
Abstract
Background
Tsukamurella is an environmental saprophyte that potentially causes various infections in humans. It has been reported to cause rare opportunistic infections in immunocompromised patients or patients with indwelling foreign bodies.
Case Presentation
We report a case of continuous ambulatory peritoneal dialysis (CAPD)-related peritonitis caused by Tsukamurella inchonensis (T. inchonensis). The patient was admitted to our hospital while demonstrating a cloudy peritoneal dialysate. Peritoneal fluid sample culturing yielded yellow-greyish, dry and membrane-like colonies. Gram staining showed straight, gram-positive rods. The organism was identified to be Tsukamurella species by matrix-assisted laser desorption/ionization-time of flight mass spectrometry (MALDI-TOF MS). It was then characterized to be homologous to T. inchonensis in the GenBank database by 16S Ribosomal RNA Sequencing. The strain was susceptible to quinolones, carbapenems and linezolid, but intermediately resistant to vancomycin in drug susceptibility testing. Eventually, the peritonitis was controlled with meropenem and the patient discharged from the hospital.
Conclusion
Here, we describe the first case of CAPD-related peritonitis caused by T. inchonensis in China. Importantly, T. inchonensis show resistance to cephalosporins and heterogeneous resistance to vancomycin, guideline-based empiric therapy occasionally fails. Further analyses of similar cases are required to understand the characteristics and formulate appropriate therapy regimen for T. inchonensis infections.
Introduction
Tsukamurella species are gram-positive, weakly acid-fast bacilli bacterium belonging to the Actinomycetes family.Citation1 Tsukamurella can be isolated from soil, arthropods, water, sludge foam and sponges. The organism share many common features with Corynebacterium, Rhodococcus, Nocardia and some nontuberculous Mycobacteria species in their morphological and biochemical properties.Citation2 Traditional phenotypic methods and commercial kits which could identify most commonly encountered bacterial species in clinical microbiology laboratories, often fail to distinguish Tsukamurella from related genera.Citation3 So that molecular methods are required for Tsukamurella identification.
As opportunistic pathogens for humans, Tsukamurella can spread through clinical instruments and infect immunocompromised patients. The spectra of Tsukamurella infections comprise pulmonary infections,Citation4–7 cutaneous infections,Citation8 bacteremia,Citation9–11 meningitis,Citation12 conjunctivitisCitation13 and peritonitis.Citation14,Citation15
Bacterial peritonitis remains a main cause of fatal complications in patients undergoing continuous ambulatory peritoneal dialysis (CAPD). The empiric treatment of bacterial peritonitis should include two types of antibiotics to cover both gram-positive and gram-negative bacteria.Citation16 However, T. inchonensis infection is rare. According to the existing literature reports, T. inchonensis shows resistance to cephalosporin and heterogeneous resistance to vancomycin, which is usually an empiric antibiotic regimen for peritonitis.Citation17–19 In this article, we provide a case of CAPD-related peritonitis caused by T. inchonensis, which is the first report in China.
Case Report
A 34-year-old Chinese male who had received 3 years of continuous ambulatory peritoneal dialysis (CAPD) therapy was admitted to our hospital with complaints of abdominal pain and vomiting. He has been diagnosed as having type 1 diabetes mellitus for 15 years and received conservative treatment, including treatments with insulin injection and antihypertensive drugs. Unfortunately, diabetic nephropathy gradually progressed, and he began receiving CAPD for end-stage renal disease at 31 years old. One month prior to hospitalization, the patient had frequent diarrhea which was relieved by norfloxacin (0.1g, every day, P.O.). One day prior to admission, he developed abdominal pain, vomiting but afebrile, followed by a cloudy peritoneal dialysate on the day of admission.
Laboratory investigation revealed white blood cell count of 6.76×103/ul, C-reactive protein (CRP) 44.67 mg/L (0–10 mg/L), and procalcitonin 4.96 ng/mL (0–0.5 ng/mL). The peritoneal dialysate was cloudy, and microscopic examination showed a concentration of 5.45×103 cells/ul with 87.5% of neutrophils. In addition, gram-positive rods were detected in the peritoneal dialysis fluid cultures, suggesting the development of CAPD-related peritonitis.
Peritonitis remains one of the most serious and life-threatening complications of CAPD. It is closely related to permanent peritoneal membrane damage, as well as to the necessity of catheter removal and conversion to hemodialysis. So, the patient was treated empirically with meropenem (1g, every 12 h, i.p.) to resistant bacterial infection and fluconazole (100mg, every day, P.O.) to prevent fungal infections. According to the International Society of Peritoneal Dialysis (ISPD) guidelines in 2016, the Committee recommended that vancomycin should preferably be administered intermittently (in one exchange every 5–7 days) and not continuously (in every exchange).Citation16 In our case, the dosage and frequency of vancomycin was also administered empirically and based on clinical experience (2g, i.p. on day 1, day 4, day 9 and day 18). After 5 days of antibiotic treatment, the peritoneal dialysis fluid was clear and the white blood cells count recovered to 67 cells/ul with 6% of neutrophils. On the 18th hospital day, the patient was uneventfully discharged after a full course of antimicrobial therapy.
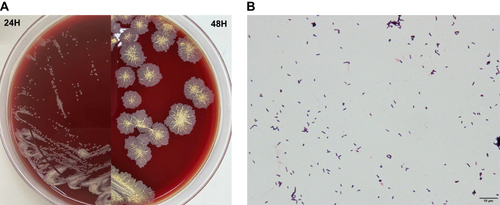
As described above, the peritoneal dialysate cultures were positive in aerobic bottles of the Bact/Alert 3D system (bioMérieux, France) after 29.2h of incubation. Anaerobic cultures were negative after 5 days of incubation. The specimens from the positive bottles were plated onto Columbia blood plate medium and incubated at 35°C in 5% CO2 chamber. After 48h of incubation, odourless, yellow-greyish, dry and membrane-like colonies were observed on blood agar (). Gram staining showed straight, gram-positive rods ().
Figure 1 Colonial appearance and gram staining of T. inchonensis. (A) Colonial appearance of T. inchonensis on a Columbia blood agar plate after 24h and 48h of incubation; (B) Gram staining (bioMérieux, SA) of T. inchonensis isolated from peritoneal dialysate cultures (×1000).
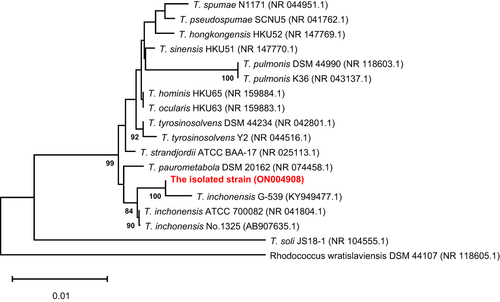
The isolated strain was identified as Tsukamurella species by MALDI-TOF MS with a confidence level of 99.9% (). Further identification was carried out by 16S rRNA gene sequencing. We performed PCR sequencing for 16S rRNA using the forward primer 27F (5’-AGAGTTTGATCATGGCTCAG-3’) and the reverse primer 1492R (5’-TACGGCTACCTTGTACGACTT-3’). The sequence were compared with the 16S rRNA gene sequence of known bacteria in the GenBank database. The concordance rates were as follows: T. inchonensis ATCC700082, 100% (1381/1381 bps); T. inchonensis G-53 KY949477.1100% (1381/1381 bps). By constructing a phylogenetic tree, we found that the isolate was located in the same branch as T. inchonensis (). The nucleotide data were registered in the NCBI database with accession numbers of ON004908 (16S ribosomal RNA).
Figure 2 Mass spectra of the bacterial isolate. The isolate strain was identified by VITEK-MS.
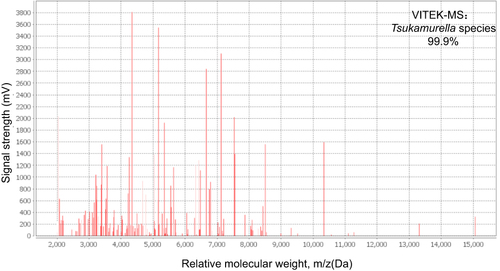
Figure 3 Phylogenetic trees presenting the relationship between the isolated strain with Tsukamurella strains. The evolutionary history was inferred using the neighbor-joining method. The isolated strain was marked in red. Evolutionary analyses were conducted in MEGA11.
An anti-microbial susceptibility test was performed using dry plate broth microdilution panels. We used cation-adjusted Mueller Hinton Broth and cultured for 24 hours under 35°C ambient condition. Minimum inhibitory concentrations (MICs) of the tested antimicrobials are shown in . The susceptibilities were interpreted by the criteria established by the Clinical and Laboratory Standards Institute (CLSI), referring to the criteria for Nocardia species.Citation20 The strain was sensitive to imipenem, ciprofloxacin, levofloxacin, moxifloxacin and linezolid, but resistant to SXT. However, T. inchonensis isolated from our case show intermediate-level resistance to vancomycin and resistance to cephalosporins, which is usually an empiric antibiotic regimen for peritonitis.
Table 1 Minimum Inhibitory Concentrations (MIC) of Tsukamurella inchonensis Isolated in This Case and Previous Literature
Discussion
Tsukamurella is a bacterial genus of dry, yellow-greyish and gram-positive rods that have been cultured from blood, conjunctival swab, lung and other clinical specimens for the last several decades.Citation21 This organism is difficult to identify and has been misidentified as Corynebacterium and atypical Mycobacteria, so that molecular methods are necessary for the accurate identification. MALDI-TOF MS, as a rapid and accurate method for the identification of bacterial and fungal pathogens, has been widely used in clinical microbiology laboratories. In our case, identification of Tsukamurella is limited to genus-level using MALDI-TOF MS. Differentiation of Tsukamurella from other related genera and species identification within these genera are difficult, as they share similar phenotypic properties. So, 16S rRNA gene sequencing was needed to identify the organism to accurate species-level. However, identification by sequencing is still beyond the reach of many routine clinical laboratories. MALDI-TOF MS, as a cost-effective and user-friendly method, still should be useful for routine species identification of Tsukamurella in clinical microbiology laboratories after optimization of the database by adding reference mass spectrum profiles of all the known Tsukamurella species.Citation22
Tsukamurella infection is not routine and most cases have been reported in immunocompromised patients, malignant tumor patients or patients with indwelling foreign bodies. To data, there are only four previous reports of the T. inchonensis infection. The organism was first isolated from bloodstream infection in a South Korea patient who ingested hydrochloric acid.Citation19 Then, a case of catheter-related bloodstream infection by T. inchonensis in a Japanese patient after bone marrow transplantation was reported.Citation17 Additionally, the organism was detected in a 14-year-old Japanese patient with Hodgkin’s lymphoma who developed T. inchonensis bacteremia, which was associated with the peripherally inserted central venous catheter.Citation23 T. inchonensis bacteremia complicated with septic pulmonary emboli was also reported in a Japanese woman with tongue cancer who underwent peripheral insertion of the central catheter and radiation therapy.Citation18 To our knowledge, this case is the fifth report globally and the first report of CAPD-related peritonitis caused by T. inchonensis.
The rate of gram-positive rod infection has increased over the past few years and it is closely related to repeat and relapsing peritonitis, hospitalization, permanent catheter loss, transfer to hemodialysis and even death, the Committee suggests that it should be treated with proper antibiotics for 3 weeks as in Staphylococcus aureus peritonitis based on the 2016 ISPD guidelines.Citation16 Vancomycin or a first-generation cephalosporin plus a third-generation cephalosporin or an aminoglycoside remains the recommended combination in order to cover for both gram-positive and gram-negative organisms.Citation16 However, according to previous studies, Tsukamurella species are resistant to penicillins and cephalosporins, and possibly susceptible to macrolides, aminoglycosides, fluoroquinolones and carbapenems.Citation21 In our report, T. inchonensis showed sensitivity to fluoroquinolones and carbapenems and intermediate-level resistance to vancomycin. We successfully treated the patient with meropenem. Additionally, different Tsukamurella species present variable anti-microbial susceptibility.Citation24 So, 16S rRNA gene sequencing or MALDI-TOF MS equipped with optimization of the database is needed to identify the organism to accurate species-level.
Conclusion
In conclusion, we described a case of CAPD-related peritonitis caused by T. inchonensis, in which the bacteria was identified by 16S rRNA gene sequencing. Importantly, T. inchonensis show resistance to cephalosporins and heterogeneous resistance to vancomycin, guideline-based empiric therapy occasionally fails. Further analyses of similar cases are required to understand the characteristics and formulate appropriate therapy regimen for T. inchonensis infections.
Ethics Approval and Consent to Participate
This report complies with the guidelines for human studies and is in accordance with the Declaration of Helsinki. All clinical data of the patient were collected in accordance with the Local Research Ethics committee of the First Affiliated Hospital of Anhui Medical University (Quick-PJ 2022-03-21).
Informed Consent for Publication
Written informed consent was obtained from the patient for the publication. The patient provided written informed consent to participate in this study.
Disclosure
The authors have no conflicts of interest to declare in this work.
Additional information
Funding
References
- Stackebrandt E, Rainey FA, Ward-Rainey NL. Proposal for a new hierarchic classification system, actinobacteria classis nov. Int J Syst Bacteriol. 1997;47(2):479–491. doi:10.1099/00207713-47-2-479
- Kattar MM, Cookson BT, Carlson LC, et al. Tsukamurella strandjordae sp. nov., a proposed new species causing sepsis. J Clin Microbiol. 2001;39(4):1467. doi:10.1128/JCM.39.4.1467-1476.2001
- Alcaide ML, Espinoza L, Abbo L. Cavitary pneumonia secondary to Tsukamurella in an AIDS patient. First case and a review of the literature. J Infect. 2004;49(1):17–19. doi:10.1016/S0163-4453(03)00139-7
- Chen CH, Lee CT, Chang TC. Tsukamurella tyrosinosolvens bacteremia with coinfection of Mycobacterium bovis pneumonia: case report and literature review. Springerplus. 2016;5(1):2033. doi:10.1186/s40064-016-3707-y
- Roger M. First case report of community-acquired pneumonia due to Tsukamurella pulmonis. Ann Intern Med. 2009;150(2):147–148. doi:10.7326/0003-4819-150-2-200901200-00022
- Ménard A, Khasakhala LI, Kuria MW, et al. Tsukamurella tyrosinosolvens - An unusual case report of bacteremic pneumonia after lung transplantation. Ann Gen Psychiatry. 2009;8(1):1–5. doi:10.1186/1744-859X-8-1
- Mehta YB, Simonelli P, Goswami R, et al. Tsukamurella infection: a rare cause of community-acquired pneumonia. Am J Med Sci. 2011;341(6):500–503. doi:10.1097/MAJ.0b013e3182129d02
- Granel F, Lozniewski A, Barbaud A, et al. Cutaneous infection caused by Tsukamurella paurometabolum. Clin Infect Dis. 1996;4:839.
- Elshibly S, Doherty J, Xu J, et al. Central line-related bacteraemia due to Tsukamurella tyrosinosolvens in a haematology patient. Ulst Med J. 2005;74(1):43–46.
- Schwartz MA, Tabet SR, Collier AC, et al. Central venous catheter–related bacteremia due to Tsukamurella species in the immunocompromised host: a case series and review of the literature. Clin Infect Dis. 2002;35(7):908.
- Shapiro CL, Haft RF, Gantz NM, et al. Tsukamurella paurometabolum: a novel pathogen causing catheter-related bacteremia in patients with cancer. Clin Infect Dis. 1992;14(1):200–203. doi:10.1093/clinids/14.1.200
- Prinz G, Bán E, Fekete S, et al. Meningitis caused by Gordona aurantiaca (Rhodococcus aurantiacus). J Clin Microbiol. 1985;22(3):472–474. doi:10.1128/jcm.22.3.472-474.1985
- Kechker P, Senderovich Y, Ken-Dror S, et al. Tsukamurella pulmonis conjunctivitis in patients with an underlying nasolacrimal duct obstruction - report of two cases. Access Microbiol. 2021;3(2):000185. doi:10.1099/acmi.0.000185
- Shaer AJ, Gadegbeku CA. Tsukamurella peritonitis associated with continuous ambulatory peritoneal dialysis. Clin Nephrol. 2001;56(3):241–246.
- Ismayilov R, Duran ZC, Hazirolan G, et al. Tsukamurella paurometabola peritonitis in a patient on automated peritoneal dialysis. Enferm Infecc Microbiol Clin. 2021;39(8):422. doi:10.1016/j.eimc.2020.10.010
- Liakopoulos V, Nikitidou O, Kalathas T, et al. Peritoneal dialysis-related infections recommendations: 2016 update. What is new? Int Urol Nephrol. 2017;49(12):2177–2184. doi:10.1007/s11255-017-1632-9
- Takebe I, Sawabe E, Ohkusu K, et al. Catheter-related bloodstream infection by Tsukamurella inchonensis in an immunocompromised patient. J Clin Microbiol. 2014;52(6):2251–2253. doi:10.1128/JCM.00421-14
- Gotoh K, Mayura IPB, Hagiya H, et al. Septic pulmonary emboli caused by Tsukamurella inchonensis: a case report. J Infect Chemother. 2020;27(2):369–372. doi:10.1016/j.jiac.2020.09.024
- Chong Y, Lee K, Chon CY, et al. Tsukamurella inchonensis bacteremia in a patient who ingested Hydrochloric acid. Clin Infect Dis. 1997;24(6):1267–1268. doi:10.1093/clinids/24.6.1267
- Woods G, Lin SY, Desmond EP. Susceptibility testing of Mycobacteria, Nocardiae, and other aerobic actinomycetes. Approved Standard M24-A2. Man Clin Microbiol. 2011;31:1356–1378.
- Safaei S, Fatahi-Bafghi M, Pouresmaeil O. Role of Tsukamurella species in human infections: the first literature review. New Microbes New Infect. 2018;22(C):6–12. doi:10.1016/j.nmni.2017.10.002
- Teng JLL, Tang Y, Wong SSY, et al. MALDI-TOF MS for identification of Tsukamurella species: Tsukamurella tyrosinosolvens as the predominant species associated with ocular infections. Emerg Microbes Infect. 2018;7(1):80. doi:10.1038/s41426-018-0083-4
- Ochi F, Tauchi H, Moritani K, et al. Tsukamurella inchonensis infection in a child with Hodgkin’s lymphoma. Pediatr Int. 2015;57(1):e7–e10. doi:10.1111/ped.12472
- Liu CY, Lai C-C, Lee M-R, et al. Clinical characteristics of infections caused by Tsukamurella spp. and antimicrobial susceptibilities of the isolates. Int J Antimicrob Agents. 2011;38(6):534–537. doi:10.1016/j.ijantimicag.2011.07.018