
Abstract
Background
The concentration of diagnostic markers such as inflammatory biomarkers including procalcitonin (PCT) and C-reactive protein (CRP) increases in bacterial infections. The aim of this study was to compare serum PCT and CRP levels with CURB-65 ranking, in the patients with community-acquired pneumonia (CAP).
Patients and methods
In a cross-sectional study, 93 hospitalized patients with a definite diagnosis of CAP, considering inclusion and exclusion criteria, were enrolled. Serum PCT and CRP levels and their relations with CURB-65 criteria were assessed.
Results
The mean serum levels of PCT and CRP were 3.64±12.32 ng/mL and 75.01±51.93 mg/L, respectively. There was a statistically significant association between CURB-65 criteria and serum levels of PCT (P=0.0001) and CRP (P=0.007), which means that the concentration of these two inflammatory biomarkers increased with an increase in the score of CURB-65 criteria. Moreover, there was a statistically significant association between the serum level of PCT and the outcomes of the disease (P<0.001).
Conclusion
According to the results, the serum level of PCT or CRP is a strong prognostic factor for evaluating severity of CAP and is a suitable factor for the CURB-65 criteria in the decision making of whether a patient with CAP in the ICU should be admitted.
Introduction
Acute pneumonia refers to acute infection and inflammation of the lung parenchyma and various microbial agents are involved in its pathogenesis. Although pneumonia is a major cause of death and disability and is often not properly diagnosed, early treatment is usually not performed. Pneumonia is classified as community-acquired pneumonia (CAP), hospital-acquired pneumonia, and ventilator-associated pneumonia.Citation1, Citation2
The parameters such as confusion, blood urea nitrogen, respiratory rate, blood pressure, and age ≥65 years (CURB-65) were used as criteria to measure the severity of pneumonia. Many reviews and studies have been carried out to investigate the risk of mortality due to pneumonia based on these criteria; According to these criteria, clinician can make decision to treat the patients in outpatient, hospitalization, or intensive care unit (ICU) admission.Citation2,Citation3 To diagnosis pneumonia, in addition to chest radiographs, other diagnostic tests such as biological markers are used to differentiate bacterial pneumonia from non-bacterial pneumonia. The C-reactive protein (CRP) and procalcitonin (PCT) are two important biomarkers for the diagnosis of bacterial pneumonia.Citation3 PCT quickly rises in bacterial infections. It is a calcitonin peptide precursor that is released by parenchyma cells in response to bacterial toxins. So, PCT is used mainly to guide antibiotic therapy in lower respiratory tract infections and in pneumosepsis.Citation1,Citation3 Several studies show that PCT levels correlate with the severity of pneumonia and reduce in patients with pneumonia during their recovery process, but increase in their level indicates a trend toward death.Citation4–Citation6 By measuring PCT serum level, we can predict the risk of bacteremia.Citation7
Berg et al reported in a study that measuring serum level of PCT as a prognostic factor (predictor) for sense of severity of illness and mortality is more valuable than to be used as a criterion for the diagnosis of bacterial pneumonia.Citation8 Huang et al reported that PCT as a prognostic factor alongside other measures can be helpful for high-risk patients.Citation9
CRP is another inflammatory marker that can be used for the diagnosis of bacterial pneumonia, and serum level >40 mg/L in bacterial pneumonia has 70% sensitivity and 90% specificity.Citation10 In other study, 73% sensitivity and 65% specificity have been reported for CRP, in this regard.Citation11
This study aimed to compare serum levels of PCT and CRP with CURB-65 criteria to assess the outcomes of the patient with CAP.
Patients and methods
In a cross-sectional study, patients with acute CAP who were admitted to Sina hospital in Hamadan during July 2015 to March 2016 were enrolled. Huang et al conducted a study in 2008 and reported the mean (SD) serum level of PCT among patients with CAP to be 82.0 (34.3) ng/mL. Based on these results, we reached at a sample of 93 at 0.05 significant level and 0.2 error level. Inclusion criteria were as follows: patients above 15 years old with new pulmonary infiltration on chest radiography with one of the clinical symptoms including: fever, cough, purulent sputum, pleuritic pain, dyspnea, crackles, or rales in lung sound. Exclusion criteria included patients with severe immune deficiency such as people with HIV, neutropenia, cancer, long-term use of steroids, kidney transplant, as well as patients with a confirmed diagnosis of pulmonary tuberculosis and hospitalized patients in 4 weeks before infection. The protocol of this study was approved by the Ethics committee of Hamadan University of Medical Sciences (accession number: IR.UMSHA.REF.1144), and written informed consent was obtained from all individuals involved. About 5 mL of blood was taken from all the patients for measuring serum levels of CRP and PCT. All the laboratory tests were blinded without the experts having knowledge of CURB-65 parameters. Serum level of CRP was measured by using quantitative diagnostic kit (Pars Azmoon Inc., Tehran, Iran), performed with immunoturbidimetric method and Hitachi autoanalyzer at Sina hospital’s laboratory in Hamadan. The assay range of CRP was 2–30 mg/L and levels higher than 30 mg/L should be diluted with normal saline. The inter-assay precision of quantitative CRP had coefficient of variation (CV) between 4% and 5%. Serum level of PCT was measured by electrochemiluminescence immunoassay (ECLIA) using Elecsys system and Roche kit at Razi laboratory of Hamadan. The assay range of PCT was 0.02–100 ng/mL. Functional sensitivity of PCT kit was less than 0.06 ng/mL with CV of about 20%. Analytical imprecision of PCT and CRP in terms of CV was 2.7% and 5.3%, respectively, which measured sixteen replicates of one sample in one assay.
In this study, CURB-65 parameters including confusion, blood urea nitrogen >19 mg/dL (>7 mmol/L), respiratory rate of 30 breaths per minute or greater, systolic blood pressure <90 mmHg or diastolic blood pressure ≤60 mmHg, and age ≥65 years are measured for determining the severity of pneumonia, and PCT and CRP serum levels were compared at various intensities of pneumonia according to CURB-65 criteria in the patients with CAP. Number and percentage of “death in hospital stay” and “death in 30 days follow-up” are evaluated for comparison of the mortality rate of the patients with CURB-65 criteria ranking and different serum levels of PCT as investigation of outcome.
The data were collected by administering a questionnaire and comprised two parts. The first part included demographic data (age and gender), symptoms, physical examination, and chest X-ray findings, and the second part included results of laboratory tests and patient’s follow-up until 30 days after admission. For statistical analysis of the data, we used chi-square test for comparing qualitative data and analysis of variance (ANOVA) for quantitative data. In addition, we constructed receiver operating characteristic (ROC) curves to illustrate graphically the predictive ability of PCT and CRP. All analysis results were estimated using Stata 11.2 software at confidence level of 95%.
Results
Overall, 93 patients with CAP were enrolled. Our study population was in the age range of 18–94 years with the mean age of 71.49±15.21 years. Seventy-seven (73.11%) of the patients were male and 16 (26.89%) cases were female. The most common clinical manifestations were cough, purulent sputum, and fever with the rate of 93.6%, 89.36%, and 70.21%, respectively.
Seventy-three (78.5%) of the patients were hospitalized in the infectious diseases ward and the rest of them (21.5%) were admitted in the ICU ward. Around 8.51% of the patients developed complications (pleural effusion or empyema), and finally, serum levels of PCT were analyzed in 90 participants (due to the scant blood sample or laboratory error, the test was not performed for 3 patients). The mean serum level of PCT was reported to be 3.64±12.32 ng/mL (range: 0.02–100), among whom 50 (55.56 %) patients had PCT levels less than 0.5 ng/mL and 40 (44.44%) patients had PCT levels ≥0.5 ng/mL. However, the mean serum level of PCT in the patients admitted to the ICU ward was 6.87±2.81 ng/mL, but in the patients admitted to the infectious ward, it was 2.72±1.45 ng/mL. In addition, the mean serum level of PCT in the patients who died during hospitalization was 12.17±9.79 ng/mL, and in the patients, who died during 30-day follow-up, the level was 9.33±7.01 ng/mL. There was a statistically significant association between the mean of PCT level and CURB-65 criteria ranking in hospitalized patients with CAP (P<0.0001) (; ). In patients with acute CAP, the relationship between CURB-65 criteria rankings and serum levels of PCT according to hospitalization ward was also statistically significant (P=0.001).
Figure 1 Association between serum levels of CRP (red line) and PCT (blue line) with CURB-65 criteria in the patients with CAP.
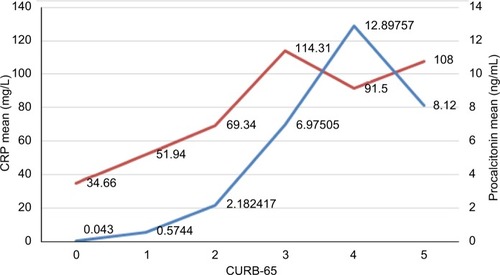
Table 1 Association between serum level of procalcitonin and CURB-65 criteria in the patients with CAP
Moreover, there was a statistically significant relationship between mortality rate among patients with acute CAP and serum levels of PCT similar to CURB-65 criteria ranking (P<0.001) ().
Table 2 Comparison of the mortality rate of the patients with CAP according to CURB-65 criteria ranking and serum levels of procalcitonin during length of hospital stay and 30-days follow-up
Serum level of CRP had been determined for eighty-six patients (CRP results were not available for 7 out of the 93 patients because of the scant blood sample or laboratory error) with the mean level of 75.01±51.93 (range: 2–180) mg/L.
There was a statistically significant relationship between the mean serum level of CRP and the CURB-65 criteria ranking in the patients with acute CAP (P=0.007) (; ).
Table 3 Association between serum level of CRP and CURB-65 criteria in the patients with CAP
In addition, a statically significant relationship was observed between the mean serum level of CRP in 67 patients who were hospitalized in the infectious ward (67.43±50.02 mg/L) and 19 patients who were admitted to the ICU ward (101.73±50.92 mg/L) (P=0.01).
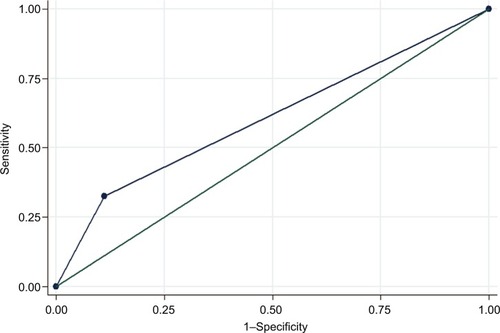
The predictive ability of PCT and CRP against CURB-65 parameters is shown in and . The area under ROC curves is over 71% and 60%, respectively, which means the predictive ability of PCT and CRP is good enough.
Figure 2 The receiver operating characteristic (ROC) curve illustrating the predictive ability of PCT against CURB-65 parameters.
Abbreviations: CURB-65; PCT, procalcitonin.
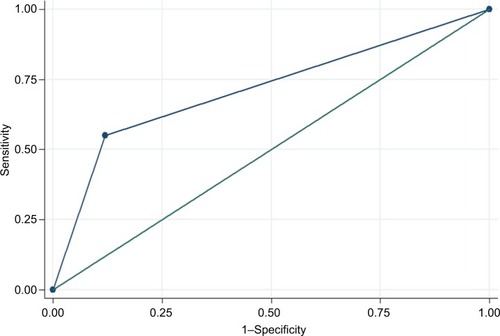
Figure 3 The receiver operating characteristic (ROC) curve illustrating the predictive ability of CRP against CURB-65 parameters.
Abbreviations: CURB-65, CRP, C-reactive protein.
Discussion
In this study, 93 patients with acute CAP and mean age of 71.49±15.21 years were enrolled, and the majority of them (73.11%) were male. In a study by Baiat-Maco et al,Citation12 which had been conducted in 2012 in Tabriz and included 70 patients with acute CAP, 61.4% of the patients were male and 38.6% were female with an average age of 65.9±14.8 (range: 16–88) years, which corresponded to the results of the present study.
In our study, the most common clinical symptoms in patients were cough, purulent sputum, and fever. Moreover, the most common chest X-ray findings in the patients were interstitial infiltration, lobar and lobular consolidation. Baiat-Maco et al’sCitation12 study reported that the most common symptoms in patients were cough, purulent sputum, fever, and shortness of breath, and the most common chest X-ray findings were found to be diffuse infiltration and consolidation, which are consistent with the present study.
For evaluation of pneumonia severity, CURB-65 criteria and biomarkers including serum levels of PCT and CRP were used, which in this study, the frequencies of ranking 0, 1, 2, 3, 4 and 5 of CURB-65 criteria, were 6.45%, 22.58%, 40.86%, 21.51%, 7.53% and 1.08%, respectively and the rank of 2 had the highest frequency. In Lim et al’sCitation13 study, these frequencies were 19%, 26%, 25.6%, 19.22%, 9.05%, and 0.9%, respectively, which were similar to our study. In a study by Ugajin et al,Citation14 frequency of ranks 0 and 1 of CURB-65 criteria were 31% in total, the rank 2 was 30%, and ranks of 3 and more were 39% in total; which is different from our study. It indicates that the patients of the present study were referred faster for hospitalization and treatment before exacerbation of disease.
The mean serum levels of PCT in our study were 3.64±12.32 ng/mL, and the values reported in studies by Baiat-Maco et al,Citation12 Kim et al,Citation15 and Lindstorm and Wong Citation16 were 4.7±1, 4.8±14.54, and 4.61±11.25 ng/mL, respectively; their values were higher than those observed in the present study and reflects the lower intensity of pneumonia in our patients than the mentioned studies because most patients in this study had second rank according to CURB-65 criteria.
In the present study, by increasing the CURB-65 ranking, the average level of PCT was increased, and the relationship between the mean serum level of PCT and CURB-65 criteria was statistically significant. This finding contradicts with the results of Baiat-Maco et al’s study,Citation12 however is consistent to the studies of Huang et al,Citation9 Kim et al,Citation15 Lindstorm and Wong,Citation16 and Walsh.Citation17 According to our findings, with an increase in the rank of CURB-65 criteria, mortality rate during hospitalization and 30-day follow-up also increased, and these findings corresponded with the results of Lim,Citation13 Huang,Citation9 and Kim.Citation15
In this study, serum levels of PCT in the patients died during hospital stay, as well as 30-days follow-up, were significantly higher than patients who were cured. Several studies have shown that in the patients with CAP, serum level of PCT correlated with the severity of pneumonia and reduced during their recovery process; however, increase in the serum PCT levels indicated a trend toward death.Citation4–Citation6 In addition, the studies of Berg et al,Citation8 Lindstormet and Wong,Citation16 Kim et al,Citation15 and Krüger et alCitation11 have reported that measuring serum level of PCT as a prognostic factor (predictor) for evaluating severity of illness and mortality is more useful than other biomarkers.
In the study by Pfister et al,Citation18 PCT has been detected as a suitable factor for rapid diagnosis of acute CAP in symptomatic patients, especially in critically ill cases. Ugajin et alCitation14 showed that high levels of serum PCT (>10 ng/mL) sharply increase the death risk. The present study showed significant correlation between serum level of PCT over 0.5 ng/mL and mortality rate during hospital stay, too. However, Baiat-Maco et alCitation12 reported no statistically significant relationship between the serum level of PCT and the outcome of illness (death or improvement) with P=0.51. Perhaps, it is due to the smaller sample size and lower CURB-65 criteria ranking of hospitalized patients in the study.
In the present study, there was statistically significant relationship between the mean serum level of CRP and the CURB-65 criteria ranking in patients with acute CAP. In a meta-analysis done by Simon et al,Citation19 it has been reported that serum levels of CRP and PCT are higher in bacterial infections than in viral infections, but the measurement of serum PCT level has higher sensitivity and specificity than CRP in the diagnosis of bacterial infection versus non-infectious or inflammatory conditions. Moreover, the accuracy of PCT in the diagnosis of bacterial infection is higher than CRP in the hospitalized patients.
In our study, the mean serum levels of PCT and CRP were significantly associated with CURB-65 criteria. In a study done by Bafadhel et al,Citation20 serum levels of CRP and PCT in 62 patients with pneumonia, 96 patients with asthma, and 161 patients with COPD were compared and reviewed. They reported that PCT and CRP serum levels in the patients with pneumonia were higher than the other two groups, and a strong correlation between CRP and PCT levels was observed. Also, they reported sensitivity of 91% and specificity of 93% for CRP levels greater than 48 mg/L for the diagnosis of pneumonia.
In the present study, the difference between mean serum level of CRP in the patients with acute CAP who were hospitalized in the ICU and infectious wards was statistically significant. Patients with CURB-65 criteria higher than 2 were hospitalized in ICU; this suggests that CRP as a prognostic factor, alongside other criteria, can be helpful in high-risk patients.
In another study by Muller et al,Citation7 conducted between 2006 and 2008 in Switzerland among 925 patients with CAP, CURB-65 criteria were compared with serum levels of CRP and PCT, and it was reported that PCT is significantly a better predictive factor in patients with pneumonia than CRP and CURB-65 criteria, and these findings corresponded with our results. Moreover, a study done by Krüger et al,Citation11 in Germany on 1671 patients with acute CAP, reported that with increasing severity of the disease according to the CURB-65 criteria, the level of biomarkers including CRP, PCT, and leukocytes also increased. In addition, 70 patients who died during 28 days of follow-up had higher levels of PCT on admission comparing to improved ones. They concluded that the serum level of PCT at admission time has the same predictive value comparing to CURB-65 criteria for calculating the severity and prognosis of disease; however, when combined with CRP might show higher accuracy of prognosis in this regard, which is consistent with our results.
In another study, Schuetz et alCitation21 reported that serum level of PCT at the time of admission has moderate prognostic information associated with the risk of death in patients and does not affect the clinical rankings, but measuring the PCT during follow-up of patients and predicting the complications may be useful and could also help in improving the ranking according to the CURB-65 criteria or pneumonia severity index. Whereas in our study, there was a significant relationship between serum level of PCT at the time of admission and CURB-65 ranking, and by increasing the ranking, serum levels of PCT and consequently the mortality rates also increased.
Conclusion
According to the findings obtained from this study, measuring the serum levels of PCT could be useful as a strong prognostic factor for the assessment of pneumonia severity and evaluating the patients with CAP. In addition, by considering that PCT and CRP levels quickly rise in bacterial infections, they are considered as the primary markers in CAP patients during infection. Using these tests can be effective in rapid evaluation and early assessment of CAP, and a good alternative to CURB-65 criteria for making clinical decisions regarding the hospitalization of the patients in the ICU ward. It should be noted that confusion, blood urea nitrogen, respiratory rate, and blood pressure, which are used for measuring severity of pneumonia, can be influenced by concomitant illness or other medications due to chronic disease, in which case measurement of PCT and CRP can be valuable in evaluating the severity of pneumonia.
Acknowledgments
The authors would like to thank Dr Maryam Adabi and the personnel of Sina Hospital laboratory for their contributions in this study. Moreover, the study was supported by the Vice-chancellor of Research and Technology, Hamadan University of Medical Sciences, Hamadan, Iran.
Disclosure
The authors report no conflicts of interest in this work.
References
- MandellLAWunderinkRGPneumoniaFauciABraunwaldEKaserDHarrison’s Internal Medicine18th edNew YorkMac Graw Hill201121302141
- MandellLAWunderinkRGAnzuetoAInfectious Diseases Society of America; American Thoracic SocietyInfectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adultsClin Infect Dis200744Suppl 2S27S7217278083
- GilbertDNProcalcitonin as a biomarker in respiratory tract infectionClin Infect Dis201152Suppl 4S346S35021460294
- BoussekeyNLeroyOAlfandariSDevosPGeorgesHGueryBProcalcitonin kinetics in the prognosis of severe community-acquired pneumoniaIntensive Care Med200632346947216477418
- MasiaMGutierrezFShumCUsefulness of procalcitonin levels in community-acquired pneumonia according to the patients outcome research team pneumonia severity indexChest200512842223222916236878
- Christ-CrainMOpalSMClinical review: the role of biomarkers in the diagnosis and management of community-acquired pneumoniaCrit Care201014120320236471
- MüllerFChrist-CrainMBregenzerTProcalcitonin levels predict bacteremia in patients with community-acquired pneumonia: a prospective cohort trialChest2010138112112920299634
- BergPLindhardtBØThe role of procalcitonin in adult patients with community-acquired pneumonia – a systematic reviewDan Med J2012593A435722381083
- HuangDTWeissfeldLAKellumJARisk prediction with pro-calcitonin and clinical rules in community-acquired pneumoniaAnn Emerg Med20085214858.e218342993
- FlandersSASteinJShochatGPerformance of a bedside C-reactive protein test in the diagnosis of community-acquired pneumonia in adults with acute coughAm J Med2004116852953515063814
- KrügerSEwigSMarreRProcalcitonin predicts patients at low risk of death from community-acquired pneumonia across all CRB-65 classesEur Respir J200831234935517959641
- Baiat-MacoJNasirzadehEKharkiANaghiliBVarshojiMAssociation between serum procalcitonin level and CURB-65 criteria among patients with acute community acquired pneumoniaThe 21st Iranian Congress on Infectious Disease and Tropical MedicineJanuary 19–23, 2013Tehran
- LimWVan der EerdenMLaingRDefining community acquired pneumonia severity on presentation to hospital: an international derivation and validation studyThorax200358537738212728155
- UgajinMYamakiKHirasawaNYagiTPredictive values of semi-quantitative procalcitonin test and common biomarkers for the clinical outcomes of community-acquired pneumoniaRespir Care201459456447324170911
- KimJHSeoJWMokJHUsefulness of plasma procalcitonin to predict severity in elderly patients with community-acquired pneumoniaTuberc Respir Dis2013745207214
- LindstromSWongEProcalcitonin, a valuable biomarker assisting clinical decision-making in the management of community-acquired pneumoniaIntern Med J201444439039724528892
- WalshEFalseyANylenESerum biomarker measurements in adults with viral respiratory infections46th Annual Meeting of Infectious Diseases Society of America (IDSA)San FranciscoOctober 25–28, 2008
- PfisterRKochanekMLeygeberTProcalcitonin for diagnosis of bacterial pneumonia in critically ill patients during 2009 H1N1 influenza pandemic: a prospective cohort study, systematic review and individual patient data meta-analysisCrit Care2014182R4424612487
- SimonLGauvinFAmreDKSaint-LouisPLacroixJSerum procalcitonin and C-reactive protein levels as markers of bacterial infection: a systematic review and meta-analysisClin Infect Dis200439220621715307030
- BafadhelMClarkTWReidCProcalcitonin and C-reactive protein in hospitalizied adult patients with community-acquired pneumonia or exacerbation of asthma or COPDChest201113961410141821030489
- SchuetzPSuter-WidmerIChaudriAChrist-CrainMZimmerliWMuellerBPrognostic value of procalcitonin in community-acquired pneumoniaEur Respir J201137238439220595156