Abstract
Objectives
To correlate cardiovascular risk factors (e.g., hypertension, obesity, hypercholesterolemia, hypertriglyceridemia, hyperglycemia, sedentariness) in childhood and adolescence with the occurrence of cardiovascular disease.
Sources
A systematic review of books and selected articles from PubMed, SciELO and Cochrane from 1992 to 2012.
Summary of findings
Risk factors for atherosclerosis are present in childhood, although cardiovascular disease arises during adulthood. This article presents the main studies that describe the importance of investigating the risk factors for cardiovascular diseases in childhood and their associations. Significant rates of hypertension, obesity, dyslipidemia, and sedentariness occur in children and adolescents. Blood pressure needs to be measured in childhood. An increase in arterial blood pressure in young people predicts hypertension in adulthood. The death rate from cardiovascular disease is lowest in children with lower cholesterol levels and in individuals who exercise regularly. In addition, there is a high prevalence of sedentariness in children and adolescents.
Conclusions
Studies involving the analysis of cardiovascular risk factors should always report the prevalence of these factors and their correlations during childhood because these factors are indispensable for identifying an at-risk population. The identification of risk factors in asymptomatic children could contribute to a decrease in cardiovascular disease, preventing such diseases as hypertension, obesity, and dyslipidemia from becoming the epidemics of this century.
Introduction
Childhood is considered the structuring period of life, during which such patterns as diet and lifestyle are formed and fixed. Although atherosclerotic disease (AD) becomes symptomatic later in life, the early identification of predisposing factors and lifestyle modifications can significantly reduce the incidence of AD.Citation1 Findings indicating that atherosclerosis begins in childhood are not new and were first presented by Saltykow in 1915 in studies involving autopsies of young patients. Atherosclerosis has been appreciated as a pediatric problem since 1965.Citation2
Coronary atherosclerosis, a disease as old as the human species, is undoubtedly the best-documented pathology.Citation3,Citation4 This process begins in early childhood, and is highly reversible at that stage.Citation5 Children usually do not develop atherosclerosis; however, they develop fatty streaks that are reversible.Citation6 Reports in the medical literature show that the degree of atherosclerosis in children and young adults can be correlated with the same risk factors identified in adults, and minimizing or reducing these known risk factors is prudent.Citation7,Citation8 Therefore, investigating risk factors for that stage of life is fundamentally important, because these risk factors can have profound implications for disease manifestations in adulthood.Citation9–Citation12
Sources
In this systematic review, we analyze the main cardiovascular risk factors present in childhood and their prevalence. Electronic searches were conducted for selected articles from PubMed, SciELO, and Cochrane from 1992 to 2012 using the following terms: physical activity, cardiovascular risk factors, obesity in childhood, children and adolescents, hypertension in childhood, and atherosclerotic disease. Searches for books, dissertations, and theses were performed using the Google Scholar search tool. There was no language restriction. Four researchers independently evaluated the titles that were identified in the initial search. Two authors independently reviewed the articles selected from the initial search for methodological quality, number of subjects studied, and results demonstrated. Studies with dubious methodologies or with very low numbers of assessed individuals and studies that repeated information that was available in other studies were excluded. In the latter case, preference was given to the most recent study and to the study with the greatest number of individuals assessed, respectively. Disagreements were resolved by consensus. The identification of risk factors in children in combination with cooperative action by public agencies and medical professionals, especially pediatricians and cardiologists, can produce positive effects for one of the world’s major public health problems. shows the distribution of the references according to continent and country.
Table 1 Distribution of references according to continent and country
Cardiovascular risk factors
Overview of associated factors
The finding that AD begins at an early stage of life reveals childhood and adolescence as critical periods for the detection of risk factors for cardiovascular disease and the prevention of future complications. Monitoring these factors would help identify early signs that when modified can mitigate or even reverse the progression of those dysfunctions. A range of risk factors, including genetic factors, hypertension, dyslipidemia, obesity, metabolic syndrome (MS), an atherogenic diet, and physical inactivity, is associated with cardiovascular disease, and the prevalence of these factors is increasing among children and adolescents.Citation13–Citation17
Lifestyle and eating habits are fundamentally important for protection against the manifestation and progression of AD risk factors. AD is considered the main causal factor for cardiovascular disease,Citation18,Citation19 and therefore should be a key target of heart disease-prevention programs.Citation20 The emphasis is on hypercholesterolemia, hypertriglyceridemia, overweight, hyperglycemia, hypertension, and physical inactivity.Citation21 Correlations between the plasma levels of cholesterol and a decrease or delay in AD progression by means of diet and lifestyle changes have been documented,Citation22 with the hypothesis that for each 1% reduction in total cholesterol, a decrease of 2% in the occurrence of coronary artery disease was observed. Studies have also reported that the degree of atherosclerosis in children and young adults can be correlated with the same risk factors that have been identified in adults. Therefore, an increase in the incidence of cardiovascular disease is likely to occur when current teens enter adulthood. Thus, as in other age-groups, it is prudent to minimize or reduce risk factors in youth.Citation7
Atherosclerosis
Although AD becomes symptomatic later in life, the early identification and modification of risk factors can reduce its later incidence.Citation1 These diseases are currently the most common causes of death. Studies suggest that the AD process is as old as the human species.Citation3,Citation23 AD begins in childhood; therefore, its prevention should begin early, because at this stage it is considered reversible, with high levels of blood lipoproteins playing a fundamental role in its manifestation.Citation24 In children, fatty streaks in the aorta, although reversible, arise at around 3 years of age and already compromise 15% of this artery by 15 years of age. Several studies cited by Françoso and CoatesCitation23 present evidence of fatty streaks and fibrous plaques in the coronary arteries of adolescents between 10 and 14 years of age and thickening of the inner layer (intima) of the coronary arteries in children less than 5 years of age. Researchers have demonstrated that a fatty diet and other traditional vascular risk factors begin to influence blood lipid levels during the early years of life.Citation6,Citation23
Due to the variety of criteria used to define optimal lipid levels in adolescents, it is difficult to compare results from across the world. However, studies have shown, for example, the presence of atheromatosis in aortic intima with cholesterol levels between 140 and 170 mg/dL. Thus, the epidemiological goals for plasma cholesterol in children would be an average of 150 mg/dL.Citation8
In a review of studies conducted in 26 countries (from 1975 to 1996) involving 60,494 children and adolescents aged 2–19 years, Brotons et alCitation25 found an average of 165 mg/dL for cholesterol, 60 mg/dL for HDL-cholesterol, and 67 mg/dL for triglycerides. demonstrates the lipid levels recommended in adolescents up to 19 years of age.Citation26
Table 2 Recommended lipid levels in adolescents aged up to 19 years
Studies conducted in Brazil revealed higher levels of cholesterol in adolescents attending private schools compared to those attending public school.Citation11,Citation27 This trend was confirmed by other studiesCitation15,Citation28,Citation29 that showed that adolescents with lower family income and those that attend public schools have lower cholesterol levels than adolescents from higher-income families and private schools. These data support Guimarães’s and Guimarães’sCitation29 proposition that families with higher socioeconomic levels do not necessarily have a better and healthier lifestyle. The lower household income in developing countries may prevent these children from consuming high levels of calories in diets heavy in saturated fats and cholesterol. In addition, students of public schools tend to expend more energy in their daily lives because they need to walk to school or use public transportation.
Despite methodological limitations for calculating low-density lipoprotein cholesterol as part of the lipid profile, its measurement is widely regarded as the gold standard for both risk assessment and intervention programs for cardiovascular diseases.Citation8 Because triglycerides are deposited on the vessel wall and initiate the process of low-density lipoprotein accumulation, they are strongly associated with the risk of developing AD.Citation30,Citation31
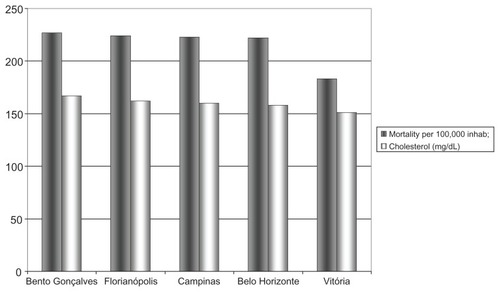
Whether breastfeeding during the first year of life confers protection against future increases in the levels of plasma lipids and mortality by AD is controversial.Citation32 The major health advantage of breastfeeding that has been clearly demonstrated remains in the protection of the infant from certain infections in early life. If there are other long-term health advantages, they have yet to be fully elucidated and confirmed. Dyslipidemia that begins during childhood tends to be maintained through development, and studies describe a direct relationship between total cholesterol levels in children and heart disease in adults.Citation33 Studies conducted in BrazilCitation15,Citation27,Citation34 have shown that cholesterol levels in adolescence correlated with 87% of deaths due to heart disease in adulthood () and showed that high levels of cholesterol are accompanied by a high mortality rate.
Figure 1 Relationship between cholesterol levels in adolescents and mortality from circulatory diseases in Brazil’s cities.
An association between inflammatory processes and the development of atherosclerosis has recently been described, providing important correlations for understanding the mechanisms of atherogenesis and risk factors. Several studies have examined different markers of inflammation in the bloodstream, such as cytokines and adhesion molecules, as potential predictors for the risk of heart disease. Some clinical studies have suggested that serum levels of tumor necrosis factor-α, interleukin-6, and C-reactive protein are elevated in patients with congestive heart failure, regardless of the etiology of the condition. Furthermore, elevated blood levels of these inflammatory markers correlate with worsening functional class, increased hospitalization rates, and poorer survival.Citation35–Citation38 In addition, structural and functional changes have been observed in the arteries of children with a familial predisposition for AD, and these changes are associated with groups of inflammatory factors and oxidation markers. During the development of atheromatous plaques, inflammation plays an essential role in the destabilization of arterial plaques, and in turn is associated with acute thromboembolic diseases. Because lifestyle-modification trials have been successful in decreasing endothelial dysfunction and levels of inflammation markers among children and adolescents, controlling the inflammatory process is suggested in addition to expanding pharmacological therapies, which are considered a secondary means of preventing AD.Citation39
Obesity
Obesity (more specifically, excessive adiposity), which is defined as an excessive accumulation of body fat, is a heterogeneous disorder with a common final pathway in which energy intake chronically exceeds energy expenditure. Obesity features a combination of genetic and environmental factors.Citation40 The energy imbalance often begins in childhood, and when this imbalance occurs the likelihood of obesity in adulthood increases. Among young people, the prevalence of obesity has greatly increased in recent years and represents the most common chronic disorder.Citation41 Excessive adiposity in childhood represents a greater risk to adult health than obesity starting in adulthood. Adults who were overweight as adolescents have an increased risk of diseases compared with adults who were of normal weight as adolescents.Citation42,Citation43 Obesity is the result of a complex interaction of factors, including metabolic, physiological, environmental, genetic, behavioral, and social influences. The Bogalusa Heart Study in Louisiana (USA), which was conducted among children and adolescents, suggested significant correlations between obesity and both lipoprotein levels (low-density lipoprotein in particular) and insulinemia, which were correlated with the risk of cardiovascular diseases.Citation44
Although it is unclear if childhood obesity is an independent risk factor for cardiovascular disease, studies show a clear association between severe obesity and increased mortality. The importance of childhood obesity as a risk factor for cardiovascular disease is increasingly evident.Citation17,Citation45 Obesity deserves particular attention because it is usually accompanied by two notorious and significant risk factors: diabetes and arterial hypertension.Citation46,Citation47 Therefore, controlling obesity during childhood is important because the obesity acquired during this period of life tends to persist into adulthood.Citation11
Studies have reported a substantial increase in the number of overweight children and adolescents in recent decades, and this increase is associated with an increased risk of hypertension, lipid abnormalities, type II diabetes, early atherosclerotic lesions, adult obesity, and mortality in young adulthood.Citation7,Citation48–Citation50 Preventing childhood obesity is the best opportunity to introduce changes in lifestyle and thus reduce cardiovascular morbidity and mortality.Citation51–Citation53 The diagnosis of overweight and obesity still presents difficulties, because the best criteria to determine these categories in this age-group remain unclear. One of the contested methods is the “cutoff point” for their identification. However, the body mass index, based on international standards, is useful, inexpensive, and replicable.Citation54 Recently, the term “obesity” has been used to identify body mass index ≥ P95 in children and adolescents.Citation50
Data on childhood and adolescent obesity around the world are still limited, and the lack of uniformity among definitions and studied age-ranges complicates comparisons of prevalence. Obesity in children and adolescents is increasing significantly, including in developing countries.Citation55 A national study, Nutre Brasil Infância (Nourish Brazil Childhood), indicated that 23% of Brazilian children up to 5 years of age exhibit excess weight,Citation56 while in developed countries, obesity mainly affects the lower-income social classes; in Brazil, for example, the most favored social classes are still the most affected, although there is a tendency toward change. The most recent studies conducted in Brazil reveal that the prevalence of overweight in children and adolescents ranges from 8.4% to 19%, while that of obesity ranges from 3.1% to 18%;Citation54,Citation57 furthermore, the prevalence of overweight and obesity is greater in higher-income households.Citation58,Citation59 The National Health and Nutrition Examination Survey estimated a prevalence of 30% for overweight and obesity ≥ P85 and a prevalence of 15% for obesity ≥ P95 for the age-group between 6 and 19 years of age.Citation60 In Brazil, studies stress the physical inactivity of children as one of the most important factors associated with obesity.Citation49–Citation54
Metabolic syndrome
MS is currently characterized as the combination of a number of risk factors for cardiovascular disease, including dyslipidemia, hypertension, carbohydrate-metabolism disorders, and obesity, especially abdominal obesity.Citation61 In children, the global consensus regarding MS is still a matter of discussion.Citation26 A direct association between obesity and insulin-resistance syndrome has been demonstrated in children, and was recently recognized as a major precursor of atherosclerotic cardiovascular disease and type II diabetes.Citation7,Citation62
Although we do not have a global consensus to define and diagnose MS in adults and children, MS is associated with a 1.5-fold increase in overall mortality and a 2.5-fold increase in cardiovascular mortality.Citation63 Given its importance, various organizations, including the World Health Organization,Citation64 the National Cholesterol Education Program Adult Treatment Panel III,Citation65 the European Group for the Study of Insulin Resistance,Citation66 and the International Diabetes Federation, have proposed criteria to define and treat MS.
To determine the prevalence of MS in children and adolescents, either the adult criteria are modified for pediatric reference values,Citation67 or specific cutoff points are used.Citation68,Citation69 Some studies suggest cutoff points corresponding to the 95th percentiles of each variable by sex and age and the height percentile when including blood pressure (BP).Citation70,Citation71 However, the lack of consensus means that the prevalence of this syndrome is markedly different in different studies.Citation72 demonstrates the definition considered most suitable for MS, according to the Department of Metabolic Syndrome of the Brazilian Society of Diabetes.Citation26
Table 3 Classification of metabolic syndrome in children and adolescents
Prospective studies have shown that obesity looms as the most important risk factor for MS and precedes the onset of insulin resistance by several years;Citation62,Citation73 insulin resistance is the leading cause of the hemodynamic and metabolic disorders of MS.Citation74 MS is caused by a combination of genetic and environmental factors in which obesity plays a primary role and leads to excessive production of insulin, which is associated with an increase in BP and dyslipidemia.Citation50 An estimated 1 million US adolescents already meet the criteria for MS,Citation50 with a prevalence of 4% between 12 and 19 years of age. In addition, MS is present in 30%–50% of overweight children.Citation67,Citation75
Hypertension
Identified as one of the most common precursors of coronary artery disease, hypertension is usually asymptomatic, and prevention is the most efficient way to fight it and avoid the high social cost of its treatment and complications. Therefore, the need to measure hypertension levels and identify those individuals with high BP is mandatory. The worldwide prevalence of hypertension in children is highly variable (2%–13%), depending on the methodology employed. In Brazil, for example, it is estimated that the prevalence of hypertension in children and adolescents is 4%,Citation76 and the need for BP measurement is considered imperative from 3 years of age. Arterial BP commonly rises with age, and its elevation in children is a prediction of hypertension in adulthood that may have started in childhood or adolescence.Citation7,Citation77–Citation80
BP should be interpreted as a result of the impact of environmental influences on the expression of several genes that in turn regulate other genes. It is influenced by angiotensin-converting enzyme gene expression and for endothelial NO synthase gene expression.Citation81,Citation82 Several known factors related to hypertension in adults, such as sex, age, family history, and the presence of increased body weight or obesity, are also observed in children and adolescents.Citation83 High BP contributes to the development of cardiovascular complications. Its association with multiple risk factors has a multiplier effect on the risk of cardiovascular events.Citation84–Citation86
Hypertension is diagnosed when the values of systolic BP and/or diastolic BP are greater than or equal to the 95th percentile for sex, age, and height, plus 5 mmHg, on three separate occasions. A prehypertensive group should also be defined and identified with the purpose of adopting stringent preventive measures. BP values ≥ 90th percentile and <95th percentile characterize prehypertension; values that are included in this range and exceed the limits of 120/80 mmHg should also be considered as prehypertensive and follow the same recommendations proposed by the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7)Citation85 for adults. summarizes the classification of BP for children and adolescents.Citation87
Table 4 Classification of blood pressure for children and adolescents (modified from the fourth report on the diagnosis, evaluation and treatment of high blood pressure in children and adolescents)Citation87
It is estimated that 30% of children and adolescents with overweight/obesity have hypertension.Citation88 Thus, the presence of overweight/obesity appears to be one of the most important factors related to hypertension in children and adolescents worldwide.Citation85,Citation89,Citation90 Several studies have shown that the presence of overweight/obesity is positively correlated with the occurrence of prehypertension in children and adolescents, and this combination increases the risk of developing adult hypertension.Citation91–Citation94 Certain conditions are strongly associated with hypertension in teens, including smoking and the use of contraceptives, alcohol, cocaine, amphetamines, anabolic steroids, phenylpropanolamine, and pseudoephedrine (nasal decongestants).
Therefore, changes in lifestyle, such as weight control, reduction in sodium intake, and exercise, are fundamental for the prevention of hypertension. Although threshold pressure levels are not yet well defined, BP most likely affects target organs in children, as in adults. Dietary intervention, maintaining an ideal weight, and engaging in regular physical activity could be encouraged at this stage as a method of primary prevention.Citation24 In a study on the stiffness of large arterial vessels, which is attributed to aging, the only studied factor that could explain the group with vessels that did not show signs of age was the lowest BP level presented.Citation95
Sedentary behavior
The death rate from cardiovascular disease is lower in individuals who exercise regularly, and there are no doubts about the improvement in quality of life that is achieved through a physical conditioning program. However, this improvement depends on a proper prescription, and intensity, duration, and modality have an important role for a satisfactory result. In adults, the recommended physical conditioning activities lie between the ventilatory threshold and the respiratory compensation point; that range is most recommended for its beneficial effects on cardiopulmonary capacity.Citation96 In children, the beneficial effects associated with physical activity include weight control, effects on cholesterol levels and insulin resistance, low BP, psychological well-being, and an increased predisposition for physical activity in young adulthood.Citation7,Citation97 Adolescents should engage in physical activities of moderate to vigorous intensity for at least 60 minutes a day, 5 days a week; this activity can be in or outside school and can be structured.Citation97
A major challenge for public health authorities has been to increase the cardiorespiratory fitness of the population. Childhood and adolescence appear to be periods for promoting good physical activity habits and preventing sedentary behavior in adulthood. Therefore, the prevention of cardiovascular disease is also a pediatric problem.Citation5 In recent decades, children have become less physically active, with energy expenditure approximately 600 kcal/day lower than their contemporaries 50 years ago.Citation98 Physical inactivity is recognized as an important determinant of chronic diseases, and an increase in the prevalence of these diseases during childhood has been documented.Citation99
Attention has been drawn to the need for physical education programs in schools and for community recreation facilities. However, few empirical studies have been conducted to determine the impact of such facilities and programs on physical activity and the level of inactivity in adolescents.Citation100 Among adolescents, there is a trend to engage less in school physical education activities and vigorous activities and to spend more time watching television.Citation101,Citation102 These behaviors can affect future health problems, whereas greater physical fitness has been linked to a lower cardiovascular risk profile in children and adolescents.Citation103
Identifying population values of maximal oxygen consumption (VO2max) is important in studies that attempt to relate physical fitness to cardiovascular risk. VO2max is a measurement that is used to guide the prescription of exercise and analyze the effect of training programs.Citation104,Citation105 Aerobic capacity measured through VO2max depends on cardiovascular, respiratory, and hematological components, and the oxidative mechanisms of muscle in exercise. This value is determined by means of cardiopulmonary exercise testing, which allows the simultaneous assessment of the cardiovascular and respiratory systems’ ability to perform their main functions, such as gas exchange.Citation104 Measurements of gas exchange are fundamental to understand the limitations of exercise. However, multiple paths (direct or indirect) have been used to determine cardiorespiratory fitness. The differences in the methods used may be responsible for the differences found in the predictive power of this important physiological variable and whether cardiorespiratory fitness can serve as a predictor of blood lipids in children.Citation106 However, the expected increase in BP with age is lower in children with better physical fitness.Citation107
Adolescence is the period of transition to adulthood, during which many structural, hormonal, and biochemical changes occur in physiological systems that affect VO2max.Citation108 Thus, it is necessary to establish specific VO2max values for this population. The international literature offers benchmarks for healthy children and adolescents.Citation15,Citation104,Citation109
Described as a behavior, physical activity includes many types of muscular activity that significantly increase energy expenditure. Physical fitness is described as an attribute, and generally refers to the ability to perform physical work; in addition, physical fitness is considered an adaptive state and is partly genetically determined.Citation110 Physical fitness measurements are preferred over physical activity measurements because they are more objective and less error-prone. In addition, aerobic fitness and physical activity correlate better with cardiovascular diseases. Thus, efforts should be intensified to identify the starting point for daily physical activity to increase physical fitness in youth.Citation110–Citation112 However, determining this variable is not yet a global reality, and empirical evaluations have been performed. The use of cardiopulmonary exercise testing makes it possible to assess metabolic and cardiopulmonary capacity accurately through direct measurements of VO2 max. This value is the most important physiological measurement for determining aerobic capacity, the accurate level of physical fitness, and therefore the correct intensity of exercise to obtain the health benefits of a fitness program.Citation96
Conclusion
Although the manifestation of coronary heart disease occurs in adulthood, detecting risk factors during childhood is crucial for establishing a prognosis and preventing damage to target organs in adults. Thus, detection and prevention should begin during childhood, when changes in lifestyle can reduce the incidence and severity of heart disease. School seems to be the key to achieving this goal.
Studies of cardiovascular risk factors in a region, city, or country should always report the prevalence and its correlations in childhood as a fundamental step in identifying a population at risk.
The studies reviewed here note the gravity of the public health problem represented by coronary heart disease. It is imperative to discuss the issues of health promotion and the prevention of future diseases that arise from the risk factors mentioned in this review.
Autopsy studies clearly indicate that atherosclerotic lesions appear during childhood. Therefore, if the risk factors for cardiovascular diseases begin in childhood, they should be addressed at this stage. This timing reinforces the need for rigorous pediatric care in this age-group for an early diagnosis, particularly counseling regarding preventive measures. For example, dyslipidemia, which is the major known risk factor, can be modified by a moderate fat restriction without impairing the growth and development of children older than 2 years of age. Thus, it is possible to achieve a great impact on cardiovascular disease through research on evaluation of risk factors in asymptomatic children.
Therefore, it would be beneficial to identify those children and adolescents with the highest risk as early in life as possible, so that interventions to reduce cardiovascular risk could be targeted. Indeed, there are existing guidelines on screening of dyslipidemia, elevated BP, and obesity in childhood; however, there is a shortage of data on the optimal age for screening of cardiovascular disease risk factors in childhood.
It is necessary to raise social awareness at all levels and develop studies to plan programs and actions to control dyslipidemia, obesity, high BP, and a sedentary lifestyle at an early age so that they do not become the epidemics of this new century.
Acknowledgment
The authors thank Geraldo Magela Freitas dos Santos for editing, formatting, and proofreading this study.
Disclosure
The authors have nothing to declare.
References
- KelishadiRZadeganNSNaderiGAAsgarySBashardoustNAtherosclerosis risk factors in children and adolescents with or without family history of premature coronary artery diseaseMed Sci Monit20028425429
- StrongWBKelderSHPediatric preventive cardiologyMansonJERidkerPMGazianoDMHennekensCHPrevention of Myocardial InfarctionOxfordOxford University Press1996433459
- LotufoPANovos conceitos sobre uma Velha RealidadeMionDJrNobreFRisco Cardiovascular GlobalSão PauloLemos Editoria19993143
- PellandaLCEcheniqueLBarcellosLMAMaccarIJBorgesFKZenBLDoença cardíaca isquêmica: a prevenção inicia durante a infânciaJ Pediatr2002789196
- MassinMVandoorneCCoremansCLepagePScheenAPreventive cardiology: strategies in childrenRev Med Liege20025720721212073792
- MichaelsenKFDyerbergJFalkEChildren, fat and cardiovascular diseasesUgeskr Laeger200216413341338 Danish11894424
- WilliamsCLHaymanLLDanielsSRCardiovascular health in childhood: a statement for health professionals from the Committee on Atherosclerosis, Hypertension, and Obesity in the Young (AHOY) of the Council on Cardiovascular Disease in the Young, American Heart AssociationCirculation200210614316012093785
- SrinivasanSRMyersLBerensonGSDistribution and correlates of non-high-density lipoprotein cholesterol in children: the Bogalusa Heart StudyPediatrics20021102932
- LenfantCSavagePJThe early natural history of atherosclerosis and hypertension in the young: National Institutes of Health perspectivesAm J Med Sci1995310Suppl 1S3S77503121
- PurathJLansingerTRaghebCCardiac risk evaluation for elementary school childrenPublic Health Nurs1995121891957596968
- GerberZRSZielinskyPFatores de Risco de Aterosclerose na infância. Um Estudo EpidemiológicoArq Bras Cardiol1997692312369595714
- AkerblomHKViikariJRaitakariOTUhariMCardiovascular risk in Young Finns Study: general outline and recent developmentsAnn Med199931455410342500
- HedleyAAOgdenCLJohnsonCLCarrollMDCurtinLRFlegalKMPrevalence of overweight and obesity among US children, adolescents, and adults, 1999–2002JAMA20042912847285015199035
- EckelRHYorkDARössnerSPrevention Conference VII: Obesity, a worldwide epidemic related to heart disease and stroke: executive summaryCirculation20041102968297515520336
- RodriguesANMoysesMRBissoliNSPiresJGPAbreuGRCardiovascular risk factor in a population of Brazilian schoolchildrenBraz J Med Biol Res2006391637164217160273
- RodriguesANPerezAJPiresJGCardiovascular risk factors, their associations and presence of metabolic syndrome in adolescentsJ Pediatr (Rio J)200985556019198738
- SantosMGPegoraroMSandriniFMacucoECFatores de risco no desenvolvimento da aterosclerose na infância e adolescênciaArq Brás Cardiol200890301308
- BerlinJAColditzGAA meta-analysis of physical activity in the prevention of coronary heart diseaseAm J Epidemiol19961326126282144946
- EsreyKLJosephLGroverSARelationship between dietary intake and coronary heart disease mortality: lipid research clinics prevalence follow-up studyJ Clin Epidemiol1996492112168606322
- GuedesDPGuedesJERPAtividade física, aptidão cardiorrespiratória, composição da dieta e fatores de risco predisponentes às doenças cardiovascularesArq Bras Cardiol20017724325011562687
- AustinMAEpidemiology of hypertriglyceridemia and cardiovascular diseaseAm J Cardiol19998313F16F
- CoelhoORUetiOMAlmeidaALípides como fator de riscoMionDJrNobreFRisco Cardiovascular GlobalSão PauloLemos Editorial19994564
- FrançosoLACoatesVEvidências anatomopatológicas do início da aterosclerose na infância e adolescênciaArq Bras Cardiol20027813113611826356
- MassinMCoremansCPalumboLLepagePPreventive cardiology: the role of the pediatricianItal J Pediatr20022898104
- BrotonsCRiberaAPerichRMWorldwide distribution of blood lipids and lipoproteins in childhood and adolescence: a review studyAtherosclerosis1998139199699886
- HalpernAManciniMCMagalhãesMECMetabolic syndrome, dyslipidemia, hypertension and type 2 diabetes in youth: from diagnosis to treatmentDiabetol Metab Syndr201025520718958
- GiulianoICBCaramelliBDislipidemias em crianças e adolescentesRev Soc Cardiol Estado São Paulo20056535543
- GuimarãesACLimaAMotaEThe cholesterol level of a selected Brazilian salaried population: biological and socioeconomic influencesCVD Prev19981306317
- GuimarãesICBGuimarãesACPrevalence of cardiovascular risk factors in selected samples of schoolchildren – socioeconomic influencePrev Cardiol20058232815722691
- HokansonJEAustinMAPlasma triglyceride level is a risk factor for cardiovascular disease independent of high-density lipoprotein cholesterol level: a meta-analysis of population-based prospective studiesJ Cardiovasc Risk199632132198836866
- GazianoDMHennekensCHPrevention of Myocardial InfarctionOxfordOxford University Press1996433459
- GoldingJEmmetPMRogersISDoes breast feeding have any impact on non-infectious, non-allergic disorders?Early Hum Dev199749SupplS131S1429363422
- FortiNGianniniSDDiamentJFatores de risco para aterosclerose em filhos de pacientes com doença coronariana precoceArq Bras Cardiol1996661191238762687
- RodriguesANAbreuGRGouvêaSACardiovascular risk investigation: when should it start?GasparyanAYCardiovascular Risk FactorsRijeka CroatiaInTech2012
- Alonso-MartinezJLLlorente-DiezBEchegaray-AgaraMOlaz-PreciadoFUrbieta-EchezarretaMGonzález-ArencibiaCC-reactive protein as a predictor of improvement and readmission in heart failureEur J Heart Fail2002433133612034159
- MaedaKTsutamotoTWadaAHigh levels of plasma brain natriuretic peptide and interleukin-6 after optimized treatment for heart failure are independent risk factors for morbidity and mortality in patients with congestive heart failureJ Am Coll Cardiol2000361587159311079662
- VasanRSSullivanLMRoubenoffRInflammatory markers and risk of heart failure in elderly subjects without prior myocardial infarction: the Framingham Heart StudyCirculation2003107111486149112654604
- ToprakAKandavarRToprakDC-reactive protein is an independent predictor for carotid artery intima-media thickness progression in asymptomatic younger adults (from the Bogalusa Heart Study)BMC Cardiovasc Disord2011117822208681
- KelishadiRInflammation-induced atherosclerosis as a target 1 for prevention of cardiovascular diseases from early lifeOpen Cardiovasc Med J20104242921804638
- SorensenTIAThe genetics of obesityMetabolism199544Suppl 3467674914
- TroianoRPFlegalKMOverweight children and adolescents: description, epidemiology and demographicsPediatrics1998101Suppl 349750412224656
- GunnellDJFrankelSJNanchahalKPetersTJSmithGDChildhood obesity and adult cardiovascular mortality: a 57-y follow-up study based on the Boyd Orr cohortAm J Clin Nutr199867111111189625081
- VanHornLGreenlandPPrevention of coronary artery disease is a pediatric problemJAMA1997278177917809388158
- KikuchiDASrinivasanSRHarshaDWWebberLSSellersTABerensonGSRelation of serum lipoprotein lipids and apolipoproteins to obesity in children: the Bogalusa Heart StudyPrev Med1992211771901579553
- ZanellaMTObesidadeMionDJrNobreFRisco Cardiovascular GlobalSão PauloLemos Editorial1999103114
- CaliAMCaprioSObesity in children and adolescentsClin Endocrinol Metab200893S31S36
- LloydLJLangley-EvansSCMcMullenSChildhood obesity and adult cardiovascular disease: a systematic reviewInt J Obes (Lond)201034182819434067
- CoronelliCLSMouraECHipercolesterolemia em escolares e seus fatores de riscoRev Saude Publica200337243112488917
- AlvesJGBSiqueiraPPFigueiroaJNOverweight and physical inactivity in children living in favelas in the metropolitan region of Recife, BrazilJ Pediatr (Rio J)200985677119198735
- DanielsSRArnettDKEckelRHOverweight in children and adolescents: pathophysiology, consequences, prevention, and treatmentCirculation20051111999201215837955
- BuitenCMetzgerBChildhood obesity and risk of cardiovascular disease: a review of the sciencePediatr Nurs200026131812026312
- WatersEde Silva-SanigorskiAHallBJInterventions for preventing obesity in childrenCochrane Database Syst Rev201112CD00187122161367
- SummerballCDMooreHJVogeleCEvidence-based recommendations for the development of obesity prevention programs targeted at preschool childrenObes Rev201213Suppl 112913222309071
- GiuglianoRMeloALPDiagnóstico de sobrepeso e obesidade em escolares: utilização do índice de massa corporal segundo padrão internacionalJ Pediatr200480129134
- MelloEDLuftVCMeyerFObesidade infantil: como podemos ser eficazes?J Pediatr200480173182
- BuenoMBMarchioniDMFisbergRMChanges in the nutritional status of children in public day care facilities in the municipality of São Paulo, BrazilRev Panam Salud Publica20031416517014653903
- SilvaDASPelegriniAPetroskiELGayaACAComparison between the growth of Brazilian children and adolescents and the reference growth charts: data from a Brazilian projectJ Pediatr (Rio J)20108611512020143011
- AbrantesMMLamounierJAColosimoEAPrevalência de sobrepeso e obesidade em crianças e adolescentes das regiões Sudeste e NordesteJ Pediatr200278335340
- MouraAASilvaMAMFerrazMRMTRiveraIRPrevalência de pressão arterial elevada em escolares e adolescentes de MaceióJ Pediatr2004803540
- O’BrienSHHolubkoyRReisECIdentification, evaluation, and management of obesity in an academic primary care centerPediatrics2004114154159
- ReavensGMLithellHLandsbergLHypertension and associated abnormalities – the role of insulin resistance and the sympathoadrenal systemN Engl J Med19963347481
- BrandãoAPBrandãoAABerensonGSFusterVMetabolic syndrome in children and adolescentsArq Bras Cardiol200585798116113843
- LakkaHMLaaksonenDELakkaTAThe metabolic syndrome and total cardiovascular disease mortality in middle-aged menJAMA20022882709271612460094
- AlbertiKGZimmetPZDefinition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultationDiabet Med1998155395539686693
- National Cholesterol Education ProgramDetection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III)Bethesda (MD)National Institutes of Health2002
- BalkauBCharlesMAComment on the provisional report from the WHO consultation. European Group for the Study of Insulin Resistence (EGIR)Diabet Med19991644244310342346
- CookSWeitzmanMAuingerPNguyenMDietzWHPrevalence of a metabolic syndrome phenotype in adolescents: findings from the third National Health and Nutrition Examination Survey, 1988–1994Arch Pediatr Adolesc Med200315782182712912790
- CsábiGTörökKJegesSMolnárDPresence of metabolic cardiovascular syndrome in obese childrenEur J Pediatr2000159919410653338
- SrinivasanSRMyersLBerensonGSPredictability of childhood adiposity and insulin for developing insulin resistance syndrome (syndrome X) in young adulthood: the Bogalusa Heart StudyDiabetes20025120420911756342
- National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and AdolescentsThe fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescentsPediatrics200411455557615286277
- The Expert Committee on the Diagnosis and Classification of Diabetes MellitusReport of the expert committee on the diagnosis and classification of diabetes mellitusDiabetes Care199922Suppl 1S5S19
- IsomaaBAlmgrenPTuomiTCardiovascular morbidity and mortality associated with the metabolic syndromeDiabetes Care20012468368911315831
- TaskinenMRDiabetic dyslipidemia: from basic research to clinical practiceDiabetologia20034673374912774165
- MortonNMHolmesMCFievetCImproved lipid and lipoprotein profile, hepatic insulin sensitivity and glucose tolerance in 11 beta hydroxyesteroid dehydrogenase type 1 null miceJ Biol Chem2001276412934130011546766
- WeissRDziuraJBurgertTSObesity and the metabolic syndrome in children and adolescentsN Engl J Med20043502362237415175438
- Cadernos de Atenção BásicaHipertensão Arterial SistêmicaBrasiliaMinistério da Saúde;2006
- FalknerBGiddingSSPortmanRRosnerBBlood pressure variability and classification of prehypertension and hypertension in adolescencePediatrics200812223824218676538
- RajMEssential hypertension in adolescents and children: recent advances in causative mechanismsIndian J Endocrinol Metab201115Suppl 4S367S37322145141
- OliveiraRGLamounierJAOliveiraADBCastroMDROliveiraJSBlood pressure in school children and adolescents – the Belo Horizonte studyJ Pediatr (Rio J)199975256266 Portuguese14685527
- SalgadoCMCarvalhaesJTAArterial hypertension in childhoodJ Pediatr (Rio J)200379Suppl 1S115S12414506524
- McmillenCRobinsonJSDevelopmental origins of the metabolic syndrome: prediction, plasticity, and programmingPhysiol Rev20058557163315788706
- CarlsonSHOparilSChenYFWyssJMBlood pressure and NaCl-sensitive hypertension are influenced by angiotensin-converting enzyme gene expression in transgenic miceHypertension20023921421811847186
- RosaAARibeiroJPHigh blood pressure in children and adolescents: determinant factorsJ Pediatr (Rio J)199975758214685545
- KaveyREWDanielsSRLauerRMAtkinsDLHaymanLLTaubertKAmerican Heart Association guidelines for primary prevention of atherosclerotic cardiovascular disease beginning in childhoodCirculation20031071562156612654618
- ChobanianAVBakrisGLBlackHRThe Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 reportJAMA20032892560257212748199
- LiebermanEHypertension in childhood and adolescenceKaplanNMClinical Hypertension8th edBaltimoreWilliams & Wilkins2002512526
- Sociedade Brasileira de Cardiologia/Sociedade Brasileira de Hipertensão/Sociedade Brasileira de NefrologiaVI Diretrizes Brasileiras de HipertensãoArq Bras Cardiol201095151
- SorofJDanielsSObesity hypertension in children: a problem of epidemic proportionsHypertension20024044144712364344
- CampanaANNBTavaresMCGCFAvaliação da Imagem Corporal: Instrumentos e Diretrizes para a PesquisaSão PauloPhorte2009
- European Society of HypertensionGuidelines for the management of arterial hypertensionJ Hypertens2003211011105312777938
- [No authors listed]The effects of nonpharmacologic interventions on blood pressure of persons with high normal levels. Results of the Trials of Hypertension Prevention, phase IJAMA1992267121312201586398
- MonteiroCACondeWLCastroIRThe changing relationship between education and risk of obesity in Brazil (1975–1997)Cad Saude Publica200319Suppl 1S67S75 Portuguese12886437
- RosaMLFonsecaVMOigmanGMesquitaETArterial prehypertension and elevated pulse pressure in adolescents: prevalence and associated factorsArq Bras Cardiol2006874653 Portuguese16906269
- SrinivasanSRMyersLBerensonGSChanges in metabolic syndrome variables since childhood in prehypertensive and hypertensive subjects: the Bogalusa Heart StudyHypertension200648333916769996
- RodriguesANCoelhoLCGoncalvesWLStiffness of the large arteries in individuals with and without Down syndromeVasc Health Risk Manag2011737538121731889
- RondonMUPBForjazCLMNunesNAmaralSLBarrettoACPBNegrãoCEComparação entre a prescrição de intensidade de treinamento físico baseada na avaliação ergométrica convencional e na ergoespirometriaArq Bras Cardiol1998701591669674176
- StrongWBMalinaRMBlimkieCJEvidence based physical activity for school-age youthJ Pediatr200514673273715973308
- BorehamCRiddochCThe physical activity, fitness and health of childrenJ Sports Sci20011991592911820686
- TwiskJWPhysical activity guidelines for children and adolescents: a critical reviewSports Med20013161762711475323
- Gordon-LarsenPMcMurrayRGPopkinBMDeterminants of adolescent physical activity and inactivity patternsPediatrics2000105E8310835096
- FreedmanDSSrinivasanSRValdezRAWilliamsonDFBerensonGSSecular increases in relative weight and adiposity among children over two decades: the Bogalusa Heart StudyPediatrics1997994204269041299
- LippoBRSSilvaIMAcaCRPLiraPICSilvaGAPMottaMEFADeterminants of physical inactivity among urban adolescentsJ Pediatr (Rio J)20108652052421140040
- Al-HazaaHMPhysical activity, fitness and fatness among Saudi children and adolescents: implications for cardiovascular healthSaudi Med J20022314415011938387
- ArmstrongNWelsmanJRAssessment and interpretation of aerobic fitness in children and adolescentsExerc Sport Sci Rev1994224354767925551
- ObertPMandigoutSNottinSVinetAN’GuyenDLecoqACardiovascular responses to endurance training in children: effect of genderEur J Clin Invest20033319920812641537
- TolfreyKCampbellIGJoneAMSelected predictor variables and the lipid-lipoprotein profile of prepubertal girls and boysMed Sci Sports Exerc1999311550155710589856
- SheaSBaschCEGutinBThe rate of increase in blood pressure in children 5 years of age is related to changes in aerobic fitness and body mass indexPediatrics1994944654707936854
- Tourinho FilhoHTourinhoLSPRCrianças, adolescentes e atividade física: aspectos maturacionais e funcionaisRev Paul Educ Fis1998127184
- TurleyKRWilmoreJHCardiovascular responses to treadmill and cycle ergometer exercise in children and adultsJ Appl Physiol1997839489579292484
- ThomasNEBakerJSDaviesBEstablished and recently identified coronary heart disease risk factors in young people: the influence of physical activity and physical fitnessSports Med20033363365012846588
- BouchardCDionneFTSimoneauJABoulayMRGenetics of aerobic and anaerobic performancesExerc Sport Sci Rev19922027581623888
- McMurrayRGAinsworthBEHarrellJSGriggsTRWilliamsODIs physical activity or aerobic power more influential at reducing cardiovascular disease risk factors?Med Sci Sports Exerc199830152115299789853