
Abstract
Aim
The prevalence of acute myocardial infarction (AMI) is increasing in young adults, especially in men. This study aims to compare the characteristics and explore the association between age and clinical outcomes in male adults who first experienced AMI.
Methods
A total of 2737 male patients with AMI were divided into three groups by age: <50, 50–65, and ≥65 years. Clinical characteristics and long-term results (all-cause and cardiac deaths, nonfatal MI, revascularization, nonfatal stroke, cardiac rehospitalization) were identified across different age subgroups. The association between age and the outcomes was assessed by Cox proportional hazard models.
Results
This population was followed up for a median of 36.7 months. Patients <50 years had a lower prevalence of diabetes (19.4%) and previous stroke (1.8%), while they were more often to be smokers (77.1%), obese (26%), dyslipidemia (74.7%), and with the single-vessel disease (16.2%). The risk of cardiovascular and all-cause death in patients ≥65 years was higher than patients <50 years, which was noticed through competing risk regression analysis after adjusting for confounding factors (adjusted HR 3.24; 95% CI 2.26–4.22, p=0.020 for cardiovascular death, adjusted HR 4.17; 95% CI 1.91–9.10, p<0.001 for all-cause death).
Conclusion
In conclusion, although men who suffered from first AMI under the age of 50 had lower mortality, they had a higher burden of modifiable traditional risk factors. The management of modifiable lifestyles should be addressed to all young AMI patients.
Introduction
Acute myocardial infarction (AMI) remains a primary reason for morbidity and mortality globally. AMI in young populations which can lead to death in their life, resulting in a major public health crisis is not intensively investigated.Citation1 Although the prevalence of AMI has decreased in older patients, younger individuals who experience AMI have not had the same declines in cardiovascular events, especially men.Citation2 The clinical characters of AMI vary by age. Previous studies have identified that risk factors included tobacco use, obesity, and diabetes may be crucial to young individuals.Citation3–Citation5 The Framingham Heart Study had shown that the young men aged under 45 years remain adverse outcomes after present with AMI over a decade follow-up period.Citation6 Compared to the elderly, the young are not well studied about the prevalence, comorbidities, and therapies. Moreover, current studies have focused on the age of 40 or 45 years while there has not been a clear definition of young in patients with AMI.Citation7 In particular, relevant researches about Chinese men who received the percutaneous coronary intervention (PCI) are limited. Therefore, in our study, we assessed the major baseline features, angiography characteristics, treatments, and long-term follow-up in young AMI men under the age of 50 years.
Methods
Subjects
The data source was from the Cardiovascular Center of Beijing Friendship Hospital Database (CBD) Bank. A cohort of 5170 Chinese adults who were diagnosed with AMI (according to the Fourth Universal Definition of Myocardial Infarction) from January 2013 to August 2020 was included in our study. Of them, 2433 were excluded based on the following exclusion criteria: (1) female, (2) with a previous episode of AMI, (3) without coronary angiography, (4) with missing data on baseline characteristics or long-term results. Finally, we identified 2737 male patients who performed with coronary angiography in this retrospective study. Enrolled individuals were categorized into three groups based on their age: <50 years (young), 50–64 years, and ≥65 years. Individuals were followed up at 1, 3, 6 months, and each year after discharge. The median follow-up time is 36.7 (IQR: 36.3, 37.2) months.
Data Collections and Definitions
The progress of the data collected was consistent with the Declaration of Helsinki. The collection was permitted by the Institutional Review Board of Beijing Friendship Hospital affiliated to Capital Medical University.
We collected information including basic demographic data, medical histories, laboratory values, echocardiography findings, angiographic evaluations, medications at discharge and length of hospital stay from relevant medical records. Additionally, information on the type of AMI was also available for each participant. Outcome data included cardiovascular (CV) death, all-cause mortality, recurrence of MI, non-fatal stroke, rehospitalization for heart failure, and revascularization. Furthermore, causes of non-cardiovascular death were recorded in our analysis. We collected follow-up results over the telephone between trained clinicians and patients or their relatives. Outcomes were obtained via telephone follow-up.
The clinical definition of AMI was in accordance with the Fourth Universal Definition of MI during the study period.Citation8 Hypertension was defined with a raised blood pressure higher than 140/90 mmHg or treated with antihypertensive drugs. Diabetes mellitus was defined with an elevated fasting blood glucose >126 mg/dL (7.0 mmol/L) or random blood glucose >200 mg/dL (11.1 mmol/L) or previously diagnosed or treated with antidiabetic medication. Dyslipidemia was defined with an elevated low-density lipoprotein cholesterol (LDL-C) ≥ 130 mg/dL (3.3 mmol/L), total cholesterol (TC) ≥ 200 mg/dL (5.2 mmol/L), triglyceride (TG) ≥ 150 mg/dL (1.7 mmol/L) or previously diagnosed or treated with lipid-lowering drugs. The level of high-density lipoprotein cholesterol (HDL-C) lower than 40 mg/dL (1.0 mmol/L) in men or 50 mg/dL (1.3 mmol/L) in women was also defined as dyslipidemia. Body mass index (BMI) higher than 30 kg/m2 was defined as Obesity.
Transthoracic echocardiography was carried out in all individuals on admission to evaluate LVEF, left atrial (LA) diameter, left ventricular end-diastolic dimension (LVEDD), and left ventricular end-systolic dimension (LVESD). Each individual underwent coronary angiography via the radial or femoral approach, where PCI was performed after it if necessary. CV mortality was defined as heart-related death. All-cause mortality was described as death for any reason. Non-fatal stroke was described as a cerebral disorder and supported by brain CT scans or MRI detection. Cardiac rehospitalization was defined as being hospitalized due to heart failure. Revascularization was described as the unplanned restoration of blood flow for ischemic symptoms and events.
Statistical Analysis
The collected data were analyzed using the R Programming Language and SPSS version 25.0 (IBM Inc, Armonk, New York). Continuous variables were revealed as mean with standard deviation or median with interquartile range, and comparison between categories was analyzed using Student’s T-tests or Wilcoxon rank-sum test as appropriate. Categorical variables were presented as counts and percentages, and differences between groups were analyzed using the chi-square test. Gray’s test was applied to compare the independent prediction of age on CV mortality, recurrence of MI, revascularization, non-fatal stroke, cardiac rehospitalization due to the competitive risk from all-cause deaths. The competing risk regression curves were calculated for the cumulative incidence of outcomes. Covariates like patterns of AMI, left main coronary artery (LM), hypertension, diabetes, dyslipidemia, previous stroke, CKD, smoking, aspirin treatment, the peak level of NT-proBNP, the peak level of TnI, pre-PCI TIMI 0/1 flow, BMI, LVEF <50% were involved in the multivariate assessment. All p values were two-tailed, and p < 0.05 was considered statistically significant.
Results
Study Population
Baseline characteristics of all subjects in this research are presented in . In total, we recruited 2737 male patients. The mean age of the overall study population was 61 years. Of these people, 13.7% were aged younger than 50 years, 51.1% were aged 50 to 65 years, and 35.1% were aged 65 years or older. There were more patients <50 years present with STEMI than NSTEMI when compared with those aged 50–65 years and those ≥65 years.
Table 1 Baseline Clinical Characteristics of the Patients Stratified by Age
Risk Factors
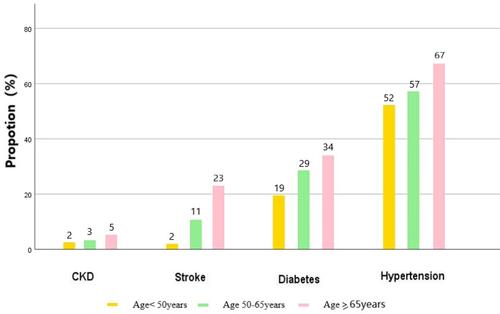
Patients <50 years presented less with diabetes mellitus and previous stroke compared with patients 50–65 years and ≥65 years, as shown in . Young men under 50 years old had fewer cardiovascular risk factors compared with the other two groups except for smoking (77.1%) and obesity (26%). Median peak troponin and CK-MB in young patients indicated that more heart muscle was affected in them. Although CK-MB and troponin levels were significantly higher in men younger than 50 years compared with those aged 50 to 65 years, the LVEF was similar between the two groups. Among men <50 years, BMI over 30kg/m2 was 26%, and LDL-C levels over 120mg/dl (3.0mmol/L) was 39% ( and ).
Figure 1 Modifiable risk factors in patients with myocardial infarction.
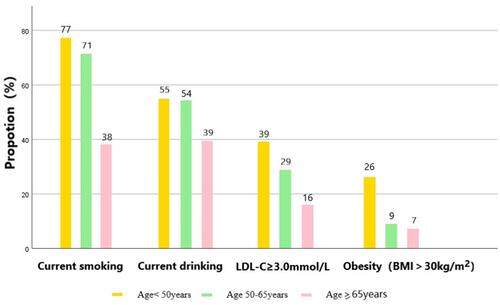
Figure 2 Unmodifiable risk factors in patients with myocardial infarction.
Angiographic Characteristics
Coronary angiographic procedures were carried out in all subjects and the findings can be found in . Single-vessel occlusion and TIMI 0/1 coronary blood flow before the percutaneous coronary intervention were more common in patients <50 years (all p < 0.001). The number of stenosed coronary arteries increased with aging (all p < 0.001). Besides, the most frequently affected coronary segment according to our study was the left anterior descending coronary artery (LAD) among the 3 groups. Those individuals under the age of 50 were less likely to be LM, LAD, left circumflex artery, and right coronary artery disease when compared with patients ≥65 years (all p < 0.001). Patients with IABP, ventilator and CABG were significantly higher in men older than 65 years compared with those aged younger than 50 years (p < 0.05).
Medications at Discharge
The median period of hospitalization was 7 days (25th, 75th percentile: 6, 9) in patients <50 years and 50–65 years, 8 days (25th, 75th percentile: 6, 11) in patients ≥65 years old (p < 0.001). Patients <50 years were significantly less likely to be discharged on calcium channel blockers (CCB, p = 0.002), and diuretics (p < 0.001) when compared with patients ≥65 years, as shown in . However, young patients received more prescriptions of beta-blockers. No differences were observed in the number of patients receiving aspirin, non-aspirin antiplatelet, ACEI or ARB, statin, and ezetimibe by age group (all p > 0.05).
Outcomes
Over a median follow-up period of 36.7 months (interquartile range: 36.3–37.2 months), there were 194 (7.1%) deaths in our cohort, representing 1.9% of patients <50 years and 13.9% of patients ≥65 years (p < 0.001). Mortality rates between patients ≥65 years (n = 134; 13.9%), 50–65 years (n = 53; 3.8%) and <50 years (n = 7; 1.9%) differed significantly. Young patients showed a more favorable outcome compared with the other two age groups. One hundred and four were dead due to cardiovascular-related causes, 53 as non-CV deaths, and 37 were undetermined. Men <50 years had a higher percentage of respiratory failure and other causes of death than the elderly ( and ).
Table 2 Causes of Death Among Patients Who Experienced Non-Cardiovascular Death
Table 3 Competing Risk Model of Outcomes
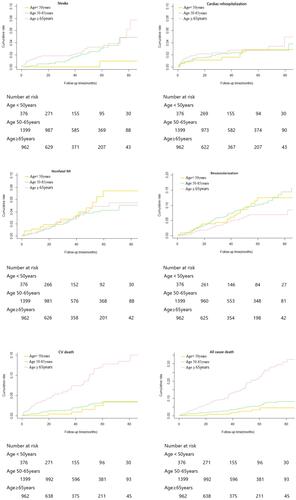
and reveal the analysis of outcomes based on competition from all-cause death. The cumulative occurrence of CV mortality, revascularization, non-fatal stroke increased significantly with elevated age groups except for recurrence of MI and rehospitalization for heart failure. After adjusting for patterns of acute myocardial infarction, hypertension, diabetes, dyslipidemia, and other confounding factors, patients ≥65 years still had a higher CV and all-cause mortality than patients <50 years. On adjusted competing risk modeling, the hazard ratio (HR) of CV death (HR = 3.24, 95% CI 2.26–4.22, Gray’s test p = 0.02) and all-cause death (HR = 4.17, 95% CI 1.91–9.10, Gray’s test p < 0.001) remaining significant.
Figure 3 Competing risk regression curves for CV death, non-fatal MI, non-fatal stroke, cardiac rehospitalization, and revascularization for the Age<50 years group (yellow line), Age 50–65 years group (green line) and Age ≥ 65 years group (pink line).
Discussion
This retrospective analysis focused on the between-group comparisons of characteristics, treatment, and outcomes of AMI according to age. About 52.1% presented with STEMI. The proportion of patients <50 years representing 13.7% of all AMI patients in our study. We observed an obvious increase in younger men presenting with modifiable cardiovascular risk factors, including smoking, drinking, and obesity which account for nearly one out of four patients. Compared with older men, younger men were less probably to be present with diabetes, previous stroke, or hypertension. Besides, men aged ≥50 years had more multi-vessel diseases. Young adults under the age of 50 had a significantly lower CV and all-cause mortality in comparison to the over 65 years group. The significant differences still exist after adjusting baseline confounders.
Although AMI in young patients is rare, the incidence of AMI in this population is increasing. A 10-year follow-up data indicated that the prevalence of AMI was higher in men than women between 30 and 55 years.Citation9 Nearly three in four young adults can experience symptoms of cardiac ischemia, which was higher in men than in women.Citation7 Similar results can be found in several studies.Citation10–Citation14 Development of AMI at a young age is correlated with multiple cardiovascular risk factors files, such as smoking, hypertension, dyslipidemia, overweight, and inactivity.Citation15 One of the most frequent causes of MI in younger individuals is plaque instability which was comparable to the old.Citation16 Modifiable risk factors include smoking, obesity, and hyperlipidemia which were most commonly observed among young subjects in our study. Bentzon et al found that the high rate of plaque rupture coexists with the population of metabolic disorders.Citation17 Smoking and hyperlipidemia are two important risk factors accounting for almost two-thirds of patients with AMI.Citation7 The number of smoking was over three quarters in young patients. Frequent exposure to cigarette smoking can result in endothelial dysfunction due to the damage of arterial cells, especially start at an early age.Citation18 Hyperlipidemia appears to be one of the most common risk factors. Several unconventional risk factors such as lipoprotein (a), inflammation, and genetic variations were also found, which may also explain some of the reasons for the early occurrence of MI.Citation19,Citation20 Our data showed that almost 40% of patients<50 years with a high level of LDL-C over 120mg/dl. Besides, nearly half of these young adults with coronary heart disease are obese.Citation21 The incidence of obesity in our study is 26%, 9%, 7% in the three age groups, respectively. The development of MI at an early age is associated with obesity which accelerated atherosclerotic progression. Increasing the prediction of BMI ≥ 25 kg/m2 on MI in younger subjects can be observed by Chen et al.Citation22 These similar observations can be found in previously reported studies.Citation23–Citation26
PCI is considered the golden criterion therapy for AMI. Angiography was performed in all patients in our study through a femoral or radial artery approach by at least two interventional cardiologists. A study including 2528 patients indicated that single vessel occlusion was observed more prevalent in patients under the age of 40 years.Citation5 Additionally, they had a lower extent of plaque and overall plaque burden than patients aged 41 to 50. According to the American Heart Association, the LAD was the most frequently affected branch of all ages. In 2019, a cohort study of the Germans discovered that less than one-third of the older patients (>40 years) had one-vessel disease compared with the younger group (≤40 years).Citation26 We found a lower prevalence of multi-vessel, LM, LAD, LCX, and RCA disease in men <50 years compared with the other two groups. In line with previous findings, the young were more frequently to have the single-vessel occlusion.Citation27,Citation28 There was an increasing tendency of diseased vessels with increasing age.Citation29 One explanation is the multi-vessel disease occurred more commonly in individuals who have a history of diabetes. In our study, the old had a higher prevalence of diabetes. We also found that the young had more TIMI 0/1 flow before PCI. The effect of coronary collateral circulation is a compensation way after the block of the normal coronary circulation.
Several previous studies have revealed a more positive prognosis in the young than the old with AMI.Citation11,Citation12,Citation30,Citation31 A study from Norway showed nearly one in ten individuals with AMI under 45 years died or underwent non-obstructive coronary artery disease during follow-up.Citation27 Thomas et al followed up 5873 patients with MI who underwent PCI for 3 years and found that the outcome of patients ≤40 years is significantly better when compared with older patients.Citation26 However, Yang et al demonstrated that very young MI patients (≤40 years) had similar one-year and longer periods results when compared to those aged 41 to 50 despite having a lower prevalence of risk factors.Citation5 A study that included 26,545 ACS patients from 2006 to 2017 revealed that subjects younger than 35 years were at significantly great risk of 30-day mortality.Citation29 In our analysis, the CV and all-cause death in AMI individuals <50 years is significantly lower than that of patients ≥65 years after adjustment for confounding factors. For death, the gap between adults aged <50 years and 50–65 years narrowed. One benefit of our study was the capability to present further assessment of non-CV death reasons. Respiratory failure and other reasons, except for cancer, sepsis, renal failure, gastrointestinal bleeding, and cerebrovascular disease were the main causes of death in young men. Patients with AMI may suffer from hemodynamic instability and fluid retention then resulting in gas exchange impairment and breathing difficulties.Citation32 In our analysis, there were fewer patients <50 years present with the pulmonary disease when compared with those aged 50–65 years and those ≥65 years. And we also found that the number of using ventilators was significantly higher in patients older than 65 years compared with those aged younger than 50 years. Despite a high survival rate, 12.5% of young men experienced one of the adverse events (non-fatal stroke, reoccurrence of MI, revascularization, or cardiac rehospitalization) during follow-up. The role of beta-blockers has been proved beneficial to prognosis. This study highlights the significance of secondary medication for coronary artery disease and the removal of modifiable risk factors in this group of patients.
One of the most common typical symptoms of AMI is acute precordial discomfort. Both atherosclerotic and non-atherosclerotic factors contributed to the development of AMI. Excessive alcohol assumption is related to chest pain, which may result in coronary occlusion due to endothelial disorder.Citation33 Besides, a growing number of young people are in the rapid pace of modern life living with depression and anxiety, especially in big cities. Compared with older individuals, frequent exposure to high stress was a positive correlation with the risk of myocardial infarction in younger adults.Citation34 In addition, systemic inflammatory reaction, hypercoagulation, and endothelial disorder may also cause MI.Citation18 The risk of mortality in young men is lower while they were more likely to have higher levels of cardiac biomarkers in our study. Early identification and appropriate treatment for AMI remain significant in young individuals. Underlying mechanisms are essential to be analyzed intensively in this population.
Limitations
Study limitations should be noted in this work. First, it is a retrospective single-center analysis within the prospectively designed which is hard to demonstrate causal associations between clinical characteristics and outcomes. Second, patients who were too ill to be hospitalized were not enrolled in this study. Those people may have different characteristics compared with the remaining patients. Third, we were unable to evaluate stress, substance abuse, or physical activity which were recognized as risk factors prevalent among young patients presenting with AMI. Fourth, the study did not continue to gather long-term follow-up data about prescribed medical therapies and risk factor modification.
Conclusions
Age differences exist in long-term prognosis, especially CV and all-cause death after myocardial infarction. Although men who suffered from first AMI under the age of 50 had lower mortality, they had a higher prevalence of modifiable risk factors and were less probably to be prescribed post-AMI medical drugs except for beta-blockers. The findings emphasize that efficient advice such as physical activity and smoking cessation should be given from public health professions and governments to all young AMI patients.
Ethics Approval and Consent to Participate
The study protocol was approved by the study institutional review board of the Beijing Friendship Hospital affiliated to Capital Medical University (No:2021-P2-307-01). All relevant guidelines were followed for the study. The requirement for informed consent from patients was waived because of its retrospective design. All methods were carried out in accordance with the ethical standards of the institutional and the Declaration of Helsinki. The patient data is confidential. Any unauthorized use or disclosure of its contents is prohibited.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Acknowledgments
The authors gratefully acknowledge the assistance with data acquisition by Dr. Guoliang Zhao.
Disclosure
All authors declare that they have no competing interests.
Additional information
Funding
References
- Karim MA, Majumder AA, Islam KQ, et al. Risk factors and in-hospital outcome of acute ST segment elevation myocardial infarction in young Bangladeshi adults. BMC Cardiovasc Disord. 2015;15:73. doi:10.1186/s12872-015-0069-2
- Gupta A, Wang Y, Spertus JA, et al. Trends in acute myocardial infarction in young patients and differences by sex and race, 2001 to 2010. J Am Coll Cardiol. 2014;64(4):337–345. doi:10.1016/j.jacc.2014.04.054
- Divakaran S, Singh A, Biery D, et al. Diabetes is associated with worse long-term outcomes in young adults after myocardial infarction: the partners YOUNG-MI registry. Diabetes Care. 2020;43(8):1843–1850. doi:10.2337/dc19-0998
- Yandrapalli S, Nabors C, Goyal A, Aronow WS, Frishman WH. Modifiable risk factors in young adults with first myocardial infarction. J Am Coll Cardiol. 2019;73(5):573–584. doi:10.1016/j.jacc.2018.10.084
- Yang J, Biery DW, Singh A, et al. Risk factors and outcomes of very young adults who experience myocardial infarction: the partners YOUNG-MI registry. Am J Med. 2020;133(5):605–612.e601. doi:10.1016/j.amjmed.2019.10.020
- Murthy NS, Nandakumar BS, Pruthvish S, George PS, Mathew A. Disability adjusted life years for cancer patients in India. Asian Pac J Cancer Prev. 2010;11(3):633–640.
- Gulati R, Behfar A, Narula J, et al. Acute myocardial infarction in young individuals. Mayo Clin Proc. 2020;95(1):136–156. doi:10.1016/j.mayocp.2019.05.001
- Thygesen K, Alpert JS, Jaffe AS, et al. Fourth universal definition of myocardial infarction (2018). J Am Coll Cardiol. 2018;72(18):2231–2264. doi:10.1016/j.jacc.2018.08.1038
- Kannel WB, Abbott RD. Incidence and prognosis of unrecognized myocardial infarction. An update on the Framingham study. N Engl J Med. 1984;311(18):1144–1147. doi:10.1056/NEJM198411013111802
- Shah N, Kelly AM, Cox N, Wong C, Soon K. Myocardial infarction in the “young”: risk factors, presentation, management and prognosis. Heart Lung Circ. 2016;25(10):955–960. doi:10.1016/j.hlc.2016.04.015
- Cole JH, Miller JI 3rd, Sperling LS, Weintraub WS. Long-term follow-up of coronary artery disease presenting in young adults. J Am Coll Cardiol. 2003;41(4):521–528. doi:10.1016/S0735-1097(02)02862-0
- Lawesson SS, Stenestrand U, Lagerqvist B, Wallentin L, Swahn E. Gender perspective on risk factors, coronary lesions and long-term outcome in young patients with ST-elevation myocardial infarction. Heart. 2010;96(6):453–459. doi:10.1136/hrt.2009.175463
- Jortveit J, Govatsmark RE, Langørgen J, et al. Gender differences in the assessment and treatment of myocardial infarction. Tidsskr nor Laegeforen. 2016;136(14–15):1215–1222. doi:10.4045/tidsskr.16.0224
- Cui Y, Hao K, Takahashi J, et al. Age-specific trends in the incidence and in-hospital mortality of acute myocardial infarction over 30 years in Japan - report from the Miyagi AMI Registry Study. Circ J. 2017;81(4):520–528. doi:10.1253/circj.CJ-16-0799
- Egred M, Viswanathan G, Davis GK. Myocardial infarction in young adults. Postgrad Med J. 2005;81(962):741–745. doi:10.1136/pgmj.2004.027532
- Naghavi M, Libby P, Falk E, et al. From vulnerable plaque to vulnerable patient: a call for new definitions and risk assessment strategies: part I. Circulation. 2003;108(14):1664–1672. doi:10.1161/01.CIR.0000087480.94275.97
- Bentzon JF, Otsuka F, Virmani R, Falk E. Mechanisms of plaque formation and rupture. Circ Res. 2014;114(12):1852–1866. doi:10.1161/CIRCRESAHA.114.302721
- van der Schoot GGF, Anthonio RL, Jessurun GAJ. Acute myocardial infarction in adolescents: reappraisal of underlying mechanisms. Neth Heart J. 2020;28(6):301–308. doi:10.1007/s12471-020-01408-y
- Wu W, Berman A, Biery D, Blankstein R. Recent trends in acute myocardial infarction among the young. Curr Opin Cardiol. 2020;35(5):524–530. doi:10.1097/HCO.0000000000000781
- Gupta M, Gupta P, Mp G, Roy A, Qamar A. Risk factors for myocardial infarction in very young South Asians. Curr Opin Endocrinol Diabetes Obes. 2020;27(2):87–94. doi:10.1097/MED.0000000000000532
- Jalowiec DA, Hill JA. Myocardial infarction in the young and in women. Cardiovasc Clin. 1989;20(1):197–206.
- Chen Y, Copeland WK, Vedanthan R, et al. Association between body mass index and cardiovascular disease mortality in east Asians and south Asians: pooled analysis of prospective data from the Asia Cohort Consortium. BMJ. 2013;347:f5446. doi:10.1136/bmj.f5446
- Misra A, Wasir JS, Vikram NK, Pandey RM, Kumar P. Cutoffs of abdominal adipose tissue compartments as measured by magnetic resonance imaging for detection of cardiovascular risk factors in apparently healthy adult Asian Indians in North India. Metab Syndr Relat Disord. 2010;8(3):243–247. doi:10.1089/met.2009.0046
- Misra A, Soares MJ, Mohan V, et al. Body fat, metabolic syndrome and hyperglycemia in South Asians. J Diabetes Complications. 2018;32(11):1068–1075. doi:10.1016/j.jdiacomp.2018.08.001
- Shih CY, Chu ML, Hsieh TC, Chen HL, Lee CW. Acute myocardial infarction among young adult men in a region with warm climate: clinical characteristics and seasonal distribution. Int J Environ Res Public Health. 2020;17(17):6140. doi:10.3390/ijerph17176140
- Wittlinger T, Seifert C, Simonis G, Gerlach M, Strasser RH. Prognosis in myocardial infarction of young patients: results of a prospective registry. Int J Cardiol. 2020;300:1–6. doi:10.1016/j.ijcard.2019.10.037
- Jortveit J, Pripp AH, Langørgen J, Halvorsen S. Incidence, risk factors and outcome of young patients with myocardial infarction. Heart. 2020;106(18):1420–1426. doi:10.1136/heartjnl-2019-316067
- Tung BW, Ng ZY, Kristanto W, et al. Characteristics and outcomes of young patients with ST segment elevation myocardial infarction undergoing primary percutaneous coronary intervention: retrospective analysis in a multiethnic Asian population. Open Heart. 2021;8(1):e001437. doi:10.1136/openhrt-2020-001437
- Qureshi W, Kakouros N, Fahed J, Rade J. Comparison of prevalence, presentation, and prognosis of acute coronary syndromes in ≤35 years, 36–54 years, and ≥ 55 years patients. Am J Cardiol. 2021;140:1–6.
- Khoury S, Soleman M, Margolis G, et al. Incidence, characteristics and outcomes in very young patients with ST segment elevation myocardial infarction. Coron Artery Dis. 2020;31(2):103–108. doi:10.1097/MCA.0000000000000779
- Yılmaz S, Coşansu K. Prognostic factors and outcomes in young patients with presented of different types acute coronary syndrome. Angiology. 2020;71(10):894–902. doi:10.1177/0003319720939444
- van Diepen S, Katz J, Albert N, et al. Contemporary management of cardiogenic shock: a scientific statement from the American heart association. Circulation. 2017;136(16):e232–e268. doi:10.1161/CIR.0000000000000525
- Mostofsky E, van der Bom JG, Mukamal KJ, et al. Risk of myocardial infarction immediately after alcohol consumption. Epidemiology. 2015;26(2):143–150. doi:10.1097/EDE.0000000000000227
- Lavie CJ, Menezes AR, De Schutter A, Milani RV, Blumenthal JA. Impact of cardiac rehabilitation and exercise training on psychological risk factors and subsequent prognosis in patients with cardiovascular disease. Can J Cardiol. 2016;32(10 Suppl 2):S365–s373. doi:10.1016/j.cjca.2016.07.508