
Abstract
Purpose
This study was aimed at exploring the use of the acute gastrointestinal injury (AGI) grade and sensitive biomarkers to investigate gastrointestinal (GI) injury in early stage of acute pancreatitis (AP).
Patients and Methods
The AGI grade was used to evaluate intestinal function. Any GI injury above grade I (grades II–IV) was considered as severe. An AP rat model was created by retrograde injection of 4% sodium taurocholate. The pancreatic and intestinal histopathology scores were calculated by hematoxylin-eosin staining. Human and rat sera were assessed using ELISA. Tight junction (TJ) proteins were detected by Western blotting.
Results
In clinical study, the GI injury rate in mild acute pancreatitis (MAP), moderate severe acute pancreatitis (MSAP), and severe acute pancreatitis (SAP) groups was 26.8%, 78.4%, and 94.8%, respectively (P < 0.05). Diamine oxidase (DAO), histidine decarboxylase (HDC), and matrix metalloproteinase 8 (MMP8) serum levels were higher in AP patients than in healthy people (P < 0.05). Patients with GI injury had higher serum levels of DAO, HDC, and MMP8 than those without GI injury (P < 0.05). In animal experiments, the serum levels of DAO, HDC, and MMP8 were higher in the AP group than in normal and sham-operated (SO) groups (P < 0.05). The expressions of tricellulin, claudin-1, ZO-1, and occludin were significantly lower in the AP group than in normal and SO groups (P < 0.05).
Conclusion
The serum levels of DAO, HDC, and MMP8 are novel biomarkers of GI injury in the early stage of AP; their elevation indicates the development of GI injury in AP. The intestinal TJ disruption may be a primary mechanism of GI injury and requires more in-depth research.
Introduction
Acute pancreatitis (AP) is among the most prevalent gastrointestinal (GI) conditions requiring hospitalization. It has a global incidence of ~34 per 100,000 person-years,Citation1 and studies indicate that the rate is increasing worldwide.Citation2 The updated Atlanta classification categorizes AP as mild, moderate, and severe.Citation3 Although the majority of people have mild acute pancreatitis (MAP), ~20% individuals develop moderate severe acute pancreatitis (MSAP) or severe acute pancreatitis (SAP) with pancreatic necrosis, peripancreatic tissue necrosis, and/or organ failure.Citation4,Citation5
Intestinal mucosal barrier dysfunction is considered a major trigger of systemic inflammatory response syndrome (SIRS) and multiple organ dysfunction (MOF) in AP patients, and intestinal barrier injury is a common complication in AP patients.Citation6 Intestinal bacterial translocation, pancreatic tissue necrosis and infection, and the beginning of multiple organ dysfunction syndrome are all caused by increased intestinal mucosal permeability.Citation7 However, Acute Physiology and Chronic Health Evaluation (APACHE) II and Sequential Organ Failure Assessment are two examples of current clinical scoring systems that have little efficacy in predicting the severity of AP.Citation8 The European Society of Intensive Care Medicine suggested the acute gastrointestinal injury (AGI) grade as more precise and detailed evaluation criteria.Citation9 The AGI grade can be used to assess the degree of GI damage and predict severity and adverse clinical outcomes in critical patients.Citation10 However, the AGI grade is a score criterion based on clinical presentation with some lag, and serum markers for early prediction of AGI are currently unclear.
Several serum indicators may be used to predict AGI prognosis. Diamine oxidase (DAO), a cytoplasmic enzyme, is reportedly a reliable indicator of intestinal mucosal injury in both humans and rats.Citation11,Citation12 The primary effect of histidine decarboxylase (HDC) is histamine production, which exhibits HDC activity in almost all adult mammalian tissues, and HDC may also play a role in tissue healing after gastrointestinal ischemic injury.Citation13 HDC is commonly induced at the inflammation site during the late and chronic phases of both allergic and non-allergic inflammation.Citation14 Matrix metalloproteinases (MMPs) are a class of endopeptidases that catalyze the degradation of extracellular matrix proteins. It has been experimentally demonstrated that MMPs can enhance the activity of pro-inflammatory cytokines, thereby promoting inflammatory processes.Citation15 Twenty-three MMPs that are released into the extracellular space by cells have been identified.Citation16 MMP-1, MMP-7, MMP-8, TIMP-1, and TIMP-4 levels were higher in the AP group than in the control group.Citation17 Injury to the intestinal mucosal barrier plays a crucial role in the mechanism of gastrointestinal dysfunction. Dysregulated tight junctions (TJs) and their protein interactions regulate paracellular permeability between intestinal epithelial cells in SAP.Citation18 The occurrence of anomalous apoptosis or proliferation of the intestinal epithelial cells may result in augmented permeability of the intestinal barrier.Citation19 The intestinal barrier comprises a layer of epithelial cells connected by TJ proteins, including occludin, claudin, and ZO-1. Intestinal pathogens, endotoxins, and some harmful factors constantly interact with the intestinal epithelium, which can induce inflammation and oxidative stress.Citation20 The disruption of intestinal barrier will increase intestinal permeability. Expression of claudin-1, ZO-1, and occludin reportedly decreases in response to acute pancreatitis and intestinal injury, thus altering intercellular TJs and facilitating intestinal microbiota translocation.Citation21,Citation22 Inflammatory responses, programmed necrosis, and reactive oxygen species accumulation have been identified as significant factors in the exacerbation of intestinal barrier damage induced by SAP in the context of a high-fat diet.Citation23 Previous studies showed that angiopoietin-2 and trefoil factor-2 may be the biomarkers of AGI in small sample data.Citation24,Citation25 Thus, effective predictors of GI injury in the early stages of AP remain lacking.
In this study, we focused on clinical AGI grade and sensitive biomarkers to investigate GI injury in patients with AP in the first 24 h after hospitalization. Furthermore, we used an animal model to investigate the predictive accuracy of these biomarkers in the early stage of AP and to identify putative mechanisms underlying the expression of TJ proteins in GI injury.
Materials and Methods
Patients and Diagnostic Criteria
This was a retrospective cohort study analyzing patients with AP admitted to the Second Affiliated Hospitals of Guangxi Medical University (Nanning, China) from January 2017 to July 2022 within 72 h of AP onset. Ethical approval of the research protocol was granted by the Ethics Committee of the Second Affiliated Hospitals of Guangxi Medical University [2017-KY (0120)], all methods were carried out in accordance with relevant guidelines and regulations. The committee waived the need for written informed consent considering the retrospective nature of the study. The diagnostic criteria for AP were in accordance with the 2012 revision of the Atlanta classification.Citation3 The diagnosis of AP necessitates the presence of any two out of the following three characteristics: (1) The patient experienced a sudden and severe onset of persistent pain in the upper central region of the abdomen, which frequently spread to the back; (2) the activity of serum lipase or amylase is at least three times higher than the upper limit of normal; and (3) typical observations are preferably made using computed tomography (CT) instead of magnetic resonance imaging or transabdominal ultrasonography. Patient exclusion criteria were as follows: (1) age <18 years, (2) ongoing pregnancy, and (3) a diagnosis of chronic pancreatitis. All clinical information of patients who met the inclusion criteria were collected.
Data Collection and Study Design
Clinical data and blood samples were collected in the first 24 h of hospitalization. Data were collected on baseline clinical characteristics of patients, including age, sex, body mass index, levels of white blood cells, hemoglobin (HB), hematocrit (HCT), total bilirubin (TBil), albumin (Alb), alanine aminotransferase (ALT), aspartate aminotransferase (AST), glutamyl transpeptidase (GGT), alkaline phosphatase (ALP), blood urea nitrogen, creatinine (Cr), lactate dehydrogenase (LDH), K+, Ca2+, and triglyceride (TG). Four scoring systems were used for all patients: APACHE-II, Ranson, Bedside Index of Severity in Acute Pancreatitis (BISAP), and modified CT severity index (mCTSI). The AGI grades and their application to AP patients were defined and exemplified by Ling Ding et al.Citation7 According to this grade, any GI injury above grade I (grades II–IV) was considered as severe. Throughout the assessment interval (the duration necessary for the scoring mechanism to monitor), all assessments were computed for the most critical laboratory examinations and physiological parameters. A control group was established by retaining serum samples from 20 individuals who were in good health.
Animals and Experimental Design
Fifty-four male Sprague–Dawley rats (6–8 weeks old) were obtained from the Laboratory Animal Center of Guangxi Medical University (Nanning, China). Rats were housed at 24°C with a 12/12-h light–dark cycle and had ad libitum access to food and water. The present investigation was performed in compliance with the Animal Protection Guidelines sanctioned by the regional animal ethics committee. Our animal care and welfare protocol was approved by the committee responsible for such matters at Guangxi Medical University. Rats were randomly divided into three groups, namely the normal group (N, n = 6), sham-operated group (SO, n = 24), and AP group (AP, n = 24). All animals were starved for 12 h before the surgical procedures. Retrograde injection of 4% sodium taurocholate into the bile and pancreatic duct was used to establish the AP model. The pancreas and duodenum of the rats in the SO group were inverted and returned to the original position after laparotomy. Rats were euthanized at 0, 6, 12, and 24 h after AP induction or sham operation. Serum was stored at −80°C after abdominal aorta blood samples were centrifuged at 500 g for 15 min. A second part of pancreases and intestinal tissues were preserved in 10% formalin, paraffin-embedded, and used for H&E staining.
Histopathologic Analysis
Morphological analyses were performed by two expert researchers who were blinded to the experimental conditions. Alterations in pancreatic histopathology were assessed and categorized on the basis of the methodology outlined by Van Laethem.Citation26 Changes in intestinal histopathology were examined and classified using the Chiu’s score.Citation27
ELISA Assay
The levels of HDC (Cloud-Clone, Wuhan, China), DAO (Cloud-Clone, Wuhan, China), and MMP8 (Cusabio, Wuhan, China) in patient and rat serum were measured using the ELISA standard procedures.
Western Blotting Analysis
Total protein was extracted using a high-efficiency radio immunoprecipitation assay lysis buffer (Solarbio, China) containing a protease inhibitor cocktail (NCM, China) and quantified using a bicinchoninic acid protein concentration assay kit (NCM, China). Electrophoresis was performed on 10% or 12% sodium dodecyl sulfate-polyacrylamide gels and then, the proteins were transferred to polyvinylidene fluoride membrane (Millipore, USA). The membrane was blocked with 5% skimmed milk at 22°C for 1 h. The membrane with proteins was incubated with primary antibodies against GAPDH (1:5000 dilution, Abcam, USA), tricellulin (1:1000 dilution, ABclonal, Wuhan, China), claudin-1 (1:800 dilution, Proteintech, Wuhan, China), ZO-1 (1:1000 dilution, Proteintech, Wuhan, China), and occludin (1:800 dilution, Proteintech, Wuhan, China) overnight at 4°C. Subsequently, the membrane was incubated with a secondary antibody (1:10,000, Cell Signaling Technology, USA) at 22°C for 1 h. Protein bands were visualized using the Odyssey infrared laser imaging system (Licor, USA), and the quantification was performed using the Quantity One software (Bio-Rad Laboratories).
Statistical Analyses
The data are presented as mean ± standard deviation (mean ± SD), and categorical variables are expressed as the means (ratios). SPSS 20.0 (IBM SPSS, Armonk, NY, USA) statistical software was used for data analysis. Using one-way analysis of variance and the Bonferroni post-hoc test, differences between multiple groups were determined. Categorical variables were evaluated using a χ2 test, and Fisher’s exact test was used when the number of observations was <5. The predictive accuracy of each scoring system was determined by the area under the receiver operating characteristic (ROC) curve with a 95% confidence interval. Area under the curve (AUC) values were compared using the Z test to determine statistical significance. A P value of <0.05 indicated statistical significance.
Results
Baseline Characteristics of AP Patients
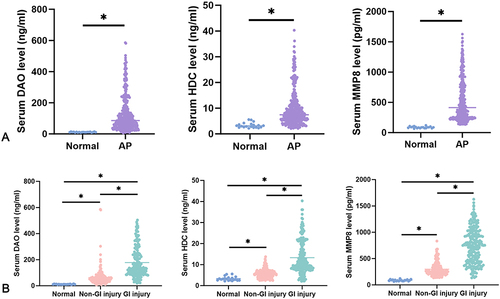
A total of 388 AP patients were included in this study. shows baseline characteristics for individuals classified according to AP severity. According to the severity of AP, there were 209 patients with MAP, 102 patients with MSAP, and 77 patients with SAP. Patients with MSAP were younger (46.14 ± 15.66 years) than those with MAP (P < 0.05). MAP was caused by gallstones in most cases. The APACHE-II scores were significantly higher in the SAP group than in MAP and MSAP groups (P < 0.05, respectively); the BISAP scores were higher in the SAP group than in the MAP group (P < 0.05). In addition, the mCTSI scores were considerably higher in the SAP group than in MAP and MSAP groups (P < 0.05, separately), and the mCTSI scores were significantly higher in the MSAP group than in the MAP group (P < 0.05; ). The SAP group had a greater risk of GI injury than the other groups, with GI injury rates of 26.8%, 78.4%, and 94.8%, respectively (χ2 = 154.805, P < 0.05; ). In the MAP group, there were 153 patients with AGI I grade and 56 patients with AGI II grade, and in the MSAP group, there were 22 patients with AGI I grade, 73 patients with AGI II grade, and 7 patients with AGI III grade. The SAP group had four patients with AGI I grade, 28 patients with AGI II grade, 41 patients with AGI III grade, and 4 patients with AGI IV grade. The serum DAO, HDC, and MMP8 levels were significantly higher in the AP group than in the control group (P < 0.05; ). The serum DAO, HDC, and MMP8 levels were higher in the SAP group than in MAP and MSAP groups (P < 0.05, separately), and they were higher in the MSAP group than in the MAP group (P < 0.05).
Table 1 Clinical Characteristics of AP Patients in the Early Stage
Table 2 The GI Injury in Different Severe of AP Patients
Figure 1 Serum HDC, DAO and MMP8 levels in healthy controls and patients in each group. (A) Serum DAO, HDC, and MMP8 levels were significantly higher in AP patients than in healthy controls. (B) Serum levels of DAO, HDC, and MMP8 were higher in GI injury patients than in non-GI injury patients.
The Serum DAO, HDC, and MMP8 Levels in AP Patients with Different AGI Grade
There were 179 patients with AGI I grade, 157 patients with AGI II grade, 48 patients with AGI III grade, and 4 patients with AGI IV grade ( and ). There were 209 patients in the GI injury group and 179 patients in the non-GI injury group. The serum levels of DAO, HDC, and MMP8 were higher in the former than in the latter (178.15 ± 115.71 vs 63.12 ± 68.19 ng/mL, 13.31 ± 7.86 vs 5.76 ± 2.10 ng/mL, and 738.82 ± 335.31 vs 297.83 ± 126.66 pg/mL, P < 0.05, respectively; and ).
Table 3 Serum HDC, DAO, and MMP8 Levels in AP Patients with Different AGI Class
Histopathological Analysis of Pancreatic and Intestinal Tissues
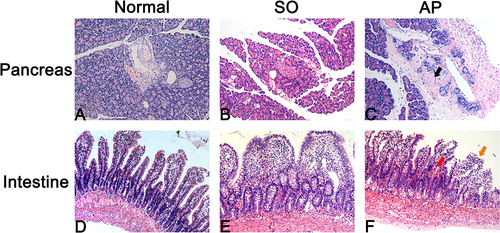
Edema, hemorrhage, inflammation, and necrosis were observed in the pancreas in the AP group (). Edema, hemorrhage, loss in the apex of the villus, massive detachment of the epithelium down the sides of villi, and chyladenectasis were detected in the AP group (), and the Histological Scores for Intestinal Damage (HSID) were statistically higher in the AP group than in normal and SO groups at the same time point (P < 0.05; ).
Table 4 The Intestinal Score, Serum HDC, DAO, and MMP8 Levels in AP Rats
Figure 2 Pancreas and intestinal injury in AP rats. (A–C) Edema, hemorrhage, inflammation, and necrosis were observed in the pancreas in the AP group. (D–F) Edema, hemorrhage, loss in the apex of the villus, massive epithelial lifting down the sides of villi, and chyladenectasis were detected in the AP group.
The Serum DAO, HDC, and MMP8 Levels in AP Rats
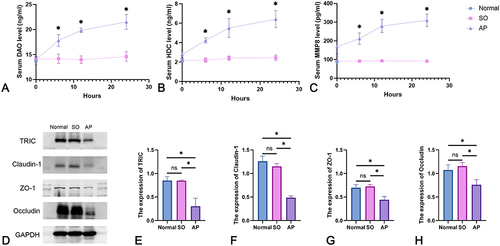
The serum level of DAO was higher in the AP group than in the SO group at 6 h, 12 h, and 24 h (17.82 ± 1.18 vs 14.16 ± 0.93 ng/mL, 19.83 ± 0.44 vs 13.98 ± 0.76 ng/mL, and 21.52 ± 1.48 vs 14.61 ± 0.98 ng/mL, respectively; P < 0.05 at all time points, ). The serum levels of HDC were higher in the AP group than in the SO group at 6 h, 12 h, and 24 h (4.23 ± 0.27 vs 2.19 ± 0.21 ng/mL, 5.51 ± 0.97 vs 2.41 ± 0.21 ng/mL, and 6.42 ± 0.88 vs 2.44 ± 0.28 ng/mL, respectively; P < 0.05 at all time points, ). The serum levels of MMP8 were also higher in the AP group than in the SO group at 0 h, 6 h, 12 h, and 24 h (169.00 ± 38.04 vs 90.51 ± 1.08 pg/mL, 211.71 ± 30.95 vs 91.72 ± 1.86 pg/mL, 279.50 ± 35.38 vs 92.77 ± 1.95 pg/mL, and 309.42 ± 33.80 vs 91.43 ± 1.53 pg/mL, respectively; P < 0.05 at all time points, ).
Figure 3 Serum DAO, HDC, and MMP8 levels and tight junction protein expression in AP rats. (A–C) Serum DAO, HDC, and MMP8 levels were higher in the AP group than in the normal group and SO group at the same point of time. (D) Western blot for tricellulin, claudin-1, ZO-1, and occludin in the intestinal mucosa of rats. (E–H) The expression of tricellulin, claudin-1, ZO-1, and occludin was significantly decreased in the AP group than in the normal group and SO group.
The Expressions of Tricellulin, Claudin-1, ZO-1, and Occludin in Rat’s Intestinal
According to the HSID, the expression of proteins was detected 24 h after the establishment of the AP model. The expression of tricellulin, claudin-1, ZO-1, and occludin were significantly decreased in the AP group than in the normal group and SO group (P < 0.05; ).
The Serum DAO, HDC, and MMP8 Level and GI Injury in AP Patients
The predictive value of DAO, HDC, and MMP8 in GI injury in AP patients was assessed using ROC curves (). The AUCs of DAO, HDC, and MMP8 ROCs were 0.879 [95% CI (0.844, 0.915)], 0.854 [95% CI (0.815, 0.894)], and 0.898 [95% CI (0.867, 0.929)], respectively.
Figure 4 Prediction of GI injury using ROC of serum HDC, DAO, and MMP8 levels. The areas under the ROCs of DAO, HDC, and MMP8 were 0.879 [95% CI (0.844, 0.915)], 0.854 [95% CI (0.815, 0.894)], and 0.898 [95% CI (0.867, 0.929)], respectively.
![Figure 4 Prediction of GI injury using ROC of serum HDC, DAO, and MMP8 levels. The areas under the ROCs of DAO, HDC, and MMP8 were 0.879 [95% CI (0.844, 0.915)], 0.854 [95% CI (0.815, 0.894)], and 0.898 [95% CI (0.867, 0.929)], respectively.](/cms/asset/316707b6-43e7-4e80-a8c3-bb5f8c00d30b/dijg_a_12302521_f0004_c.jpg)
Discussion
Acute pancreatitis is considered an inflammatory disorder of the pancreas. SAP would be life-threatening, with mortality rates as high as 30%. Although patients with MAP typically recover completely, SAP would be fatal.Citation2 GI injury is present in nearly half of patients with AP and is an independent predictor of mortality.Citation28 In this study, the SAP group had higher APACHE-II and BISAP scores than the MSAP group and MAP group, but there was no significant difference in Ranson scores among these three groups. These results indicated that these scoring systems are inadequate for identifying severe AP at an early stage. The mCTSI scores were the highest in the SAP group, followed by the MSAP group and the MAP group, indicating a high-performance diagnostic value for the severity of AP. Conversely, the rate of GI injury was the highest in the SAP group. This result indicated that GI injury is the most prevalent among SAP patients.
Although many biomarkers have been used for the diagnosis of human intestinal injury, including intestinal fatty acid binding protein (I-FABP), interleukin-6 (IL-6), C-reactive protein, and serum amyloid A (SAA), none of these biomarkers is superior to others,Citation29 and no single biomarker has been found to be particularly accurate for GI injury.Citation30 This study found no predictive value of routine blood tests for GI injury. Therefore, more biomarkers to predict the efficacy of GI injury in the early stage of AP need to be identified. DAO is localized in the mucosa and shows high activity in the small intestine, and serum DAO levels indicate the maturity and integrity of the intestinal mucosa.Citation31 Several previous studies have reported that increasing serum DAO levels indicate intestinal mucosal damage.Citation11 The enzyme HDC has been identified as the exclusive catalyst for histamine biosynthesis.Citation31 Numerous investigations have revealed that the activity of HDC is heightened in swiftly dividing tissues, including the fetal tissues of rodents, tissues undergoing the process of mending, and the regeneration of the liver after hepatectomy. Another study suggested that HDC plays a pivotal role in tissue regeneration and restoration of mucosal function following ischemia–reperfusion (I/R) injury.Citation13 Therefore, HDC has been identified as a prospective biomarker for assessing intestinal mucosal injury in individuals with acute intestinal obstruction.Citation32 In the present study, the serum levels of DAO and HDC showed direct correlation with the increasing severity of AP in the first 24 h after hospitalization and more significantly in GI injury, and these levels then increased by 6 h after AP in animal studies. Furthermore, we found that early serum levels of DAO and HDC predicted GI injury with a higher diagnostic yield accuracy as the AUCs of DAO and HDC were 0.879 [95% CI (0.844, 0.915)] and 0.854 [95% CI (0.815, 0.894)], respectively. Several studies have shown that MMPs are released in response to distant organ injury in AP animal models.Citation33,Citation34 Previous research has reported elevated MMP-9 levels in individuals who manifest SAP within 48 h of hospitalization. The AP group had higher MMP levels than the control group, with MMP-8 serving as a predictor of SAP.Citation17 In this study, we found that the serum level of MMP8 was significantly elevated in the early stages of AP and that MMP8 was elevated at as early as 6 h after AP in animal models, thus providing a better AUC for predicting GI injury in clinical studies. This study partly compensates for the paucity of serological markers of early prediction of GI injury in AP.
The mechanism of GI disruption in AP remains uncertain. Gut barrier dysfunction may be the main pathogenic mechanism. Intestinal barrier dysfunction increases pro-inflammatory factors in the blood, causing SIRS, secondary infection of necrotic pancreas, and multiorgan dysfunction.Citation35 The tight junction is a permeable and dynamic barrier between intestinal epithelial cells. The downregulation of TJ proteins, namely claudin-1, ZO-1, and occludin alters the tight junctions between cells and facilitates the translocation of intestinal microflora. Recent scientific research has demonstrated that TJ proteins, which are crucial constituents of the intestinal mucosal barrier, are indicative of changes in intestinal mucosal function.Citation36–38 Inflammatory reactions, necroptosis, and oxidative stress were considered as principal factors in SAP-induced intestinal barrier injury.Citation23 The expression of tricellulin, claudin-1, ZO-1, and occludin was significantly reduced in AP rodents, according to this study. Our study demonstrated that TJ proteins not only the bicellular TJs but also tricellular TJs, were damaged in AP.
This investigation possesses both strengths and limitations. Our study identified that serum DAO, HDC, and MMP8 levels can be new biomarkers of GI injury in the early stage of AP and that intestinal TJ disruption may be a major mechanism of GI injury. The study conducted was limited to a single center and had a relatively small sample size. Furthermore, there were no detailed molecular mechanistic investigations conducted on animal models. To enhance the robustness of our findings, it is imperative that we increase the sample size and further investigate additional molecular mechanisms in future studies.
Conclusion
Our investigation revealed that the serum levels of DAO, HDC, and MMP8 predicted GI injury with a higher diagnostic yield accuracy, and they can serve as novel biomarkers for GI injury in the initial phase of AP. Furthermore, the impairment of intestinal TJs could be a crucial mechanism behind GI injury and requires more in-depth research.
Abbreviations
AGI, acute gastrointestinal injury; GI, gastrointestinal; AP, acute pancreatitis; TJ, tight junction; MAP, mild acute pancreatitis; MSAP, moderate severe acute pancreatitis; SAP, severe acute pancreatitis; DAO, diamine oxidase; HDC, histidine decarboxylase; MMP8, matrix metalloproteinase 8; ROC, receiver operating characteristic; SO, sham-operated group; SIRS, systemic inflammatory response syndrome; APACHE, Acute Physiology, and Chronic Health Evaluation; MMPs, matrix metalloproteinases; BISAP, Bedside Index of Severity in Acute Pancreatitis; mCTSI, Modified CT severity index; AUC, area under the curve; HSID, Histological Scores for Intestinal Damage.
Statement of Ethics
The study complied with the Declaration of Helsinki. This study protocol was reviewed and approved by the Ethics Committee of the Second Affiliated Hospitals of Guangxi Medical University, approval number [2017-KY (0120)]. The requirement for written informed consent was waived due to the retrospective nature of the study. We declare that we will maintain the confidentiality of the patients’ personal information.
Disclosure
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- Xiao AY, Tan ML, Wu LM, et al. Global incidence and mortality of pancreatic diseases: a systematic review, meta-analysis, and meta-regression of population-based cohort studies. Lancet Gastroenterol Hepatol. 2016;1(1):45–55. doi:10.1016/S2468-1253(16)30004-8
- Hazra N, Gulliford M. Evaluating pancreatitis in primary care: a population-based cohort study. Br J Gen Pract. 2014;64(622):e295–301. doi:10.3399/bjgp14X679732
- Banks PA, Bollen TL, Dervenis C, et al. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013;62(1):102–111. doi:10.1136/gutjnl-2012-302779
- Schepers NJ, Bakker OJ, Besselink MG, et al. Impact of characteristics of organ failure and infected necrosis on mortality in necrotising pancreatitis. Gut. 2019;68(6):1044–1051. doi:10.1136/gutjnl-2017-314657
- Bang JY, Wilcox CM, Arnoletti JP, Varadarajulu S. Superiority of endoscopic interventions over minimally invasive surgery for infected necrotizing pancreatitis: meta-analysis of randomized trials. Dig Endosc. 2020;32:298–308. doi:10.1111/den.13470
- Capurso G, Zerboni G, Signoretti M, et al. Role of the gut barrier in acute pancreatitis. J Clin Gastroenterol. 2012;46:S46–51. doi:10.1097/MCG.0b013e3182652096
- Ding L, Chen HY, Wang JY, et al. Severity of acute gastrointestinal injury grade is a good predictor of mortality in critically ill patients with acute pancreatitis. World J Gastroenterol. 2020;26:514–523. doi:10.3748/wjg.v26.i5.514
- Vincent JL, Opal SM, Marshall JC. Ten reasons why we should NOT use severity scores as entry criteria for clinical trials or in our treatment decisions. Crit Care Med. 2010;38(1):283–287. doi:10.1097/CCM.0b013e3181b785a2
- Reintam Blaser A, Malbrain ML, Starkopf J, et al. Gastrointestinal function in intensive care patients: terminology, definitions and management. Recommendations of the ESICM Working Group on Abdominal Problems. Intensive Care Med. 2012;38:384–394. doi:10.1007/s00134-011-2459-y
- Hu B, Sun R, Wu A, et al. Severity of acute gastrointestinal injury grade is a predictor of all-cause mortality in critically ill patients: a multicenter, prospective, observational study. Crit Care. 2017;21(1):188. doi:10.1186/s13054-017-1780-4
- Tanaka Y, Mizote H, Asakawa T, et al. Clinical significance of plasma diamine oxidase activity in pediatric patients: influence of nutritional therapy and chemotherapy. Kurume Med J. 2003;50(3/4):131–137. doi:10.2739/kurumemedj.50.131
- Akimoto T, Takada M, Ichihara T, Kuroda Y. Molecular analysis for differential diagnosis of small bowel obstruction: expression of proinflammatory cytokines and diamine oxidase activity. Int J Biomed Sci. 2006;2:160–165. doi:10.59566/IJBS.2006.2160
- Fujimoto K, Imamura I, Granger DN, Wada H, Sakata T, Tso P. Histamine and histidine decarboxylase are correlated with mucosal repair in rat small intestine after ischemia-reperfusion. J Clin Invest. 1992;89:126–133. doi:10.1172/JCI115552
- Hirasawa N. Expression of Histidine Decarboxylase and Its Roles in Inflammation. Int J Mol Sci. 2019;20. doi:10.3390/ijms20020376
- Fic P, Zakrocka I, Kurzepa J, Stepulak A. Matrix metalloproteinases and atherosclerosis. Postepy Hig Med Dosw. 2011;65:16–27. doi:10.5604/17322693.931536
- Kurzepa J, Madro A, Czechowska G, et al. Role of MMP-2 and MMP-9 and their natural inhibitors in liver fibrosis, chronic pancreatitis and non-specific inflammatory bowel diseases. Hepatobiliary Pancreat Dis Int. 2014;13:570–579. doi:10.1016/S1499-3872(14)60261-7
- Vitale DS, Lahni P, Hornung L, et al. Matrix metalloproteinases and their inhibitors in pediatric severe acute pancreatitis. PLoS One. 2022;17(2):e0261708. doi:10.1371/journal.pone.0261708
- Galipeau HJ, Verdu EF. The complex task of measuring intestinal permeability in basic and clinical science. Neurogastroenterol Motil. 2016;28(7):957–965. doi:10.1111/nmo.12871
- He L, Liu T, Shi Y, et al. Gut Epithelial Vitamin D Receptor Regulates Microbiota-Dependent Mucosal Inflammation by Suppressing Intestinal Epithelial Cell Apoptosis. Endocrinology. 2018;159(2):967–979. doi:10.1210/en.2017-00748
- Assimakopoulos SF, Triantos C, Thomopoulos K, et al. Gut-origin sepsis in the critically ill patient: pathophysiology and treatment. Infection. 2018;46(6):751–760. doi:10.1007/s15010-018-1178-5
- Deng WS, Zhang J, Ju H, et al. Arpin contributes to bacterial translocation and development of severe acute pancreatitis. World J Gastroenterol. 2015;21:4293–4301. doi:10.3748/wjg.v21.i14.4293
- Guo Y, Huang C, Liu L, et al. Paneth Cell Ablation Aggravates Pancreatic and Intestinal Injuries in a Rat Model of Acute Necrotizing Pancreatitis after Normal and High-Fat Diet. Mediators Inflamm. 2019;2019:8474523. doi:10.1155/2019/8474523
- Su YR, Hong YP, Mei FC, et al. High-Fat Diet Aggravates the Intestinal Barrier Injury via TLR4-RIP3 Pathway in a Rat Model of Severe Acute Pancreatitis. Mediators Inflamm. 2019;2019:2512687. doi:10.1155/2019/2512687
- Huang Q, Wu Z, Chi C, et al. Angiopoietin-2 Is an Early Predictor for Acute Gastrointestinal Injury and Intestinal Barrier Dysfunction in Patients with Acute Pancreatitis. Dig Dis Sci. 2021;66(1):114–120. doi:10.1007/s10620-020-06138-0
- Xie RL, Chen WW, Qi MZ, et al. Trefoil factor-2, an early predictor for acute gastrointestinal injury in patients with acute pancreatitis. Medicine. 2021;100:e26624. doi:10.1097/MD.0000000000026624
- Van Laethem JL, Marchant A, Delvaux A, et al. Interleukin 10 prevents necrosis in murine experimental acute pancreatitis. Gastroenterology. 1995;108(6):1917–1922. doi:10.1016/0016-5085(95)90158-2
- Chiu CJ, McArdle AH, Brown R, Scott HJ, Gurd FN. Intestinal mucosal lesion in low-flow states. I. A morphological, hemodynamic, and metabolic reappraisal. Arch Surg. 1970;101:478–483. doi:10.1001/archsurg.1970.01340280030009
- Agarwala R, Rana SS, Sharma R, Kang M, Gorsi U, Gupta R. Gastrointestinal Failure Is a Predictor of Poor Outcome in Patients with Acute Pancreatitis. Dig Dis Sci. 2020;65(8):2419–2426. doi:10.1007/s10620-019-05952-5
- Derikx JP, Schellekens DH, Acosta S. Serological markers for human intestinal ischemia: a systematic review. Best Pract Res Clin Gastroenterol. 2017;31(1):69–74. doi:10.1016/j.bpg.2017.01.004
- Peoc’h K, Corcos O. Biomarkers for acute mesenteric ischemia diagnosis: state of the art and perspectives. Ann Biol Clin. 2019;77:415–421 doi:10.1684/abc.2019.1449.
- Fukuda T, Tsukano K, Nakatsuji H, Suzuki K. Plasma diamine oxidase activity decline with diarrhea severity in calves indicating systemic dysfunction related to intestinal mucosal damage. Res Vet Sci. 2019;126:127–130. doi:10.1016/j.rvsc.2019.08.027
- Yang JJ, Ma YL, Zhang P, Chen HQ, Liu ZH, Qin HL. Histidine decarboxylase is identified as a potential biomarker of intestinal mucosal injury in patients with acute intestinal obstruction. Mol Med. 2011;17(11–12):1323–1337. doi:10.2119/molmed.2011.00107
- Keck T, JHt B, Fernandez-del Castillo C, Antoniu BA, Warshaw AL. Matrix metalloproteinase-9 promotes neutrophil migration and alveolar capillary leakage in pancreatitis-associated lung injury in the rat. Gastroenterology. 2002;122:188–201. doi:10.1053/gast.2002.30348
- Muhs BE, Patel S, Yee H, Marcus S, Shamamian P. Inhibition of matrix metalloproteinases reduces local and distant organ injury following experimental acute pancreatitis. J Surg Res. 2003;109(2):110–117. doi:10.1016/S0022-4804(02)00084-7
- Deitch EA. Bacterial translocation or lymphatic drainage of toxic products from the gut: what is important in human beings? Surgery. 2002;131(3):241–244. doi:10.1067/msy.2002.116408
- McCall IC, Betanzos A, Weber DA, Nava P, Miller GW, Parkos CA. Effects of phenol on barrier function of a human intestinal epithelial cell line correlate with altered tight junction protein localization. Toxicol Appl Pharmacol. 2009;241(1):61–70. doi:10.1016/j.taap.2009.08.002
- Roxas JL, Koutsouris A, Bellmeyer A, et al. Enterohemorrhagic E. coli alters murine intestinal epithelial tight junction protein expression and barrier function in a Shiga toxin independent manner. Lab Invest. 2010;90(8):1152–1168. doi:10.1038/labinvest.2010.91
- Wang N, Yu H, Ma J, et al. Evidence for tight junction protein disruption in intestinal mucosa of malignant obstructive jaundice patients. Scand J Gastroenterol. 2010;45(2):191–199. doi:10.3109/00365520903406701