

Abstract
Background
First-year doctors found that during out-of-hours shifts they were being delayed and distracted from reviewing potentially sick/deteriorating patients by a high volume of prescribing tasks. This predominately consisted of oral anticoagulation prescribing and rewrites of drug charts. We hoped that if we could reduce this burden of “inappropriate prescribing tasks”, we could not only improve junior doctors’ job satisfaction and opportunities for training but also give them more time for patient reviews.
Methods
Three weekends were initially audited to quantify the number of “inappropriate prescribing tasks” using data from the hospital’s computerized task assigning system. On three subsequent weekends, a checklist was handed out to the ward teams on Friday mornings. This checklist was designed to encourage the day teams to check that drug charts would not need oral anticoagulation or rewriting over the weekend.
Results
An overall reduction in “inappropriate prescribing tasks” of 46% with a specific reduction in inappropriate oral anticoagulation prescribing of 65% was observed. Inappropriate drug chart rewrites were reduced by 30%. The reduction in the mean number of pre-intervention inappropriate prescribing tasks (as a percentage of total prescribing tasks) and the post-intervention mean was 6.94% (95% confidence interval −0.54 to 14.42, p-value=0.062).
Conclusion
Improved job satisfaction and a perceived reduced workload were noted from post-intervention qualitative surveys. While improved patient safety directly resulting from this intervention is more difficult to establish, and the observed reduction in inappropriate prescribing was only approaching statistical significance, our colleagues commented in post-intervention feedback that they felt they had more time, and felt less pressured, while attending patients. The workload of junior doctors can exert a significant effect on patient care, and simple measures can alleviate this burden. Furthermore, computerized hospital task management systems are an underutilized source of data for audit and quality improvement.
Supplementary materials
Instructions on the use of the checklist printed on its reverse
How to use this checklist
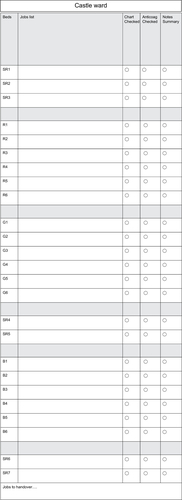
This checklist is designed to help minimize inappropriate prescribing jobs for the on-call teams over the weekend. We appreciate that Friday afternoons are usually hectic, but this checklist is designed to prompt you to do a quick round of the drug charts on the ward to check that no warfarin/Tinzaparin will need prescribing and no drug charts will need rewriting over the weekend. This chart should include your specific ward’s bed layout, and there is space for the checklist to double up as your Friday jobs list with space for any important jobs to be handed over as well. We are also trying to ensure that the patient notes, which will be used by the on-call team when they attend a potentially sick patient over the weekend, have a clearly documented ceiling of care, management plan and clinical summary.
Jobs
The ‘Jobs list’ column is to allow junior doctors space to note down tasks generated from the ward round. As a result, the checklist can act as an aide-memoire for these tasks throughout the working day on Friday and the checklist is more likely to be utilised.
Chart checklist
This box is to be ticked once it is confirmed that this patient’s chart has adequate space for nurse administration signatures over the weekend (and will therefore not need rewriting).
Anticoagulation checklist
This can be ticked once it is confirmed that this patient’s drug chart has had warfarin or therapeutic Tinzaparin prescribed (if applicable) for over the weekend.
Note summary checklist
This checklist is to serve as a reminder to check the notes of any patient, who you feel has the potential to deteriorate over the weekend. Please ensure that the last entry includes a brief clinical summary with overall management plan and a ceiling of care to aid the on-call doctors over the weekend.
Jobs to hand over
This space is for any tasks that come up during Fridays that will require handing over to on-call juniors.
Figure S1 Checklist designed to decrease inappropriate prescribing handed over to junior doctors during out-of-hours.
Acknowledgments
The authors to thank the audit and quality improvement department at South Warwickshire Foundation Trust as well as their FY1 colleagues on general medicine. They also thank Mr Richard Morrell, consultant in emergency medicine, for championing the project.
Disclosure
The authors report no conflicts of interest in this work.