has been hampered by people’s erroneous perceptions about the impact that COVID-19 can have on adults and children. While parents continued to protect their children from COVID-19 by closing schools and kindergartens and limiting other educational or recreational activities, adults continued to work or maintain social interactions with friends or other family members. Besides, due to the fear of contracting the new SARS-CoV-2 infection or having their children hospitalized, parents opted to seek medical advice over the phone, or to self-medicate, which may result in the detrimental consequences of the COVID-19 pandemic on children. To lessen the negative impact on children, the adult population, especially parents, should follow the COVID 19 preventive rules, be aware of correct information by effectively communicating with medical staff, and get vaccinated.Citation112
Vaccination Strategies
Additionally, development of new vaccination strategies against Omicron needs to be considered to control its dissemination.Citation19 Like the Omicron variant, several additional VOCs could be seen in the future that potentially lead to a catastrophic pandemic. Increased viral transmission may enhance the opportunity for SARS-CoV-2 mutations to become new variant.Citation113 As a result, in the current global COVID 19 pandemic, safe and effective vaccines against circulating variants are the only way to halt the COVID 19 pandemic and also the most cost-effective solution to reduce its worldwide burden.Citation114 The global average COVID 19 vaccination coverage was, however, reported to be low (about 42%), thus accelerating the transmissibility of SARS-CoV-2, including Omicron, and promoting the evolution of novel variants.Citation15,Citation19 This highlights that full immunization of the global population with the COVID 19 vaccine to attain herd immunity may be the solution, even to avert the lurking threat of the evolving new and more dangerous SARS-CoV-2 variants. For SARS-CoV-2, the threshold level for herd immunity ranges between 60% and 83%.Citation115
There is a new notion proposing that a combination of infection and vaccination could generate high neutralization capacity, preserving reasonable effectiveness against Omicron.Citation73 Thus, universal COVID 19 vaccination should also involve those who have previously been infected with SARS-CoV-2, as subsequent vaccination of previously infected individuals has been reported to retain relatively high neutralization titers to protect against Omicron.Citation73 This is also supported by other studies indicating that individuals who had been previously infected with SARS-CoV-2 (or convalescent individuals) and subsequently received mRNA vaccines showed substantial neutralizing antibody titers against Omicron.Citation53,Citation82,Citation116 Individuals who have been previously infected and vaccinated with Pfizer BNT162b2 were estimated to have 73% protection against Omicron infection, while those who had never been infected were reported to retain only about 35% protection.Citation73 Despite the necessity for universal COVID l9 vaccination, public hesitation about the vaccine’s efficacy is a major global health challenge.Citation113 This public apprehension can be alleviated by raising public awareness and trust in COVID 19 vaccinations, and thereby enhancing herd immunity, which in turn, ultimately controls SARS-CoV-2 spread, such as Omicron variants.
In light of several reports demonstrating that the booster dose of COVID 19 vaccines after primary immunization enhances immune protection against Omicron, we suggest that adding a booster dose could be a helpful vaccination strategy as a control measure for omicron infection and transmission. Furthermore, as reported by many studies, the current COVID-19 vaccines are found to be poorly effective against Omicron and develop less immunity than other VOCs.Citation44,Citation58,Citation71 This observation will provide further understanding that developing vaccines specific to omicron using mutated S protein could be another option, though it is unlikely to provide protection against prior strains. Thus, there is a need to develop vaccines that will be efficacious against the newly emerged globally circulating worldwide mutants.Citation113 On the other hand, switching from the existing monovalent vaccine strategy to multivalent vaccine formulations, primarily to cover both the previous variants and Omicron, could potentially be an alternative to halt the progress of COVID 19.Citation44,Citation113 Overall, much effort should be made to develop effective vaccines against SARS-CoV-2 variants using strategies such as DNA-based vaccines, RNA-based vaccines, non-replicating viral vectors, replicating viral vectors, inactivated vaccines, live-attenuated vaccines, and protein subunits in order to tackle the current wave of COVID 19 pandemic and prevent another wave of the pandemic in the future.Citation117 Thus, more clinical studies are required to find the most successful vaccine that reduce COVID- 19 case surging while also combating the emergence of new variants.
Conclusion
In summary, the newly emerged Omicron SARS-CoV-2 variant possesses the most mutations of all the variants that have been discovered so far during the COVID 19 pandemic. Owing to the heavily mutated S protein, Omicron is highly scrutinized to be linked with immune escape, increased transmissibility and risk of reinfection, diagnostic or therapeutic escape, albeit with a milder disease nature. This variant substantially dodges immune responses, including infection-blocking antibodies and cell mediated immune responses elicited by prior infection or vaccination. Omicron has also been reported to have an extremely high-rate of dissemination in the community, and is believed to be far more infectious than prior VOCs, with a higher risk of reinfection due to its high potential for immunological evasion. Besides, this novel variant poses detection uncertainty in diagnostic laboratories. The current PCR testing may not detect Omicron variants, particularly the BA.2 sublineage missing SGTF feature, necessitating the development of new diagnostics. As a result, Omicron is now the VOC, prompting grave public worries even worse than the previously reported variants, and it will become the dominant strain worldwide.
Modern preventive public health measures as well as vaccination strategies are needed to battle current pandemics or prevent the occurrence of future pandemics. The existing COVID 19 preventive measures need to be maintained to prevent the spread of the Omicron variant. In addition, new vaccination strategies, such as universal vaccination (extensive and fair) of the global population as well as booster vaccines, multivalent vaccines, or variant-specific vaccine development, should be considered to treat Omicron and other emerging VOCs. These may be also the solutions to avert the future threat of the evolving SARS-CoV-2 variants.
Abbreviations
ACE2, angiotensin converting enzyme 2; COVID-19, Coronavirus disease of 2019; E protein, envelope protein; HLA, Human leukocyte antigen; M protein, membrane protein; mAb, monoclonal antibody; MERS, middle east respiratory syndrome; N protein, Nucleocapsid protein; nsp, non-structural protein; ORF, Open reading frame; PCR, Polymerase chain reaction; RBD, Receptor binding domain; S protein, Spike protein; SARS, severe acute respiratory syndrome; SARS-CoV-2, Severe acute respiratory syndrome coronavirus-2; SGTF, S gene target failure; VOC, Variant of concern.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
- Bos R, Rutten L, van der Lubbe JE, et al. Ad26 vector-based COVID-19 vaccine encoding a prefusion-stabilized SARS-CoV-2 spike immunogen induces potent humoral and cellular immune responses. NPJ Vaccines. 2020;5(1):1–11. doi:10.1038/s41541-020-00243-x
- Abebe EC, Dejenie TA, Shiferaw MY, et al. The newly emerged COVID-19 disease: a systemic review. Virol J. 2020;17(1):1–8. doi:10.1186/s12985-020-01363-5
- Boopathi S, Poma AB, Kolandaivel P. Novel 2019 coronavirus structure, mechanism of action, antiviral drug promises and rule out against its treatment. J Biomol Struct Dyn. 2020;39:1–10.
- Lazarus JV, Ratzan SC, Palayew A, et al. A global survey of potential acceptance of a COVID-19 vaccine. Nat Med. 2020;27:1–4.
- Guihot A, Litvinova E, Autran B, et al. Cell-mediated immune responses to COVID-19 infection. Front Immunol. 2020;11:1662. doi:10.3389/fimmu.2020.01662
- Malik JA, Ahmed S, Shinde M, et al. The impact of COVID-19 on the comorbidities: a review of recent updates for combating it. Saudi J Biol Sci. 2022;29(5):3586–3599. doi:10.1016/j.sjbs.2022.02.006
- England PH. SARS-CoV-2 variants of concern and variants under investigation in England. Tech Brief; 2021:12.
- World Health Organization. Weekly epidemiological update on COVID-19; 2022.
- Lauring AS, Malani PN. Variants of SARS-CoV-2. JAMA. 2021;326(9):880. doi:10.1001/jama.2021.14181
- Liu Y, Zhang N, Wang B, et al. Broad and long-lasting immune response against SARS-CoV-2 omicron and other variants by PIKA-adjuvanted recombinant SARS-CoV-2 Spike (S) protein subunit vaccine (YS-SC2-010). bioRxiv. 2021. doi:10.1101/2021.12.22.473615
- Center for Disease Control and Prevention. SARS-CoV-2 variant classifications and definitions; 2021.
- World Health Organization. Tracking SARS-CoV-2 variants; 2022.
- Dudas G, Hong SL, Potter BI, et al. Emergence and spread of SARS-CoV-2 lineage B. 1.620 with variant of concern-like mutations and deletions. Nat Commun. 2021;12(1):1–12. doi:10.1038/s41467-021-26055-8
- World Health Organization. Update on Omicron; 2021.
- Hanson. Classification of Omicron (B.1.1.529): SARS-CoV-2 variant of concern. 2021.
- Goodman B. New studies bring BA.2 variant into sharper focus; 2022.
- World Health Organization. COVID-19 weekly epidemiological update, Edition 77; 2022.
- G Mcgregor. “What is ‘stealth Omicron’? The rise of the subvariant is alarming some scientists who say it needs its own Greek letter. Fortune; 2022.
- He X, Hong W, Pan X, et al. SARS‐CoV‐2 Omicron variant: characteristics and prevention. MedComm. 2021;2(4):838–845. doi:10.1002/mco2.110
- Centers for Disease Control and Prevention. Science brief: omicron (B. 1.1. 529) variant; 2021.
- Bhoye S, Marakwad T. A comparative characteristics of both variants of severe acute respiratory syndrome Coronavirus-2 (SARS-CoV-2): delta and Omicron; 2021.
- Haseltine WA. Omicron Origin. Forbes; 2021.
- Cookson C, Barnes O. What we know about Omicron variant that has sparked global alarm. The Financial Times; 2021.
- Callaway E. Heavily mutated Omicron variant puts scientists on alert. Nature. 2021;600(7887):21. doi:10.1038/d41586-021-03552-w
- Chen J, Wang R, Gilby NB, et al. Omicron variant (B. 1.1. 529): infectivity, vaccine breakthrough, and antibody resistance. J Chem Inf Model. 2022;62(2):412–422. doi:10.1021/acs.jcim.1c01451
- Dejnirattisai W, Huo J, Zhou D, et al. SARS-CoV-2 Omicron-B. 1.1. 529 leads to widespread escape from neutralizing antibody responses. Cell. 2022;185(3):467–484.e15. doi:10.1016/j.cell.2021.12.046
- Kumar S, Thambiraja TS, Karuppanan K, et al. Omicron and delta variant of SARS‐CoV‐2: a comparative computational study of spike protein. J Med Virol. 2021;94(4):1641–1649.
- Saxena SK, Kumar S, Ansari S, et al. Characterization of the novel SARS‐CoV‐2 Omicron (B. 1.1. 529) variant of concern and its global perspective. J Med Virol. 2021;94(4):1738–1744.
- Quarleri J, Galvan V, Delpino M. Omicron variant of the SARS-CoV-2: a quest to define the consequences of its high mutational load. GeroScience. 2021:1–4. doi:10.1007/s11357-021-00500-4
- Gong SY, Chatterjee D, Richard J, et al. Contribution of single mutations to selected SARS-CoV-2 emerging variants spike antigenicity. Virology. 2021;563:134–145. doi:10.1016/j.virol.2021.09.001
- Pang X, Li P, Zhang L, et al. Emerging SARS-CoV-2 mutation hotspots associated with clinical outcomes and transmission. Front Microbiol. 2021;3047. doi:10.3389/fmicb.2021.753823
- Rao S, Singh M. The newly detected B. 1.1. 529 (Omicron) variant of SARS-CoV-2 with multiple mutations: implications for transmission, diagnostics, therapeutics, and immune evasion. DHR Proc. 2021;1(S5):7–10. doi:10.47488/dhrp.v1iS5.35
- Leary S, Gaudieri S, Parker MD, et al. Generation of a novel SARS-CoV-2 sub-genomic RNA due to the R203K/G204R variant in nucleocapsid. bioRxiv. 2021;2020:27.
- Mourier T, Shuaib M, Hala S, et al. Saudi Arabian SARS-CoV-2 genomes implicate a mutant Nucleocapsid protein in modulating host interactions and increased viral load in COVID-19 patients; 2021.
- Benvenuto D, Angeletti S, Giovanetti M, et al. Evolutionary analysis of SARS-CoV-2: how mutation of Non-Structural Protein 6 (NSP6) could affect viral autophagy. J Infect. 2020;81(1):e24–e7. doi:10.1016/j.jinf.2020.03.058
- Karim SSA, Karim QA. Omicron SARS-CoV-2 variant: a new chapter in the COVID-19 pandemic. Lancet. 2021;398(10317):2126–2128. doi:10.1016/S0140-6736(21)02758-6
- Kannan SR, Spratt AN, Sharma K, et al. Omicron SARS-CoV-2 variant: unique features and their impact on pre-existing antibodies. J Autoimmun. 2022;126:102779. doi:10.1016/j.jaut.2021.102779
- Greaney AJ, Starr TN, Gilchuk P, et al. Complete mapping of mutations to the SARS-CoV-2 spike receptor-binding domain that escape antibody recognition. Cell Host Microbe. 2021;29(1):44–57. e9. doi:10.1016/j.chom.2020.11.007
- Harvey WT, Carabelli AM, Jackson B, et al. SARS-CoV-2 variants, spike mutations and immune escape. Nat Rev Microbiol. 2021;19(7):409–424. doi:10.1038/s41579-021-00573-0
- Korber B, Fischer WM, Gnanakaran S, et al. Tracking changes in SARS-CoV-2 spike: evidence that D614G increases infectivity of the COVID-19 virus. Cell. 2020;182(4):812–27. e19. doi:10.1016/j.cell.2020.06.043
- Plante JA, Liu Y, Liu J, et al. Spike mutation D614G alters SARS-CoV-2 fitness. Nature. 2021;592(7852):116–121. doi:10.1038/s41586-020-2895-3
- Volz E, Hill V, McCrone JT, et al. Evaluating the effects of SARS-CoV-2 spike mutation D614G on transmissibility and pathogenicity. Cell. 2021;184(1):64–75. e11. doi:10.1016/j.cell.2020.11.020
- Tao K, Tzou PL, Nouhin J, et al. The biological and clinical significance of emerging SARS-CoV-2 variants. Nat Rev Genet. 2021;22(12):757–773. doi:10.1038/s41576-021-00408-x
- Dejnirattisai W, Shaw RH, Supasa P, et al. Reduced neutralisation of SARS-CoV-2 omicron B. 1.1. 529 variant by post-immunisation serum. Lancet. 2021. doi:10.1016/S2352-3018(21)00103-X
- Tada T, Zhou H, Samanovic MI, et al. Comparison of neutralizing antibody titers elicited by mRNA and adenoviral vector vaccine against SARS-CoV-2 variants. Biorxiv. 2021. doi:10.1101/2021.07.19.452771
- Guerrera G, Picozza M, D’Orso S, et al. BNT162b2 vaccination induces durable SARS-CoV-2–specific T cells with a stem cell memory phenotype. Sci Immunol. 2021;6(66):eabl5344. doi:10.1126/sciimmunol.abl5344
- Wall EC, Wu M, Harvey R, et al. AZD1222-induced neutralising antibody activity against SARS-CoV-2 Delta VOC. Lancet. 2021;398(10296):207–209. doi:10.1016/S0140-6736(21)01462-8
- Anichini G, Terrosi C, Gori Savellini G, et al. Neutralizing antibody response of vaccinees to SARS-CoV-2 variants. Vaccines. 2021;9(5):517. doi:10.3390/vaccines9050517
- Redd AD, Nardin A, Kared H, et al. Minimal cross-over between mutations associated with Omicron variant of SARS-CoV-2 and CD8+ T cell epitopes identified in COVID-19 convalescent individuals. bioRxiv. 2021. doi:10.1101/2021.12.06.471446
- Bošnjak B, Stein SC, Willenzon S, et al. Low serum neutralizing anti-SARS-CoV-2 S antibody levels in mildly affected COVID-19 convalescent patients revealed by two different detection methods. Cell Mol Immunol. 2021;18(4):936–944. doi:10.1038/s41423-020-00573-9
- Mengist HM, Kombe AJK, Mekonnen D, et al. editors. Mutations of SARS-CoV-2 spike protein: implications on immune evasion and vaccine-induced immunity. In::Seminars in Immunology. Elsevier; 2021.
- Wilhelm A, Widera M, Grikscheit K, et al. Reduced neutralization of SARS-CoV-2 Omicron variant by vaccine sera and monoclonal antibodies (preprint). medRxiv. 2021. doi:10.1101/2021.12.07.21267432
- Schmidt F, Muecksch F, Weisblum Y, et al. Plasma neutralization properties of the SARS-CoV-2 Omicron variant (preprint). medRxiv. 2022. doi:10.1101/2021.12.12.21267646
- Roessler A, Riepler L, Bante D, et al. SARS-CoV-2 B. 1.1. 529 variant (Omicron) evades neutralization by sera from vaccinated and convalescent individuals. medRxiv. 2021. doi:10.1101/2021.12.08.21267491
- Nemet I, Kliker L, Lustig Y, et al. Third BNT162b2 vaccination neutralization of SARS-CoV-2 Omicron infection. N Engl J Med. 2021;386(5):492–494.
- Zhang L, Li Q, Liang Z, et al. The significant immune escape of pseudotyped SARS-CoV-2 variant omicron. Emerg Microbes Infect. 2021;11:1–11.
- Pulliam JR, van Schalkwyk C, Govender N, et al. Increased risk of SARS-CoV-2 reinfection associated with emergence of the Omicron variant in South Africa. medRxiv. 2021. doi:10.1101/2021.11.11.21266068
- Aggarwal A, Stella AO, Walker G, et al. SARS-CoV-2 Omicron: reduction of potent humoral responses and resistance to clinical immunotherapeutics relative to viral variants of concern. medRxiv. 2021. doi:10.1101/2021.12.14.21267772
- Barnes CO, Jette CA, Abernathy ME, et al. SARS-CoV-2 neutralizing antibody structures inform therapeutic strategies. Nature. 2020;588(7839):682–687. doi:10.1038/s41586-020-2852-1
- Starr TN, Greaney AJ, Hilton SK, et al. Deep mutational scanning of SARS-CoV-2 receptor binding domain reveals constraints on folding and ACE2 binding. Cell. 2020;182(5):1295–310. e20. doi:10.1016/j.cell.2020.08.012
- Bertoglio F, Fühner V, Ruschig M, et al. A SARS-CoV-2 neutralizing antibody selected from COVID-19 patients by phage display is binding to the ACE2-RBD interface and is tolerant to known RBD mutations; 2020.
- Walls AC, Park Y-J, Tortorici MA, et al. Structure, function, and antigenicity of the SARS-CoV-2 spike glycoprotein. Cell. 2020;181(2):281–292. doi:10.1016/j.cell.2020.02.058
- Schubert M, Bertoglio F, Steinke S, et al. Human serum from SARS-CoV-2 vaccinated and COVID-19 patients shows reduced binding to the RBD of SARS-CoV-2 Omicron variant in comparison to the original Wuhan strain and the Beta and Delta variants. medRxiv. 2021. doi:10.1101/2021.12.10.21267523
- Tarke A, Sidney J, Methot N, et al. Impact of SARS-CoV-2 variants on the total CD4+ and CD8+ T cell reactivity in infected or vaccinated individuals. Cell Rep Med. 2021;2(7):100355. doi:10.1016/j.xcrm.2021.100355
- May DH, Rubin B, Dalai SC, et al. Omicron variant partially escapes the T-cell response induced by SARS-CoV-2 vaccines; 2021.
- Noh JY, Jeong HW, Kim JH, et al. T cell-oriented strategies for controlling the COVID-19 pandemic. Nat Rev Immunol. 2021;21(11):687–688. doi:10.1038/s41577-021-00625-9
- Kared H, Redd AD, Bloch EM, et al. SARS-CoV-2–specific CD8+ T cell responses in convalescent COVID-19 individuals. J Clin Invest. 2021;131(5). doi:10.1172/JCI145476.
- Redd AD, Nardin A, Kared H, et al. CD8+ T cell responses in COVID-19 convalescent individuals target conserved epitopes from multiple prominent SARS-CoV-2 circulating variants. medRxiv. 2021. doi:10.1093/ofid/ofab143
- Goel RR, Painter MM, Apostolidis SA, et al. mRNA vaccines induce durable immune memory to SARS-CoV-2 and variants of concern. Science. 2021;374(6572):abm0829. doi:10.1126/science.abm0829
- World Health Organization. COVID 19 vaccines; 2021.
- Andrews N, Tessier E, Stowe J, et al. Vaccine effectiveness and duration of protection of comirnaty, vaxzevria and spikevax against mild and severe COVID-19 in the UK. medrxiv. 2021. doi:10.1101/2021.09.15.21263583
- Ranzani OT, Dos Santos Leite R, Castilho LD, et al. Vaccine effectiveness of Ad26. COV2. S against symptomatic COVID-19 and clinical outcomes in Brazil: a test-negative study design. medRxiv. 2021. doi:10.1101/2021.10.15.21265006
- Cele S, Jackson L, Khoury DS, et al. SARS-CoV-2 Omicron has extensive but incomplete escape of Pfizer BNT162b2 elicited neutralization and requires ACE2 for infection. medRxiv. 2021. doi:10.1101/2021.12.08.21267417
- Lu L, Mok BW-Y, Chen L, et al. Neutralization of SARS-CoV-2 Omicron variant by sera from BNT162b2 or Coronavac vaccine recipients. medRxiv. 2021. doi:10.1101/2021.12.13.21267668
- Jordan SC, Shin B-H, Gadsden T-AM, et al. T cell immune responses to SARS-CoV-2 and variants of concern (Alpha and Delta) in infected and vaccinated individuals. Cell Mol Immunol. 2021;18(11):2554–2556. doi:10.1038/s41423-021-00767-9
- Geers D, Shamier MC, Bogers S, et al. SARS-CoV-2 variants of concern partially escape humoral but not T cell responses in COVID-19 convalescent donors and vaccine recipients. Sci Immunol. 2021;6(59):eabj1750. doi:10.1126/sciimmunol.abj1750
- Barouch DH, Stephenson KE, Sadoff J, et al. Durable humoral and cellular immune responses 8 months after Ad26. COV2. S vaccination. N Engl J Med. 2021;385(10):951–953. doi:10.1056/NEJMc2108829
- Li Q, Nie J, Wu J, et al. SARS-CoV-2 501Y. V2 variants lack higher infectivity but do have immune escape. Cell. 2021;184(9):2362–2371. doi:10.1016/j.cell.2021.02.042
- Garcia-Beltran WF, Lam EC, Denis KS, et al. Multiple SARS-CoV-2 variants escape neutralization by vaccine-induced humoral immunity. Cell. 2021;184(9):2372–83. e9. doi:10.1016/j.cell.2021.03.013
- Collie S, Champion J, Moultrie H, et al. Effectiveness of BNT162b2 vaccine against omicron variant in South Africa. N Engl J Med. 2021;386(5):494–6.
- Basile K, Rockett RJ, McPhie K, et al. Improved neutralization of the SARS-CoV-2 Omicron variant after Pfizer-BioNTech BNT162b2 COVID-19 vaccine boosting. bioRxiv. 2021. doi:10.1101/2021.12.12.472252
- Gruell H, Vanshylla K, Tober-Lau P, et al. mRNA booster immunization elicits potent neutralizing serum activity against the SARS-CoV-2 Omicron variant. Nat Med. 2021;28:1–4.
- Hansen CH, Schelde AB, Moustsen-Helms IR, et al. Vaccine effectiveness against SARS-CoV-2 infection with the Omicron or Delta variants following a two-dose or booster BNT162b2 or mRNA-1273 vaccination series: a Danish cohort study. medRxiv. 2021. doi:10.1101/2021.12.20.21267966
- Arien KK, Heyndrickx L, Michiels J, et al. Three doses of the BNT162b2 vaccine confer neutralising antibody capacity against the SARS-CoV-2 B. 1.1. 529 (Omicron) variant of concern. medRxiv. 2021. doi:10.1101/2021.12.23.21268316
- Hoffmann M, Krüger N, Schulz S, et al. The Omicron variant is highly resistant against antibody-mediated neutralization–implications for control of the COVID-19 pandemic. Cell. 2021;185(3):447–456.
- Stamatopoulou M, Tsamadias V, Theodosopoulos T, et al. Rapid decay of anti-SARS-CoV-2 antibodies in infection-naïve healthcare workers four months after vaccination. Germs. 2021;11(4):625. doi:10.18683/germs.2021.1300
- Dulovic A, Kessel B, Harries M, et al. Comparative magnitude and persistence of SARS-CoV-2 vaccination responses on a population level in Germany. medRxiv. 2021. doi:10.1101/2021.12.01.21266960
- Yu X, Wei D, Xu W, et al. Reduced sensitivity of SARS-CoV-2 Omicron variant to booster-enhanced neutralization. medRxiv. 2021. doi:10.1101/2021.12.17.21267961
- Dyer O. Covid-19: south Africa’s surge in cases deepens alarm over omicron variant. BMJ. 2021:n3013. doi:10.1136/bmj.n3013
- Streinu-Cercel A, Săndulescu O, Miron VD, et al. Undetected Omicron transmission in Romania—Report of the first detected case of locally acquired omicron infection and complete epidemiological investigation. Diagnostics. 2022;12(2):348. doi:10.3390/diagnostics12020348
- World Health Organization. COVID-19 situation in the WHO European Region; 2022.
- Nishiura H, Ito K, Anzai A, et al. Relative reproduction number of SARS-CoV-2 Omicron (B. 1.1. 529) compared with Delta variant in South Africa. J Clin Med. 2022;11(1):30. doi:10.3390/jcm11010030
- Mahase E. Covid-19: hospital admission 50-70% less likely with omicron than delta, but transmission a major concern. British Medical Journal Publishing Group; 2021.
- Yang T-J, Yu P-Y, Chang Y-C, et al. Impacts on the structure-function relationship of SARS-CoV-2 spike by B. 1.1. 7 mutations; bioRxiv. 2021. doi:10.1101/2021.05.11.443686
- Leung K, Shum MH, Leung GM, et al. Early transmissibility assessment of the N501Y mutant strains of SARS-CoV-2 in the United Kingdom, October to November 2020. Eurosurveillance. 2021;26(1):2002106. doi:10.2807/1560-7917.ES.2020.26.1.2002106
- Zuckerman NS, Fleishon S, Bucris E, et al. A unique SARS-CoV-2 spike protein P681H strain detected in Israel. medRxiv. 2021. doi:10.1101/2021.08.21.21262393
- Zahradník J, Marciano S, Shemesh M, et al. SARS-CoV-2 variant prediction and antiviral drug design are enabled by RBD in vitro evolution. Nat Microbiol. 2021;6(9):1188–1198. doi:10.1038/s41564-021-00954-4
- Callaway E, Ledford H. How bad is Omicron? What scientists know so far. Nature. 2021;600(7888):197–199. doi:10.1038/d41586-021-03614-z
- Herb Scribner. “Doctor reveals new nightly omicron variant symptom”. Deseret News; 2021.
- Ferguson N, Ghani A, Cori A, et al. Report 49: growth, population distribution and immune escape of Omicron in England. Imperial College London; 2021.
- Lewnard JA, Hong VX, Patel MM, et al. Clinical outcomes among patients infected with Omicron (B. 1.1. 529) SARS-CoV-2 variant in southern California. medRxiv. 2022. doi:10.1101/2022.01.11.22269045
- Leonhardt D. “Omicron is Milder”. The New York Times; 2022.
- Kahn F, Bonander C, Moghaddassi M, et al. Risk of severe COVID-19 from the Delta and Omicron variants in relation to vaccination status, sex, age and comorbidities: surveillance results from southern Sweden. medRxiv. 2022. doi:10.2807/1560-7917.ES.2022.27.9.2200121
- Scott L, Hsiao N-Y, Moyo S, et al. Track Omicron’s spread with molecular data. Science. 2021;374(6574):1454–1455. doi:10.1126/science.abn4543
- Metzger CM, Lienhard R, Seth-Smith HM, et al. PCR performance in the SARS-CoV-2 Omicron variant of concern? Swiss Med Wkly. 2021;49:w30120.
- Bal A, Destras G, Gaymard A, et al. Two-step strategy for the identification of SARS-CoV-2 variant of concern 202012/01 and other variants with spike deletion H69–V70, France, August to December 2020. Eurosurveillance. 2021;26(3):2100008. doi:10.2807/1560-7917.ES.2021.26.3.2100008
- Connor Parker. Government scientists monitoring new BA.2 variant of Omicron. Yahoo News; January 21, 2022.
- Farooqi T, Malik JA, Mulla AH, et al. An overview of SARS-COV-2 epidemiology, mutant variants, vaccines, and management strategies. J Infect Public Health. 2021;14(10):1299–1312. doi:10.1016/j.jiph.2021.08.014
- FDA. Coronavirus (COVID-19) Update: FDA limits use of certain monoclonal antibodies to treat COVID-19 due to the Omicron variant; Janaury, 2022.
- Miguez-Rey E, Choi D, Kim S, et al. Monoclonal antibody therapies in the management of SARS-CoV-2 infection. Expert Opin Investig Drugs. 2022;31:1–18.
- FDA. FDA Roundup: February 25, 2022; February 25, 2022.
- Miron VD. COVID-19 in the pediatric population and parental perceptions. Germs. 2020;10(4):294. doi:10.18683/germs.2020.1220
- Malik JA, Ahmed S, Mir A, et al. The SARS-CoV-2 mutation versus vaccine effectiveness: new opportunities to new challenges. J Infect Public Health. 2022;15(2):228–240. doi:10.1016/j.jiph.2021.12.014
- Alkandari D, Herbert JA, Alkhalaf MA, et al. SARS-CoV-2 vaccines: fast track versus efficacy. Lancet Microbe. 2021;2(3):e89–e90. doi:10.1016/S2666-5247(21)00034-3
- Kim JH, Marks F, Clemens JD. Looking beyond COVID-19 vaccine Phase 3 trials. Nat Med. 2021;27(2):205–211. doi:10.1038/s41591-021-01230-y
- Haveri A, Solastie A, Ekström N, et al. Neutralizing antibodies to SARS-CoV-2 Omicron variant after 3rd mRNA vaccination in health care workers and elderly subjects and response to a single dose in previously infected adults. medRxiv. 2021. doi:10.1101/2021.12.22.21268273
- Malik JA, Mulla AH, Farooqi T, et al. Targets and strategies for vaccine development against SARS-CoV-2. Biomed Pharmacother. 2021;137:111254. doi:10.1016/j.biopha.2021.111254