Abstract
Group C Streptococcus (GCS) is a rare cause of bacteremia in humans. It is mostly associated with zoonological infections. Although GCS can be part of the normal oral, skin, and genitourinary fora, an infection with this pathogen can be highly virulent, causing rapid, disseminating disease. With a mortality of about 25%, the poor prognosis is linked to the severity of illness and the high level of virulence of the organism. Only a few cases of GCS meningitis have been reported. We present the first case of GCS meningitis with cavernous sinus thrombosis.
Case report
An eighteen year old African American male presented to the emergency room with a 1-week history of sore throat, muscle aches, fever, headache, and photophobia. He also complained of nausea, one episode of vomiting, and abdominal pain. He was a college student and lived in a dormitory. He denied any recent travel or contact with ill people. Past medical history was significant for sickle cell trait and Osgood Schlatter’s disease. He was up to date on vaccinations.
Physical examination revealed a tall, thinly built young man, in mild pain with an oral temperature of 97.5°F, blood pressure of 114/69 mmHg, heart rate of 89 beats per minute (BPM) and respirations of 18/minute. He had injected conjunctiva of the right eye, and pharyngeal and tonsillar exudates. The examination of the central nervous system revealed neck stiffness; Kernig’s and Brudzinski’s signs were not elicited. Cranial nerves were intact. The power and deep tendon reflexes were essentially normal. The rest of the systemic examinations were unremarkable.
Hemoglobin was 17.5 g/dL, hematocrit 50.8 g/dL, and white count 20.3 × 109/L with 89% granulocytosis, and platelet count of 35 × 109/L. Basic metabolic profile was within normal limits, except for a potassium level of 3.2 meq/L, blood urea nitrogen of 44.9 mg/dL, and creatinine of 2.3 mg/dL. Chest X-ray revealed bilateral infiltrates in the middle and lower lung fields. Computed tomography (CT) of the head was unremarkable. The patient declined lumbar puncture. The blood culture grew penicillin sensitive Group C Streptococcus (GCS) within 24 hours of incubation. A few hours into the admission, he developed third and sixth nerve palsy. Further work-up revealed right cavernous and ophthalmic vein thrombosis on magnetic resonance imaging ( and ). Multiple patchy cavitary lesions on both lungs were seen in the chest CT. There was no vegetation on transesophageal echocardiogram. The oculomotor and abducens palsies resolved after medical management for 16 days.
Figure 1 A band of enhancement measuring 6 mm in thickness is seen along the medial margin of the right temporal convexity (arrow #2). Increased T2 signal in the region of the right cavernous sinus with diminshed enhancement is suggestive of cavernous sinus thrombosis (arrow #1).
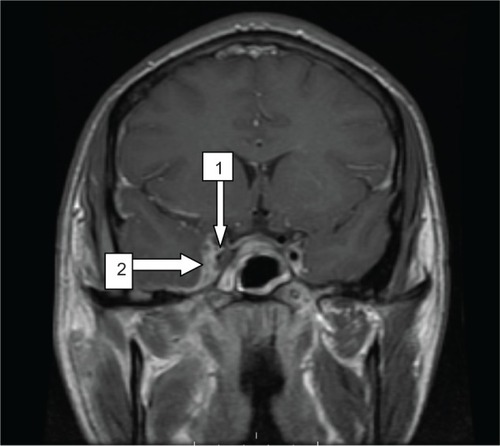
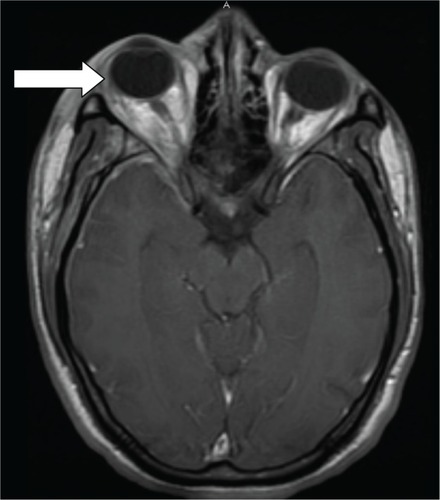
Figure 2 Right eye proptosis (arrow).
Discussion
GCS is a rare cause of bacteremia, mostly associated with zoonological infections.Citation1–Citation8 It can cause a mucopurulent pulmonary disease in horses and mastitis in cattle.Citation2,Citation3 In humans, GCS can be part of the normal oral, skin, and genitourinary flora but, GCS infection can be highly virulent, causing rapid, disseminating diseaseCitation2–Citation4 carrying with it a mortality of about 25%.Citation4,Citation5 The dismal prognosis is linked to the severity of illness and the high level of virulence of the organism.Citation2
This group of Streptococci can be differentiated from other species by their hemolysis pattern and their ability to ferment sorbitol and trehalose.Citation4 Examples of major species include Streptococcus equisimilis, S. zooepidemicus, S. equi, S. dysgalactiae, with the most common type isolated from the human throat being S. milleri.Citation1–Citation4,Citation6,Citation7 Unfortunately, one of our limitations was our laboratory was unable to identify the species of GCS. One study, which was based on the throat swabs of 1,016 college patients, showed that GCS was associated with pharyngitis.Citation3 This is significant concerning our patient as he had complained of symptoms of sore throat and had a tonsillar exudate.
Cases of virulent GCS infections are rare. GCS menigitis, though rare, has a strong association with patients who were in close contact with infected animals or consumed unpasterized milk.Citation1,Citation2,Citation6–Citation9 Huang et al reported 13 cases of GCS meningitis;Citation2 of these cases, five died, four suffered permanent neurological sequelae of some kind, and four recovered without lasting sequelae.Citation2 To the best of our knowledge, ours is the first case of GCS meningitis with cavernous sinus thrombosis. Adverse outcomes can still occur despite timely initiation of appropriate antimicrobial treatment.Citation2,Citation4,Citation5 Blood cultures taken 24 hours after starting treatment would be negative, as well as cerebrospinal-fluid analysis. This expectionally rapid eradication rate of the pathogen exists in the presence of continued fever spikes and a worsening clinical picture,Citation2 as was the case for our patient. He continued to have symptoms of fever and chills for at least 7–10 days after starting treatment.
A classic presentation of meningitis includes nuchal rigidity, fever, headache, and photophobia. However, without aggressive treatment, patients can rapidly develop more severe signs such as tetraparesis,Citation9 aortic aneurysms, osteomyelitis and lymphadenitis,Citation5 hearing loss, and blindness.Citation2,Citation4,Citation5
A possible complication of meningitis can be the development of a thrombosis in the cavernous sinus. Cavernous sinus thrombosis is the formation of a blood clot within the cavernous sinus. This is a cavity at the base of the brain which drains deoxygenated blood from the brain back to the heart. The cause is usually from a spreading infection in the nose, sinuses, ears, or teeth. S. aureus and Streptococcus are often the culpable bacteria. Cavernous sinus thrombosis symptoms include: decrease or loss of vision, chemosis, exophthalmos, headaches, and paralysis of the cranial nerves that course through the cavernous sinus, features which were observed in our patient. This infection is life-threatening and requires immediate treatment, which usually includes antibiotics and sometimes surgical drainage.
When the patient originally entered the hospital he was started on extended coverage antibiotics: ceftriaxone and vancomycin. Once the diagnosis was established, and given the history of a pencilin allergy, we decided to begin treatment with chloramphenicol, one gram intravenously, every 6 hours. He was started on dexamethasone every 4 hours for the orbital edema. Twelve to 24 hours later, the sensitivity profile showed that the pathogen was susceptible to only penicillin G. At this juncture, it was decided to desensitize the patient to pencillin. He did not suffer any ill effects of the desensitization and his antibiotic regimen was switched to intravenous penicillin G, four million units every 4 hours. Due to risk of bleeding, considering patient’s low platelet count, the decision was made to not fully anticoagulate our patient, but to manage him with 5000 units of subcutaneous heparin three times daily. Some advocate for the use of gentamicin, an aminoglycoside, with penicillin G to create a synergistic effect in severely ill patients or those who are immunocompromised.Citation10 Our patient continued this treatment regimen for 6 weeks. During these 6 weeks he developed an empyema, which had to be drained with a chest tube, likely secondary to septic emboli. After drainage, the patient did well and was discharged.
GCS infection is a rare cause of meningitis in humans. It has a high virulence and affected patients may suffer permanent neurologic sequela. Prior pharyngitis from this organism is an important risk factor. Oculomotor or abducens palsy in patients with meningitis further indicates thrombosis of the cavernous sinus since these nerves pass through the sinus. To our knowledge we have presented the first case of GCS meningitis with cavernous sinus thrombosis.
Disclosure
The authors report no conflicts of interest in this work.
References
- TurnerJCFoxAFoxKRole of group C beta-hemolytic streptococci in pharyngitis: epidemiologic study of clinical features associated with isolation of group C streptococciJ Clin Microbiol19933148088118463391
- HuangARBriedisDJGroup C streptococcal endocarditis presenting as clinical meningitis: report of a case and review of the literatureCan J Infect Dis19923524725222416199
- TurnerJCHaydenFGLoboMCRamirezCEMurrenDEpidemiologic evidence for Lancefield group C beta-hemolytic streptococci as a cause of exudative pharyngitis in college studentsJ Clin Microbiol1997351148968872
- CarmeliYRuoffKLReport of cases of and taxonomic considerations for large-colony-forming Lancefield group C streptococcal bacteremiaJ Clin Microbiol1995338211421177559958
- PoulinM FBoivinGA case of disseminated infection caused by Streptococcus equi subspecies zooepidemicusCan J Infect Dis Med Microbiol2009202596120514161
- RajasekharAClancyCJMeningitis due to group C Streptococcus: a case report and review of the literatureScand J Infect Dis201042857157820632899
- MincesLRBrownPJVeldkampPJHuman meningitis from Streptococcus equi subsp zooepidemicus acquired as zoonosesEpidemiol Infect2011139340641020492747
- MoriNGuevaraJMTilleyDHBricenoJAZuntJRMontanoSMStreptococcus equi subsp zooepidemicus meningitis in PeruJ Med Microbiol201362Pt 233533723105024
- RivasMTPascualJSesarAGroup C streptococcus meningitis: a very uncommon conditionNeurologia2008239604606 Spanish18925443
- http://www.uptodate.com[homepage on the Internet]Group C and Group G streptococcal infection Weinberg AN2013 [updated May 25, 2010]. Available from: http://www.uptodate.com/contents/group-c-and-group-g-streptococcal-infectionAccessed July 8, 2013