
Abstract
Background
A cross-sectional study was conducted to provide a snapshot of smoking behavior among staff and patients at a major metropolitan hospital in Melbourne.
Methods
Patients and staff were surveyed using a questionnaire exploring demographics, nicotine dependence (Fagerstrom test), readiness to quit, and preference for smoking cessation options.
Results
A total of 1496 people were screened within 2 hours; 1,301 participated (1,100 staff, 199 patients). Mean age was 42 years, 68% were female. There were 113 (9%) current smokers and 326 (25%) ex-smokers. Seven percent of the staff were current smokers compared with 19% of the patients. The Fagerstrom test showed that 47% of patients who smoked were moderately nicotine dependent compared with 21% of staff. A third of the staff who smoked did not anticipate health problems related to smoking. Most patients (79%) who smoked disagreed that their current health problems were related to smoking. Although more than half of the current smokers preferred pharmacotherapy, one in two of them did not prefer behavior counseling; with consistent results among staff and patients. Multivariate analyses showed that patients were three times more likely (odds ratio 3.0, 95% confidence interval 1.9–4.7) to smoke than staff.
Conclusion
This study reports lower prevalence of smoking among hospital staff compared with national data. It also indicates an under-appreciation of health effects of smoking, and a preference not to use conventional methods of quitting.
Introduction
Australia is considered to be a pioneer in tobacco control. A recent report from the Australian Bureau of Statistics (ABS) showed that the prevalence of smoking in Australia has decreased steadily over the past decade, from 22.4% in 2001 to 16.3% in 2011–2012.Citation1 Tobacco control initiatives primarily includes three categories: 1) increasing the price of tobacco products, mass media antismoking campaigns, smoke-free policies, including smoking curricula in schools, and changing social norms leading to restrictions on adolescents’ ability to purchase cigarettes; 2) addressing the tactics of the tobacco industry by restricting marketing opportunities; and 3) reducing harm from use of tobacco products.Citation2,Citation3 Australia is also the first country in the world to adopt plain-paper packaging for cigarettes, from December 1, 2012.Citation4 Plain packaging is one of the demand-reduction strategies mentioned in the World Health Organization (WHO) Framework Convention on Tobacco Control, the first evidence-based treaty for addressing the global tobacco epidemic.Citation5
It is commonly assumed, and often argued by the tobacco industry, that smokers are adequately informed about the health risks of smoking. The International Tobacco Control Four Country SurveyCitation6 in 2006, which included nationally representative samples of adult smokers from the United States, the United Kingdom, Canada, and Australia found that smokers showed significant gaps in their knowledge regarding the risks of smoking. Despite smokers being generally aware of the health risks of tobacco use, and most expressing a desire to quit, only a small percentage do so in any given year, and very few use formal cessation programs.Citation7 Many smokers need several cessation attempts before they can quit successfully. Therefore, it is important to explore the awareness and preferences for smoking cessation strategies among smokers.
There is a limited number of studies focusing on smoking behavior among patients and staff in Australian hospital settings. It is important to focus on this setting as smoking cessation interventions initiated during hospital stay are most effective.Citation8 Due to their vulnerable health and being in a setting where smoking is not allowed, there is a window of opportunity to intervene with hospitalized patients who smoke. On the other hand, smoking status of health care providers influences cessation counseling directed towards patients.Citation9 Therefore, it is also important to explore smoking behavior of the hospital staff, who can potentially support patients in the process of quitting. Literature suggests very low levels of routine provision of smoking cessation advice to patients by Australian health care providers.Citation10 On the other hand, smoking behavior and motivation to quit differ between patients and staff who are smokers.Citation11 Concerns about own health and health of family members or friends were identified as the key motivating factors to quit among both patients and staff who are smokers.Citation12 Patients were also reported to be more dependent on nicotine and less motivated to quit smoking compared with hospital staff.Citation11 Exploring readiness to quit and nicotine dependence among patients and staff is important for smoking cessation support strategies available in hospital settings in Australia to be implemented properly.
This study aimed to provide a snapshot of smoking behavior among patients and staff in a major metropolitan hospital in Melbourne, Australia in order to ascertain prevalence of smoking, levels of nicotine dependence, attitudes to the health impact of smoking, and attitudes to quit strategies. As the national data suggest that smoking prevalence differs by age and sex,Citation1 we also aimed to determine any association between current smoking and demographic variables.
Methods
Study design and study site
We performed a cross-sectional study to provide an overview of smoking behavior among patients and staff on a nominated day and time (WHO No Tobacco Day, May 31, 2012), within a 2-hour window (2–4 pm). The institution is a large tertiary public hospital with 848 beds, located in the Melbourne metropolitan area of Australia. As part of an increasing awareness strategy for a cardiovascular disease prevention week at that hospital, we conducted this study. The hospital provides inpatient and outpatient services as well as research and training for health staff. All inpatients and public outpatients, as well as staff on duty during the study period were asked to participate. Staff included clinicians with medical, nursing, and allied health backgrounds, pathology and administrative staff, and staff from environmental services.
Study population
There were no age exclusions applied to the study population. Visitors, patients in private outpatients or private rooms, intensive care, operating suites, and palliative care facilities were excluded. Those in the emergency department were also excluded as they had participated in a similar survey previously.
Sample size
The study was designed to include all consenting patients and staff within a specified period of 2 hours on a designated day at the hospital.
Study tool
A structured questionnaire, consisting of 25 close-ended questions was used. It required 5 minutes on average to complete. The questionnaire included sociodemographic details (ie, age, sex, country of birth, and employment status), smoking status (ie, current and ex-smokers, and age at smoking initiation), nicotine dependence using the Fagerstrom test for nicotine dependence (ie, no dependence, low dependence, low to moderate dependence, moderate dependence, and high dependence),Citation13 readiness to quit (quit attempts and intention to quit), perceptions on the relationship between smoking and their health, and participants’ preference for different smoking cessation options (ie, increasing price of cigarettes, face to face counseling, telephone counseling, group counseling, or counseling by local doctors). All of the variables in the study tool were categorical variables, except age of the participants, age at smoking initiation, and number of quit attempts. The questionnaire was adapted from a previous smoking audit conducted elsewhere.Citation14
Data collection
Participants were approached by the study team, and verbal consent was obtained. The interviewers then completed the questionnaire in hard copy. Interviewers were provided with an instruction sheet, which included information on how to approach the participants, how to introduce the study, as well as guidelines about completing the study. Eighty-four volunteers with a health care background collected data within the study period.
Data analysis
Data analyses were conducted using SPSS (IBM Corporation, Armonk, NY, USA) version 19 and Microsoft Excel® (Microsoft Corporation, Redmond, WA, USA). Categorical variables were described as proportions for sociodemographic details, smoking status, nicotine dependence, readiness to quit, participants’ perception of relationship between smoking and health, and participants’ preference for different smoking cessation options. Numerical variables were described in terms of mean and standard deviation (SD). To determine associations between smoking and different sociodemographic variables, smokers and nonsmokers were compared using cross-tabulations and by employing Pearson’s chi-squared (χ2) tests when the expected frequency in all of the cells of the cross-tabulation was ≥5, or Fisher’s exact test otherwise. Statistical significance was set at p<0.05. Univariate logistic regression models were fitted to determine the strength of association between smoking and demographic variables, and odds ratios (ORs) with 95% confidence intervals (CIs) were calculated. Then, multivariate logistic regression models were fitted to adjust for potential confounding variables. Confounding variables were identified initially using a χ2 test relating the sociodemographic variables to smoking. If the p-value from the χ2 test was less than 0.20 and there was no missing data for the confounder (excluding the cases with missing data, rather than the entire variable), that variable was included into the final multivariate analysis. The adjusted ORs with 95% CIs finally determined the association between smoking and demographic variables in this study.
Ethics statement
Verbal consent was obtained from each participant and only de-identified data were collected, thus ensuring privacy and confidentiality of the participants. The study was approved by the local Research Governance Unit.
Results
Study participants
A total of 1,496 patients and staff were screened. Of those, 1,301 (87%) agreed to participate. Nonparticipation was mainly due to their involvement in other activities during the study period. Among the total 1,301 participants, 1,100 (85%) were staff, 188 (15%) were inpatients, and 11 (1%) were outpatients. The study included 39% (1,100 out of 2,400) of staff, 49% (188 out of 384) of inpatients, and 11% (11 out of 105) of outpatients on the campus during the study.
Mean age of the participants was 42 (SD 17) years, with the majority being female (68%; 71% of staff and 53% of patients). More than one-third of the staff (38%) were from the 16–30 years age group, whereas the majority of the inpatients (60%) were above 60 years of age. Amongst 1,301 participants, 62% stated their country of birth as Australia and Oceania ().
Table 1 Sociodemographic profile and smoking status of participants in the cross-sectional study at a major metropolitan hospital in Melbourne, Australia
Smoking status
Of the 1,301 participants, 113 (9%) were current smokers and 326 (25%) were ex-smokers. Seven percent of staff were current smokers compared with 17% of inpatients and 55% of outpatients. Mean age at smoking initiation was 18 (SD 6) years. The vast majority of staff (87%) approved of a smoke-free hospital, and this policy was also endorsed by 69% of inpatients (). Nonsmokers were far more likely than current smokers (95% versus 5%) to support the smoke-free environment.
Nicotine dependence
Responses on the Fagerstrom test for nicotine dependenceCitation13 are shown in . Patients tended to be more nicotine dependent than staff, with almost half of the patients (47%) classified as moderately nicotine dependent compared with a fifth (21%) of staff. Furthermore, 18% of patients were classified as highly nicotine dependent compared with only 1% of staff (). Univariate analyses also showed that patients (OR 16.48, 95% CI 1.95–140) and respondents over 30 years of age were more likely to be highly nicotine dependent (data not shown).
Figure 1 Comparing scores from Fagerstrom test for nicotine dependence between staff and patients in the cross-sectional study at a major metropolitan hospital in Melbourne, Aaustralia.
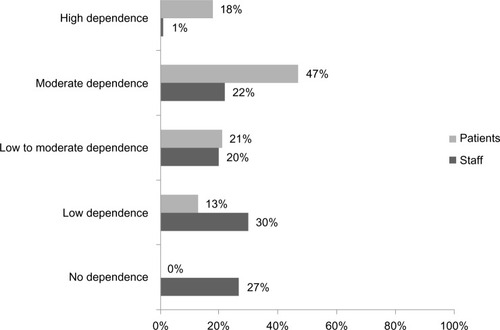
Table 2 Smoking behavior of current smokers in the cross-sectional study at a major metropolitan hospital in Melbourne, Australia
Attitudes to the health impact of smoking
A third (32%) of staff who smoked did not anticipate health problems related to smoking, compared with almost half of the patients (42%). Four out of five patients (79%) who smoked did not feel that there was a relationship between smoking and their current health problems; and one in four (24%) did not agree that smoking cessation would improve their health. This view was also held by 8% of staff.
Attitudes to quit strategy
Two-thirds of the smokers in this study expressed a desire and intention to quit within the next 6 months (67% of staff and 61% of patients). Although more than half of the current smokers intended to try pharmacotherapy (nicotine replacement therapy or non-nicotine medication) for smoking cessation, 48% of staff and 55% of patients stated that they did not prefer to use face to face counseling, telephone counseling, group counseling, or counseling by local doctors in order to quit smoking. The majority of the staff (85%) and patients (82%) did not believe that raising the cost of cigarettes to $20/pack would increase the likelihood of quitting ().
Association between smoking and demographic variables
shows the univariate and multivariate analyses exploring the association between current smoking and different demographic variables. Univariate analyses showed that participants of 16–30 years, females, and patients were more likely to smoke in this study. When the potential confounding variables such as age, sex, type of participants (ie, patients or staff), and country of birth were adjusted during multivariate analyses, it showed that patients were three times more likely (adjusted OR 3.0, 95% CI 1.9–4.7) to smoke compared with other participants.
Table 3 Association between current smoking and different demographic variables in the cross-sectional study at a major metropolitan hospital in Melbourne, Australia
Discussion
This study captured a snapshot of smoking behaviors and attitudes among patients and staff at a metropolitan hospital in Melbourne, Australia. The prevalence of smoking among hospital staff (7%) was lower than the Australian national smoking prevalence (16%).Citation1 We also recognize that current smokers may have been less likely to participate in the study, thus leading to an underestimation of the number of smokers. This finding is consistent with a recent survey of metropolitan hospitals in South Australia, which also reported a lower than average prevalence of smoking amongst its staff (8%).Citation15 The study also reported a steady decline in staff smoking rates in that particular hospital over the past decade.Citation15
Awareness regarding the potential effects of smoking on health was poor among both patients and staff. Individual smoking behavior of hospital staff can strongly influence their knowledge of the health consequences of smoking; smokers systematically underestimated the health consequences of smoking compared with ex- and never-smokers, which was independent of profession, department, sex, and age.Citation16 This is important because low levels of awareness and/or lack of knowledge amongst staff may result in incorrect or no advice being provided to patients regarding the health consequences of smoking.Citation16 A Cochrane review suggested that nursing interventions can increase quitting rates when compared with usual care.Citation17 Furthermore, evidence indicates that when smoking cessation interventions conducted by nurses are focused on cardiovascular disease patients, this can lead to a significant reduction in smoking rates, systolic blood pressure, diastolic blood pressure, and lipid levels.Citation18 Therefore, it is critical not only to target patients directly with information about the health consequences of smoking and the importance of smoking cessation, but also to address gaps in knowledge amongst health professionals, with a particular emphasis on those who smoke.
We found that younger people (16–30 years) and females were more likely to smoke in this hospital-based study, which again differs from Australian statistics.Citation1 The 2011–2012 national data show that males are more likely to smoke than females, the majority (89%) of people aged 15–17 years have never smoked, and smoking rates among young people (18–24 years) are also in decline.Citation1 However, US data suggest that younger patients (less than 50 years) are more likely to smoke during their hospital stay.Citation19 The increased prevalence of smoking among younger people and females in this study may be due to more participation from these groups during the survey. Future studies including a similar proportion of males and females would clarify possible sex differences for smoking behavior. Our study showed that the smoking initiation age was below 21 years for almost all of the smokers. This is consistent with the recent report from the US Surgeon General, which reports that in the vast majority of cases (88%), first use of cigarettes occurs by 18 years of age, with 99% of first use by 26 years of age.Citation20 This finding indicates the importance of focusing on smoking intervention at an early age.
We also found that patients were more likely than staff to be smokers and moderate to highly nicotine dependent; this is compatible with findings from similar studies.Citation21 The two-pronged approach of specialist behavioral support, as well as pharmacological treatment where indicated, is considered the gold standard for smoking cessation.Citation22 In light of this, the fact that although smokers preferred to use pharmacotherapy for smoking cessation in this study, their preference of not using behavior counseling is of concern. It was beyond the scope of this study to investigate the reasons for their reluctance to use behavior counseling. Literature suggests that patients reported less confidence in doctors and perceived that they had confidence in their own ability to quit smoking without medical advice.Citation12 But health care providers have a strong influence on patients, therefore, it is important to focus on the communication gap between them and patients. In addition, having social support may be another important factor to consider for smokers to quit. Although the social support alone for smoking cessation, which includes emotional, informational, and instrumental support, has not been shown as an effective intervention for smoking cessation,Citation23 combining social support with behavioral counseling may be their preferred choice and an effective intervention to assist them in quitting. It is crucial to identify preferences for smoking cessation options among both hospital patients and staff in future studies.
This study reported that two-thirds of smokers were ready to quit within the next 6 months, which is the important first step of motivation to quit smoking. Literature suggests that when readiness to quit is increased, interventions need to target on reducing cravings.Citation11 Increased awareness campaigns in the hospital may aid in improving the readiness to quit among smokers. Moreover, the hospital system can utilize this opportunity and follow the successful example from New Zealand, where hospitalized smoker patients are supported for smoking cessation using the ABC approach (Ask for smoking behavior and document responses, Brief advice to stop smoking regardless of their desire or motivation to quit, offering or referring to evidence-based Cessation treatment).Citation24 The patients can be offered pharmacological treatment during their stay in the hospital and can be linked to general practitioners or Quitline for further assistance. The policy for smoking cessation support of this study hospital also mentions this approach, but it warrants further investigation regarding implementation of the policy.
A smoke-free policy in the hospital was more supported by hospital staff than by patients, but was generally unpopular with current smokers. Research suggests that the visibility of smoking in a hospital campus is disapproved of by hospital staff, and a complete ban or provision of discrete smoking areas are potential solutions.Citation15 In line with the smoke-free policy in public places in Victoria, the study hospital has been declared smoke free since July 2009, and smoking is not allowed in buildings, vehicles, or in outdoor areas within the boundary of the hospital premises. However, further studies investigating the status of smoke-free areas and monitoring hospital smokers will guide to implement the current smoke-free policy effectively.
This study has certain limitations. Due to the cross-sectional design of the study and restricting 2-hour timeframe for collecting data, it is possible that many eligible patients and staff were not included. In addition, sampling of participants was not randomized, and the study did not cover a representative sample of patients and staff of the study hospital, which limit generalizability of the study findings to other study settings and should be interpreted with caution. Staff were not categorized further according to specific occupation (eg, doctor, nurse) limiting further analyses according to professional group. Similarly, patients were not categorized according to a specific department, which also limited our ability to analyze the findings according to patient groups. Another limitation was that the study relied on self-reporting of smoking status. Adding a screening test would have provided corroborative results, but was beyond the scope of this study.
Nevertheless, the data on the prevalence of smoking and smoking behavior will be an important baseline for this major metropolitan hospital and will be used to compare with future studies. The findings also underline the importance of continued education on smoking cessation, as this can increase smoking cessation interventions in the hospitals.Citation25 The study reported here was part of awareness-raising activities conducted during the WHO World No Tobacco Day. We recommend that awareness-raising campaigns, education, and associated smoking cessation services continue throughout the year, with the aim of decreasing smoking among hospital patients and staff.
Author contributions
MAR did the data analyses and prepared the manuscript. AMW, RS, DC, DRT, CFS, SM, and LWC participated in conceptualization and design of the study. RS, KD, and CW collected data and contributed to analyses. All authors read and approved the final manuscript.
Acknowledgments
The smoking audit was organized by a multidisciplinary clinical research group of the study hospital. We appreciate the support from the volunteers for conducting this audit. The audit questionnaire was adapted from one used for another smoking audit elsewhere. We would like to thank Professor Jenny Peat for her advice on statistical analyses in this manuscript. We would also like to thank Samantha McEvedy for her assistance in editing for English language.
Disclosure
The smoking audit was funded in part by Pfizer Australia Pty Ltd. The authors report no other conflicts of interest in this work.
References
- Australian Bureau of Statistics [homepage on the Internet]4364.0.55.001 – Australian Health Survey: First Results, 2011–12Health risk factors: tobacco smokingAustralian Bureau of Statistics2012 [cited November 13, 2012]. Available from: http://www.abs.gov.au/ausstats/[email protected]/Lookup/73963BA1EA6D6221CA257AA3001BE3E?opendocumentAccessed November 25, 2013
- PierceJPWhiteVMEmerySLWhat public health strategies are needed to reduce smoking initiation?Tob Control2012212258264
- WestRTobacco control: present and futureBr Med Bull20067778123136
- Framework Convention Alliance [homepage on the Internet]Australia defeats Big Tobacco’s challenge!GenevaFramework Convention Alliance2012 [cited November 14, 2012]; Available from: http://fctc.org/index.php?option=com_content&view=article&id=797%3Aaustralia-defeats-big-tobaccos-challenge&catid=239%3Apackaging-and-labelling&Itemid=243Accessed November 25, 2013
- World Health OrganizationWHO Framework Convention on Tobacco ControlGeneva, SwitzerlandWorld Health Organization2003
- HammondDFongGTMcNeillAEffectiveness of cigarette warning labels in informing smokers about the risks of smoking: findings from the International Tobacco Control (ITC) Four Country SurveyTob Control200615Suppl 3iii19iii25
- HennrikusDJJefferyRWLandoHAThe SUCCESS project: the effect of program format and incentives on participation and cessation in worksite smoking cessation programsAm J Public Health200292227427911818305
- RigottiNAClairCMunafoMRInterventions for smoking cessation in hospitalised patientsCochrane Database Syst Rev20125CD00183722592676
- MeshefedjianGAGervaisATremblayMPhysician smoking status may influence cessation counseling practicesCan J Public Health2010101429029321033533
- CastaldoJNesterJWasserTPhysician attitudes regarding cardiovascular risk reduction: the gaps between clinical importance, knowledge, and effectivenessDis Manag20058293105
- DickensGLStanifordJLongCGSmoking behaviour, motives, motivation to quit and self-efficacy among patients in a secure mental health service: comparison with staff controlsJ Psychiatr Ment Health Nurs Epub5312013
- JoshiVSuchinVLimJSmoking cessation: barriers, motivators and the role of physicians – a survey of physicians and patientsProc Singap Healthc2010192145153
- HeathertonTFKozlowskiLTFreckerRCThe Fagerstrom Test for Nicotine Dependence: a revision of the Fagerstrom Tolerance QuestionnaireBr J Addict199186911191127
- VargasRWeilandTJTaylorDPrevalence of smoking among adult emergency department patients: a multisite Australian studySt Vincent’s Hospital Melbourne Research WeekMelbourne, Australia. MelbourneSt Vincent’s Hospital Melbourne2011
- JonesTEWilliamsJSmoking prevalence and perspectives on smoking on campus by employees in Australian teaching hospitalsIntern Med J2012423311316
- WillaingIJorgensenTIversenLHow does individual smoking behaviour among hospital staff influence their knowledge of the health consequences of smoking?Scand J Public Health200331214915512745766
- RiceVHSteadLFNursing interventions for smoking cessationCochrane Database Syst Rev20081CD00118818253987
- McPhersonCPSwensonKKPineDAA nurse-based pilot program to reduce cardiovascular risk factors in a primary care settingAm J Manag Care20028654355512068961
- ReganSVianaJCReyenMPrevalence and predictors of smoking by inpatients during a hospital stayArch Intern Med20121721670167423128676
- US Department of Health and Human ServicesPreventing tobacco use among youth and young adults: a report of the Surgeon GeneralAtlanta, GADepartment of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health2012
- SchulzMTopperMBehrensJ[Smoking habits of employees and patients in the psychiatric department of a general hospital]Gesundheitswesen2004662107113 German14994209
- DuasoMDuncanDHealth impact of smoking and smoking cessation strategies: current evidenceBr J Community Nurs201217835636322875209
- WestmaasJLBontemps-JonesJBauerJESocial support in smoking cessation: reconciling theory and evidenceNicotine Tob Res20101269570720513695
- Ministry of Health Targeting Smokers: Better Help for Smokers to QuitWellingtonMinistry of Health2011
- StephenVIwonaSSmoking cessation education increases interventions in a New Zealand hospital: World No Tobacco Day revisitedN Z Med J201012313173540