
Abstract
Background
The hydration state of the body is getting more and more attention from researchers. The purpose of this study is to investigate the relationship between impaired hydration status and postoperative hospitalization death in patients with A AAD.
Methods
From January 2019 to October 2021, the clinical data of 299 patients undergoing A AAD surgery were retrospectively analyzed. Patients were divided into normal hydration group, imminent dehydration group and current dehydration group according to the dehydration standard at admission. Univariate and multivariate logistic regression analysis were used to determine the independent risk factors for in-hospital death of patients with A AAD.
Results
Postoperative in-hospital death in A AAD patients was significantly more common in the imminent and current dehydration groups (>295mmol/L) (26.7% vs 11.9%; P=0.001). The length of ICU stay was significantly longer in the impending and current dehydration groups (P<0.05). After controlling for other factors by multivariate logistic regression analysis, the results showed that the group of impending and current dehydration (>295) (OR=3.61, 95% confidence interval [CI]: 1.61–8.06; P=0.002), CRRT (OR=10.55, 95%[CI]: 3.59–31.01; P<0.001), lactic acid (OR=1.25, 95%[CI]: 1.13–1.38; P<0.001), CAD (OR=5.27, 95%[CI]: 1.12–24.80; P=0.035) was an independent risk factor for in-hospital death in A AAD patients. Albumin (OR=0.92, 95%[CI]: 0.85–0.99; P=0.040) is a protective factor.
Conclusion
The presence of high serum osmotic pressure on admission of A AAD patients can independently predict postoperative death, and the impaired body hydration status should be paid attention to.
Introduction
Acute type A aortic dissection (A AAD) is A life-threatening vascular emergency requiring urgent diagnosis and treatment. Although treatments continue to improve, especially successful surgical treatment in time, but still in hospital mortality of 18 ~ 22%.Citation1–4 Studies have found that clinical outcomes in A AAD patients with difference is very big,Citation5 even after treatment in acute index event still in high-risk state, worthy of attention. A AAD patients, once identified, are generally transported by the emergency department for emergency surgery. Buaprasert et al according to a study in patients with emergency admission 1/5 of the existence of high permeability dehydration.Citation6 Previous experiments have shown that in the state of hypertonic dehydration, the blood volume is relatively reduced, the blood is concentrated, and the blood viscosity is increased, which can not meet the blood supply of the corresponding organs. This is one of the important reasons leading to preoperative hypoperfusion of blood volume in patients with A AAD. As is known to all, poor perfusion is an evidence-based risk factor for increased mortality.Citation7,Citation8 Girdauskas et al found that the presence of preoperative hypoperfusion in patients with A AAD was associated with an increased risk of postoperative death, and hypoperfusion was the most decisive preoperative factor.Citation9 However, it is not known whether impaired hydration, such as hypertonic dehydration, is present in patients with A AAD before surgery.
In recent years, many scholars begin to pay close attention to the body gradually the change of the state of hydration, and dehydration is a manifestation of impaired hydration status. Hypertonic dehydration occurs when the kidneys lose too much water due to inadequate fluid intake, resulting in elevated serum osmolarity.Citation10 Studies have shown that dehydration may lead to an increased risk of death from cardiovascular disease.Citation11 The predictive value of serum osmolality for mortality has been reported in some specific patients, such as those with intracranial hemorrhage and acute coronary syndromes.Citation12,Citation13 In an intensive care unit (ICU) in the study, in the heart, brain, blood vessels, and gastrointestinal tract disease in critically ill patients in the hospital, high serum osmotic pressure is associated with increased mortality.Citation14 However, the association between serum osmolality imbalance and mortality has not been studied. Effective identification of high-risk groups and implementation of interventions to reverse dehydration and reduce the current risk of dehydrationCitation15 will help improve the clinical prognosis of patients with A AAD.
Clinically, effective assessment of hydration status is hampered by the complexity of patient signs and the low accuracy of instrumental techniques used for assessment.Citation16 The bioelectrical impedance analyzer (BIA) currently used in clinical practice is susceptible to external factors, such as sweat, skin temperature, and electrode position, which can significantly affect the measurement results.Citation15 Studies have shown that the difference between directly measured and calculated osmolality is negligibleCitation15,Citation17 and that serum osmolality may be a better feature of actual dehydration even in young adults.Citation18 Therefore, this research by calculating A AAD patients serum osmotic pressure on admission to hospital to evaluate hydration damaged condition.
Based on the above analysis, this study retrospectively analyzed 299 eligible patients with A AAD, in order to explore the relationship between serum osmolality on admission and postoperative in-hospital death in patients with A AAD, so as to provide a better theoretical basis for clinical practice.
Method
Patient Collection
A total of 400 patients diagnosed with A AAD by CT angiography and magnetic resonance imaging (MRI) were admitted to the Department of Cardiac Surgery of the Union Hospital Affiliated to Fujian Medical University from January 2019 to October 2021. All patients with A AAD were screened postoperatively in the intensive care unit (ICU) and received standard care. Qualified participants will be included in the final analysis if they meet the following criteria. The inclusion criteria are: (1) onset time<14 days; (2) aged 18 or above. Patients with the following conditions were excluded: (1) preoperative hypernatremia; (2) severe infection, autoimmune disease, multiple organ failure (MODS), sepsis or cancer at admission; (3) patients with incomplete clinical data. This study was approved by the Ethics Committee of the hospital, and the Ethics Committee approval number was 2021KJT055. This study is a retrospective observational study of informed consent, and conform to the declaration of Helsinki. We ensured that all patient data were confidential and anonymized and were used only for data analysis.
Data Collection
The clinical data of patients were collected retrospectively by searching clinical electronic databases. The patients’ socio-demographic characteristics, including age, sex, BMI, and past history, were collected. Collect diagnosis and treatment records and laboratory test results, such as temperature, heart rate, blood pressure, intraoperative clinical data, blood tests and biochemical tests on admission.
Variable Definition
Preoperative hydration state (normal hydration or dehydration) results were grouped according to the calculation formula of serum osmotic pressure: 1.86×(Na++K+) +1.15×glucose + urea +14 (mmol/L).Citation19 In-hospital death was the primary end point, and secondary end points were other postoperative complications during hospitalization, including liver insufficiency, renal insufficiency, gastrointestinal bleeding, MODS, cerebral infarction, and neurological complications. MODS was defined as sequential organ failure score > 6 at least 48 hours after admission (2 consecutive days or more).Citation20
Data Analysis
Statistical analysis was performed by IBM SPSS® 26.0, and GraphPad Prism 9.0 for Windows (GraphPad software, La Jolla, CA, USA) was used for plotting. The hydration status (serum osmotic pressure) of all patients at admission was divided into normal hydration group (275–295) and imminent and current dehydration group (>295). The characteristics of patients between the two groups were analyzed and compared. The measurement data were expressed by Mean and SD. When it satisfies the normal distribution, it’s described by means and standard deviations; When normal distribution is not satisfied, median and interquartile spacing are used. For the comparison of non-normal distribution data, the Mann–Whitney rank sum (U) test was used. Counting data were represented by numbers and percentage values (%), and Chi-square test was used to compare differences of categorical variables. When the conditions of Chi-square test were not met, Fisher’s exact test was used, and the value P<0.05 (bilateral) was considered significant. First, single logistic regression analysis was used to preliminarily determine the potential risk factors of in-hospital death (P<0.1), and then multiple logistic regression analysis was used to confirm the risk factors (P<0.05).
Results
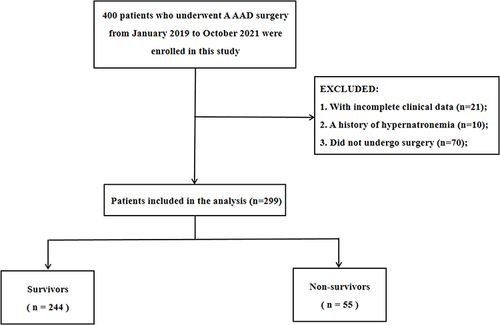
A total of 400 patients with A AAD were enrolled between January 2019 and October 2021. Excluding 21 patients with incomplete medical records, 10 patients with hypernatremia on admission and 70 patients without surgery, 299 patients were included in the study. Of these, 55 died and 244 survived (). As shown in , there were 221 males (73.9%) and 78 females (26.1%). The median age of patients was 54.0. There were 198 patients (66.2%) with hypertension, 136 patients (45.5%) with smoking, and 93 patients (31.1%) with drinking alcohol. In this study, the mortality rate of patients with A AAD was 18.4%.
Table 1 Baseline Clinical Data of Patients with A AAD at Admission
Figure 1 Patient flow chart of the cohort.
Preoperative Clinical Data Characteristics of the Two Groups
According to the groups of water loss/dehydration, they were divided into euhydration group (275–295 mmol/L) and impending and current dehydration group (>295 mmol/L). The relevant baseline characteristics of the two groups are shown in . The difference of serum osmotic pressure between the two groups was statistically significant (P<0.05). WBC, neutrophil count, serum creatinine, and blood glucose were significantly higher in the impending and current dehydration groups than in the normal hydration group (P<0.05). PLT of the euhydration group was significantly higher than that of the impending and current dehydration groups, and the difference was statistically significant (P<0.05). There was no significant difference in hemoglobin, albumin and lactic acid.
Table 2 Preoperative Laboratory Test Data of the Patients Grouped by Hydration Status
Intraoperative Clinical Data Characteristics of the Two Groups
As shown in , there was no statistically significant difference in operation duration, CPB duration, and aortic occlusion duration between the euhydration group and the impending and current dehydration group (P>0.05). Compared with the normal hydration group, patients in the impending and current dehydration groups received mechanical ventilation for a significantly longer time, with statistical significance (P<0.05).
Table 3 The Clinical Data of Intraoperative Patients Were Grouped by Hydration Status
Comparison of Postoperative Clinical Outcome Between the Two Groups
A postoperative hospital death in A AAD patients was significantly more common in the impending and current dehydration groups (>295mmol/L) (26.7% vs 11.9%; P=0.001) (see and ). As shown in , patients in the dehydration group were more likely to develop acute renal insufficiency than those in the euhydration group (26.7% vs 15.5%; P=0.017). The duration of ICU stay of patients in the impending and current dehydration groups was significantly higher than that in the euhydration group, and the difference was statistically significant (P<0.05). There were no significant differences in the incidence of acute renal insufficiency, gastrointestinal bleeding and MODS between the two groups.
Table 4 In-Hosiptal Outcomes After a AAD Surgery Were Grouped by Hydration Status
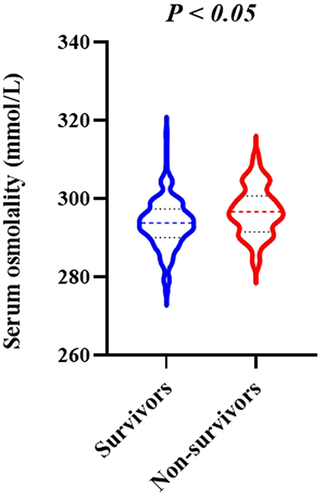
Figure 2 The violin plots for hydration status grouping in survivors group and non-survivors group.
Multivariate Logistic Regression Analysis Results
As shown in , the independent risk factors of postoperative hospital death in A AAD patients were further analyzed by logistic regression. Univariate logistic regression analysis showed that impending and current dehydration, serum albumin, age, smoking, LVEF, lactic acid and hemoglobin were correlated with in-hospital death (P<0.1), which may be risk factors for postoperative in-hospital death in A AAD patients. After multivariate logistic regression analysis, the results showed that impending dehydration and dehydration group (>295) (OR=3.61, 95% confidence interval (CI): 1.61–8.06; P=0.002), CRRT (OR=10.55, 95%(CI): 3.59–31.01; P<0.001), lactic acid (OR=1.25, 95%(CI): 1.13–1.38; P<0.001), CAD (OR=5.27, 95%(CI): 1.12–24.80; P=0.035) was an independent risk factor for in-hospital death in patients with A AAD, serum albumin (OR=0.92, 95%(CI): 0.85–0.99; P=0.040) was a protective factor for hospitalization outcomes.
Table 5 Determine the Factors Affecting in-Hospital Mortality by Univariate and Multivariate Logistic Regression Analysis
Discussion
To our knowledge, this is the first study to describe a significant relationship between impaired hydration status and mortality in patients with acute type A aortic dissection. The results of this study showed that patients with A AAD with high serum osmotic pressure (>295mmol/L) at admission were significantly associated with an increased risk of in-hospital mortality, and that high serum osmotic pressure (impending and current dehydration) remained independently associated with in-hospital mortality after adjustment for other factors. Arevalo et al reported in patients with heart failure that high osmotic pressure was associated with increased mortality and readmitted hospital admission, but the effect of low osmotic pressure was not significant.Citation21
The results of this study showed that patients with A AAD in the impending and current dehydration groups (>295mmol/L) were able to independently predict in-hospital death, which remained significant after multivariate adjustment for the effects of albumin, CRRT, smoking, lactic acid and other factors (P<0.05). A patients with A AAD usually require emergency surgical intervention, and postoperative survival remains poor. In this study, the postoperative patient mortality rate was 18.4%, which was approximately consistent with clinical statistics.Citation4 Many studies have confirmed that high serum osmolality may be associated with poor prognosis.Citation13 We also found that the mortality rate of A AAD patients in the impending and current dehydration group was significantly higher than that in the euhydration group, and the condition of high osmotic pressure was unfavorable for clinical results (), which was consistent with some research results.Citation12–14 The reasons may be as follows: first, changes in hyperosmolality are always accompanied by increases in its main components, such as hypersodium and hyperglycemia,Citation22 which have been reported as risk factors for increased cardiac mortality in patients, respectively. Mortality can be predicted based on specific disorders of certain laboratory parameters at the time of an emergency, often referred to as a “aggregation” effect.Citation23 Second, high osmotic pressure may cause the redistribution of body fluids, such as fluid accumulation into the effective circulation volume, thus increasing the cardiac preload, leading to a worse outcome. Third, changes in cell hydration may be a key factor in determining cell swelling or contraction, affecting the integrity of cell structure and function until apoptotic cell death.Citation24 Nag et al also reported in their study that higher serum osmotic pressure on admission was associated with early death and worse prognosis,Citation13 which was also confirmed by Bhalla et al ‘s study,Citation25 providing theoretical evidence for this study. At the same time, this study also found this correlation (see ). Overall, these results suggest that serum osmotic pressure has clinical significance in the development of A AAD and is an early prognostic factor for A AAD. Actively improving the hydration status of patients upon admission may be a new strategy for improving hospital survival of patients with A AAD in the future.
Another finding of this study was that we compared the differences in hospitalization outcomes between groups with different hydration states and found that mechanical ventilation and duration of stay in the ICU were significantly higher in A AAD patients (hyperoosmotic pressure) in the impending and current dehydration groups (see ). High osmotic pressure has a negative effect on mechanical ventilation, which may be caused by the reduced response of ventilators to metabolic acidosis under high osmotic pressure conditions.Citation21 This is consistent with the cross-sectional findings of Pogson et al.Citation26 However, another clinical investigation is paradoxical, showing that hypernatremia reflects the effect of osmotic pressure to some extent and is not associated with ICU mortality in patients with respiratory diseases.Citation27 This may be related to the complex regulation mechanism between serum osmotic pressure and lung function. In an earlier clinical trial of resuscitation of pre-hospital traumatic hypotension, hypertonic saline/dextran was found to be less common in acute lung injury than normal saline.Citation27 Administration of hypertonic saline can lead to hyperosmosis, save the inhibition of T cells by traumatic anti-inflammatory mediators, inhibit neutrophilic activation and reduce macrophage migration, preserve alveolar surfactants and weaken pulmonary neutrophilic isolation, thereby improving lung injury.Citation28 In addition, many studies have also shown that high osmotic pressure has a protective effect on the lung,Citation26,Citation29 which is different from our previous cognition. Of course, this needs to be verified by more prospective controlled studies in the future.
This study also found that high osmotic pressure had a significant adverse effect on postoperative AKI in patients with A AAD, and the incidence was significantly higher than that in the normal group (see ). In the study of Farhan et al, high serum osmotic pressure was positively correlated with the risk of postoperative AKI in patients receiving PCI,Citation30 and the incidence of AKI increased significantly with the increase of osmotic pressure, which was consistent with the results of this study. It is worth noting that there is A certain heterogeneity between the patients we included in A AAD surgery and PCI patients. However, in all studies, high serum osmolality was associated with an increased risk of long-term death, even after adjusting for baseline risk.Citation12–14,Citation31 This study is no exception, and the correlation between the two may not be independent of AKI, suggesting that the increased mortality associated with high osmotic pressure may be driven by the increased occurrence of postoperative AKI in patients with A AAD. The two are mutually reinforcing, which is worth further exploration.
What merits our special attention in this study is the question of how patients with A AAD transition from a hypovolemic state to a hypervolemic state. Because of the limitation of retrospective study for how to deal with this situation, the part of the data is blank at present. Studies by others have illustrated that the ideal treatment for this condition at the time of emergency admission in patients with A AAD has not been established.Citation32 This blood volume conversion process is complex and needs to be comprehensively considered according to the body condition of the A AAD patient and the needs of the surgical procedure. Therefore, how to better cooperate with clinicians and anesthesiologists to adjust and deal with the impaired hydration status of patients during the operation and monitor closely after the operation are the areas that we need to explore in the future research.
In clinical practice, for a single serum indicator, it may only reflect severe organ dysfunction or a disturbance of the overall homeostasis mechanism, especially sodium, glucose and urea. The strength of this study is that serum osmolality is an easily calculated measure based on data that is generally available for most hospitalized patients. The advantage of osmotic pressure calculations is that there is a good balance between simplicity and clinical practicality. In this study, calculated serum osmolality was used and an attempt was made to combine these variables in the calculation to predict postoperative hospitalization mortality in patients with A AAD (see ). All of these parameters are readily available to clinicians, and by defining a group with a much higher risk of death, the impact of an intervention can focus on investigating the impact of treatment on outcomes in that group. As an important supplement for clinical prognostic markers, it has great clinical significance. Online versions of the algorithms described in this report may be helpful in aiding clinical decision making.
Limitation
The study still has some limitations. First, we conducted a single-center retrospective analysis with a relatively small sample size, subsequent studies with larger samples are needed to support our conclusions. Secondly, because the data are from a retrospective study, it is not possible to effectively obtain the data of the conversion of A AAD patients from hypovolemic to hypervolemic state. Future research should continue to explore and explore effective conversion methods and their safety. Finally, in future prospective studies, low osmolality can be classified to facilitate the analysis of the effects of different osmolality levels on the postoperative prognosis of patients with A AAD, and to provide more clinical basis for medical staff to make clinical decisions.
Conclusions
The present study shows that high serum osmotic pressure is an independent predictor of in-hospital mortality in patients undergoing A AAD surgery, providing novel and robust evidence for a relationship between high serum osmotic pressure and the risk of death in patients undergoing A AAD surgery.
Disclosure
The authors report no conflicts of interest in this work.
Acknowledgments
The authors thank the Department of Cardiovascular Surgery, Union Hospital, Fujian Medical University. Yaqin Chen and Yanchun Peng are co-first authors.
Additional information
Funding
References
- Erbel R, Aboyans V, Boileau C, et al. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The task force for the diagnosis and treatment of aortic diseases of the European Society Of Cardiology (ESC) (published correction appears in. Eur Heart J. 2014;35(41):2873–2926. doi:10.1093/eurheartj/ehu281
- Benedetto U, Dimagli A, Kaura A, et al. Determinants of outcomes following surgery for type A acute aortic dissection: the UK national adult cardiac surgical audit. Eur Heart J. 2021;43(1):44–52. doi:10.1093/eurheartj/ehab586
- Nienaber CA, Eagle KA. Aortic dissection: new frontiers in diagnosis and management: part I: from etiology to diagnostic strategies. Circulation. 2003;108(5):628–635. doi:10.1161/01.CIR.0000087009.16755.E4
- Pape LA, Awais M, Woznicki EM, et al. Presentation, diagnosis, and outcomes of acute aortic dissection: 17-year trends from the international registry of acute aortic dissection. J Am Coll Cardiol. 2015;66(4):350–358. doi:10.1016/j.jacc.2015.05.029
- Evangelista A, Isselbacher EM, Bossone E, et al. Insights from the international registry of acute aortic dissection: a 20-year experience of collaborative clinical research. Circulation. 2018;137(17):1846–1860. doi:10.1161/CIRCULATIONAHA.117.031264
- Buaprasert P, Piyapaisarn S, Vanichkulbodee A, Kamsom A, Sri-On J. Prevalence and risk factors of hypertonic dehydration among older patients admitted to the emergency department: a prospective cross-sectional study. Geriatr Gerontol Int. 2021;21(6):485–491. doi:10.1111/ggi.14168
- Schrock JW, Glasenapp M, Drogell K. Elevated blood urea nitrogen/creatinine ratio is associated with poor outcome in patients with ischemic stroke. Clin Neurol Neurosurg. 2012;114(7):881–884. doi:10.1016/j.clineuro.2012.01.031
- Erbel R, Aboyans V, Boileau C, et al. Corrigendum to: 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases. Eur Heart J. 2015;36(41):2779. doi:10.1093/eurheartj/ehv178
- Girdauskas E, Kuntze T, Borger MA, Falk V, Mohr FW. Surgical risk of preoperative malperfusion in acute type A aortic dissection. J Thorac Cardiovasc Surg. 2009;138(6):1363–1369. doi:10.1016/j.jtcvs.2009.04.059
- Cheuvront SN, Kenefick RW. Dehydration: physiology, assessment, and performance effects. Compr Physiol. 2014;4(1):257–285 doi:10.1002/cphy.c130017.
- Gorelick MH, Shaw KN, Baker MD. Effect of ambient temperature on capillary refill in healthy children. Pediatrics. 1993;92(5):699–702. doi:10.1542/peds.92.5.699
- Rohla M, Freynhofer MK, Tentzeris I, et al. Plasma osmolality predicts clinical outcome in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Eur Heart J Acute Cardiovasc Care. 2014;3(1):84–92. doi:10.1177/2048872613516018
- Nag C, Das K, Ghosh M, Khandakar MR. Plasma osmolality in acute spontaneous intra-cerebral hemorrhage: does it influence hematoma volume and clinical outcome? J Res Med Sci. 2012;17(6):548–551.
- Shen Y, Cheng X, Ying M, Chang HT, Zhang W. Association between serum osmolarity and mortality in patients who are critically ill: a retrospective cohort study. BMJ Open. 2017;7(5):e015729. doi:10.1136/bmjopen-2016-015729
- Hooper L, Abdelhamid A, Attreed NJ, et al. Clinical symptoms, signs and tests for identification of impending and current water-loss dehydration in older people. Cochrane Database Syst Rev. 2015;2015(4):CD009647. doi:10.1002/14651858.CD009647.pub2
- El-Sharkawy AM, Devonald MAJ, Humes DJ, Sahota O, Lobo DN. Hyperosmolar dehydration: a predictor of kidney injury and outcome in hospitalised older adults. Clin Nutr. 2020;39(8):2593–2599. doi:10.1016/j.clnu.2019.11.030
- Hooper L, Abdelhamid A, Ali A, et al. Diagnostic accuracy of calculated serum osmolarity to predict dehydration in older people: adding value to pathology laboratory reports. BMJ Open. 2015;5(10):e008846. doi:10.1136/bmjopen-2015-008846
- Farhan S, Vogel B, Baber U, et al. Calculated serum osmolality, acute kidney injury, and relationship to mortality after percutaneous coronary intervention. Cardiorenal Med. 2019;9(3):160–167. doi:10.1159/000494807
- Garrett DC, Rae N, Fletcher JR, et al. Engineering Approaches to Assessing Hydration Status. IEEE Rev Biomed Eng. 2018;11:233–248. doi:10.1109/RBME.2017.2776041
- Khajuria A, Krahn J. Osmolality revisited--deriving and validating the best formula for calculated osmolality. Clin Biochem. 2005;38(6):514–519. doi:10.1016/j.clinbiochem.2005.03.001
- Arévalo-Lorido JC, Gómez JC, Formiga F, et al. High serum osmolarity at admission determines a worse outcome in patients with heart failure: is a new target emerging? Int J Cardiol. 2016;221:238–242. doi:10.1016/j.ijcard.2016.07.084
- Cole E, Gillespie S, Vulliamy P, Brohi K. Organ Dysfunction in Trauma (ORDIT) study collaborators. Multiple organ dysfunction after trauma. Br J Surg. 2020;107(4):402–412. doi:10.1002/bjs.11361
- Nicholson T, Bennett K, Silke B. Serum osmolarity as an outcome predictor in hospital emergency medical admissions. Eur J Intern Med. 2012;23(2):e39–e43. doi:10.1016/j.ejim.2011.06.014
- Mattox KL, Maningas PA, Moore EE, et al. Prehospital hypertonic saline/dextran infusion for post-traumatic hypotension. The U.S.A. Multicenter Trial. Ann Surg. 1991;213(5):482–491. doi:10.1097/00000658-199105000-00014
- Bhalla A, Sankaralingam S, Dundas R, Swaminathan R, Wolfe CD, Rudd AG. Influence of raised plasma osmolality on clinical outcome after acute stroke. Stroke. 2000;31(9):2043–2048. doi:10.1161/01.STR.31.9.2043
- Pogson ZE, McKeever TM, Fogarty A. The association between serum osmolality and lung function among adults. Eur Respir J. 2008;32(1):98–104. doi:10.1183/09031936.00144207
- Bihari S, Peake SL, Bailey M, Pilcher D, Prakash S, Bersten A. Admission high serum sodium is not associated with increased intensive care unit mortality risk in respiratory patients. J Crit Care. 2014;29(6):948–954. doi:10.1016/j.jcrc.2014.06.008
- Chen L, Liu C, Liu L. Osmolality-induced tuning of action potentials in trigeminal ganglion neurons. Neurosci Lett. 2009;452(1):79–83. doi:10.1016/j.neulet.2009.01.022
- Schliess F, Häussinger D. The cellular hydration state: a critical determinant for cell death and survival. Biol Chem. 2002;383(3–4):577–583. doi:10.1515/BC.2002.059
- Murao Y, Loomis W, Wolf P, Hoyt DB, Junger WG. Effect of dose of hypertonic saline on its potential to prevent lung tissue damage in a mouse model of hemorrhagic shock. Shock. 2003;20(1):29–34. doi:10.1097/01.shk.0000071060.78689.f1
- Smith GB, Prytherch DR, Schmidt PE, Featherstone PI. Predictive models: the angel is in the details. Crit Care Med. 2009;37(11):2997–2998. doi:10.1097/CCM.0b013e3181b4a15c
- Czerny M, Schoenhoff F, Etz C, et al. The impact of pre-operative malperfusion on outcome in acute type a aortic dissection: results from the GERAADA registry. J Am Coll Cardiol. 2015;65(24):2628–2635. doi:10.1016/j.jacc.2015.04.030