
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Objective
Breast cancer is the most common malignancy and one of the main causes of death in women. Luminal B (HER2−) breast cancer subtype has been proposed since the 2011 St Gallon consensus. The hormone receptor status in this type of breast cancer is positive; thus, endocrine therapy was performed in all cases, but the treatment was not satisfactory, and a significant number of cases received very little benefit from chemotherapy. Furthermore, there is no effective treatment target for this subtype. Luminal B (HER2−) breast cancer subtype has been proposed since the 2011 St Gallon consensus. Therefore, the study of the key molecules in the microenvironment of breast cancer can help to reveal the biological characteristics.
Patients and methods
Luminal B (HER2−) breast cancer is a subtype with higher heterogeneity and poorer prognosis than luminal A. It is known that the development of cancer cells is an active process, and this process needs microenvironment cytokines, including chemokine (C–C motif) ligand 5 (CCL5) and collagen IV. Therefore, CCL5 and collagen IV were imaged and detected by quantum dot, and the CCL5/collagen IV ratio was calculated to investigate the prognostic value of the CCL5/collagen IV ratio in luminal B (HER2−).
Results
Quantitative determination showed a statistically significant negative correlation between CCL5 and collagen IV. The 5-year disease-free survival (5-DFS) of the high and low CCL5/collagen IV ratio subgroups was significantly different. The CCL5/collagen IV ratio had a greater prognostic value for 5-DFS. The CCL5/collagen IV ratio was an independent prognostic indicator.
Conclusion
Our findings revealed the effective integration of tumor CCL5 and collagen IV, and a new method for predicting the prognosis of luminal B (HER2−) has been developed.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Introduction
Breast cancer is the most common malignancy and one of the main causes of death in women.Citation1 Luminal B (HER2−) subtype breast cancer is defined as (estrogen receptor [ER]+), (progestogen receptor [PR]+; <20%), HER2− and Ki-67≥14% disease.Citation2 According to the St Gallen 2015 definitions, the proportion of luminal (HER2−) cancer is 71% and luminal B-like (HER2+) is 6%,Citation3 and race/ethnicity and socioeconomic status are independent in contributing to disease among luminal A tumors, but not found in women with luminal B (HR+/HER2+) disease.Citation4 The clinicopathological features of luminal B breast cancer are similar to those of luminal A breast cancer, but luminal B cancer has a higher heterogeneity and poorer prognosis than luminal A,Citation5,Citation6 and there is a higher proportion of local recurrence and single bone metastasis in patients with luminal B breast cancer than in patients in the nonluminal groups.Citation7 The hormone receptor status in this type of breast cancer is positive; thus, endocrine therapy was performed in all cases, but the treatment was not satisfactory,Citation8 and a significant number of cases received very little benefit from chemotherapy. Furthermore, there is no effective treatment target for this subtype. Luminal B (HER2−) breast cancer subtype has been proposed since the 2011 St Gallon consensus. This subtype of breast cancer has been extensively studied.Citation9–Citation16 It is known that the microenvironment is closely related to the occurrence and development of tumor.Citation17,Citation18 Therefore, the study of the key molecules in the microenvironment of breast cancer can help to reveal the biological characteristics. Imaging technology of nanoparticle quantum dot (QD)-labeled molecular probes is a new technology that is based on nanomaterials and immunofluorescence detection. It has characteristics such as good histocompatibility, fluorescence signal stabilization and multimolecule coaxial imaging. We have already applied this technology to study some key molecules in breast cancer such as HER2, ER, EGFR and Ki-67Citation19–Citation22 and some key molecules in microenvironment such as collagen IV,Citation23 and the co-imaging of the key molecules between cancer cells and the tumor microenvironment (TM) was also successfully performed.Citation24 But how the key molecules participate in the occurrence and development of tumor through the microenvironment needs further study.
CCL5 is one of the key breast cancer molecules which is closely related to invasion and metastasis of breast cancer.Citation25,Citation26 Exploring the dynamic relationship between CCL5 and breast cancer microenvironment would help to reveal the mechanism of tumor invasion and metastasis. Invasion and metastasis of breast cancer are a multistep complex process, which include laminine bound to extracellular matrix (ECM), released protein hydrolase, degraded ECM, passed through basement membrane (BM) transfer and so on. ECM is the main tissue barrier of tumor cell infiltration, mainly composed of collagen IV and others, which can prevent the invasion and metastasis of tumor cells. Exploring the dynamic relationship between CCL5 and breast cancer microenvironment is helpful to reveal the process of tumor invasion and metastasis.
Traditional immunohistochemical (IHC) technique can only perform semiquantitative detection of a single tumor key molecule; however, the imaging technique of nano-QD-labeled molecular probes can realize multimolecule coaxial imaging.Citation19 Some scholars have applied this technology to study the key molecules of breast cancer.Citation19,Citation27,Citation28 We have successfully applied this technique in the previous study.Citation20–Citation24,Citation29,Citation30 Based on earlier studies, we used luminal B (HER2−) breast cancer as the study sample, performing molecular co-imaging of CCL5 and collagen IV, to investigate the mechanism of invasion and metastasis of luminal B (HER2−) breast cancer. Meanwhile, we further constructed the quantitative evaluation system of CCL5 and collagen IV by image acquisition system to find out new prognostic markers for luminal B (HER2−) breast cancer.
Patients and methods
Patients and specimens
Formalin-fixed, paraffin-embedded specimens from 109 patients with luminal B HER2− invasive breast cancer were collected from the Second People’s Hospital of Wuhu, China, from January 2009 to January 2012. All patients are women, aged from 24 to 79 years, with a median age of 49 years. There were 44 cases with lymph node metastases and 65 without lymph node metastases. Major pathological parameters, including age, tumor size, lymph node status and histological grade as determined by conventional IHC, were available. All patients had undergone six to eight cycles of anthracycline- and docetaxel-based chemotherapy after breast cancer surgery; patients who had >3 metastatic lymph nodes had undergone radiotherapy after chemotherapy; and all patients had undergone endocrinotherapy after chemotherapy (tamoxifen was used pre menopause, and letrozole was used after menopause). The end point of the follow-up study was recurrence or distant metastasis. The study protocol was approved by the medical ethics committee of the Second People’s Hospital of Wuhu. All the patients whose tissue samples were used had provided written informed consent. The characteristics of patients are summarized in .
Table 1 Correlation between CCL5/collagen IV ratio and clinicopathological features of breast cancer
CCL5 testing
Four-micrometer-thickness tissue sections were heated for 1.5 h at 60°C and then dewaxed three times in xylene solution (each time for 6 min). Tissue sections of dewaxing were hydrated by alcohol of descending concentration (100% ethanol→95% ethanol→85% ethanol→75% ethanol→H2O→ddH2O). Tissue sections of hydration were pretreated in citric acid buffer for antigen retrieval (0.01 M/L, pH 6.0; 100°C citric acid buffer→H2O→ddH2O→Tris-buffered saline). Tissue sections of antigen retrieval were added to the blocking buffer (3% H2O2), then incubated at 37°C for 10 min and, finally, rinsed three times by Tris-buffered saline (every time for 3 min). After removing the blocking buffer, slides were added to mouse antihuman CCL5 (1:100; 53405.111; Abcam, Cambridge, UK) and then incubated at 37°C for 2 h. The slides were rinsed with mixed solution of Tris-buffered saline and Tween-20 (2,000:1) and then added to the blocking buffer after removing the rinsed solution, followed by incubating at 37°C for 30 min. The slides were added to biotin-labeled sheep anti-rabbit immunoglobulin G (IgG) (dilution 1/100; Vector Laboratories, Inc., Burlingame, CA, USA) after removing the blocking buffer and then incubated at 37°C for 1 h. The slides were added to quantum dots conjugated streptavidin (QDs-SA) probe (λ=605 nm; Jiayuan Quantum Dots, Wuhan, China) after blocking and then incubated at 37°C for 30 min. The slides were sealed by mixed solution of Tris-buffered saline, and there was no fluorescence glycerol (1:9) after rinsing; the slides were then observed using fluorescence microscope (Leica DM 4000B; Leica Microsystems, Wetzlar, Germany) in Blu-ray (λ=405–565 nm), finally, stored at 4°C by avoiding light.
CCL5 and collagen IV testing
The main steps for the imaging of CCL5 and collagen IV are as follows: heating (60°C, 1.5 h)→dewaxing (xylene solution)→hydration (alcohol-gradient hydration)→antigen retrieval (citric acid buffer pretreatment)→blocking (Tris-buffered saline)→adding the first antibody (mouse antihuman CCL5; rabbit antihuman collagen IV, 1:200, EPR17072; Abcam)→rinsing (mixed solution of Tris-buffered saline and Tween-20, 200:1)→blocking (Tris-buffered saline)→adding the second antibody (biotinylated IgG)→rinsing (mixed solution of Tris-buffered saline and Tween-20, 200:1)→blocking (Tris-buffered saline)→adding QDs-SA (605-QDs-SA, 525-QDs-SA)→rinsing (mixed solution of Tris-buffered saline and Tween-20, 200:1)→sealing (mixed solution of Tris-buffered saline and no fluorescence glycerol, 1:9)→observation (the fluorescence microscope, λ=330–385 nm). In addition to the three experimental steps, such as adding the first antibody, adding QDs-SA and observation, the other steps were the same as the CCL5 experiment. In the process of adding the first antibody, mouse antihuman CCL5 (1:100) and rabbit antihuman collagen IV (1:200) were blending (1:1). In the process of adding QDs-SA, 605-QDs-SA and 525-QDs-SA were blending (1:1). The experimental results were observed by fluorescence microscope under ultraviolet (UV) excitation: 605-QDs-SA (inorganic components: ZnCdSe/ZnS; surface ligands: oleic acid; size: 7.5±0.5 nm; emission: 604 nm; full width at half maximum: 29 nm; quantum yield: 92%; MaiXin-Bio, Fuzhou, China) and 525-QDs-SA (inorganic components: ZnCdSe/ZnS; surface ligands: oleic acid; size: 5.5±0.5 nm; emission: 521 nm; full width at half maximum: 34 nm; quantum yield: 75%; MaiXin-Bio; ).
Figure 1 CCL5 and collagen IV testing.
Notes: CCL5 expressed in the cytoplasm of cancer cell and collagen IV expressed in the BM were imaged and detected simultaneously and quantitatively by QD-based system. a, heating, dewaxing, hydration; b, antigen retrieval, blocking, adding the first antibody; c, rinsing, blocking, adding the second antibody; d, rinsing, blocking, adding QDs-SA; e, rinsing, sealing, observation.
Abbreviations: BM, basement membrane; CCL5, chemokine (C–C motif) ligand 5; QD, quantum dot.
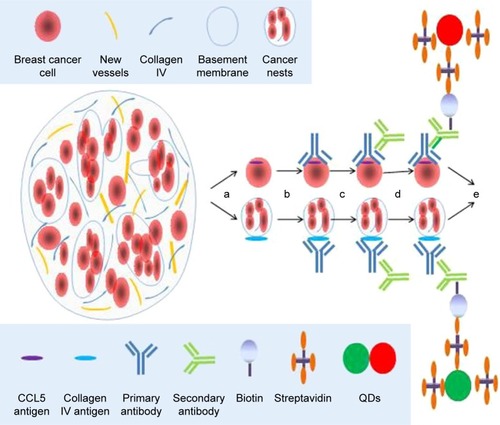
Image acquisition and analysis
The molecular imaging of QDs was acquired by Olympus DP72 image acquisition system (Olympus Corporation, Tokyo, Japan). The QD fluorescence signal information on CCL5 and collagen IV was analyzed as mentioned earlier. The distribution and expression intensity of QDs were quantified by spectral stripping technique, and the QD score (QDS) of each sample was obtained.
Statistical analyses
The relationship between the CCL5/collagen IV ratio and clinical characteristics was assessed by the Mann–Whitney U test or the Kruskal–Wallis H test, and Spearman correlation analysis was adopted. The optimal boundary value point was defined by the curve analysis of the subject (receiver operating characteristic curve [ROC]). The single-factor survival analysis was carried out by Kaplan–Meier method. The log-rank examination and evaluation group was used to evaluate the difference. Cox proportional risk model was used to evaluate the independent prognostic factors of breast cancer. Statistical analyses were performed by SPSS 19.0 software (IBM Corporation, Armonk, NY, USA), and two-tailed P<0.05 was considered as statistically significant.
Results
CCL5 and collagen IV detection and quantification in luminal B (HER2−) tissue
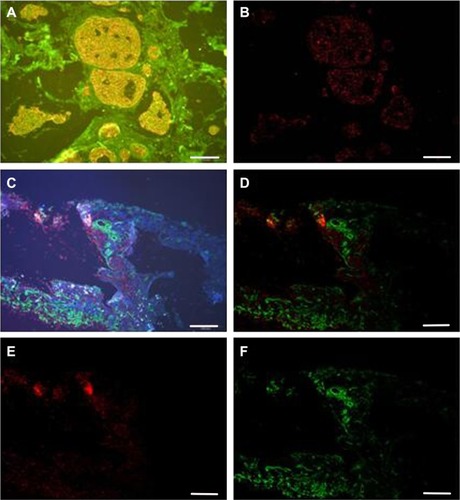
We found that CCL5 fluorescence of orange red QDs with specific distribution in the cytoplasm of cancer cell () using QD-F(ab)2 probes excited by a single UV excitation light source (UV 330–385 nm), software separation of CCL5 QD fluorescence (), CCL5 and collagen IV co-imaging, CCL5 fluorescence imaging is orange red in the cytoplasm, collagen IV fluorescence imaging is green in the BM (), software separation of CCL5 and collagen IV QD fluorescence (), spectrally isolated CCL5 single expression signals (), spectrally isolated collagen IV single expression signals (). In 109 patients, there was statistically significant negative association between CCL5 and collagen IV (Spearman’s ρ, P=0.001, r=−0.315).
Figure 2 CCL5 and collagen IV detection and quantification in luminal B (HER2−) tissue.
Notes: (A) CCL5 fluorescence of orange red QDs with specific distribution in the cytoplasm of cancer cell. (B) Software separation of CCL5 QD fluorescence. (C) CCL5 (red) on the cytoplasm of cancer cell and collagen IV (green) in the ECM were visible at high resolution against the clear discernable background. (D) Software separation of CCL5 and collagen IV QD fluorescence. (E) Spectrally isolated CCL5 single expression signals. (F) Spectrally isolated collagen IV single expression signals. Scale bar=100 μm.
Abbreviations: CCL5, chemokine (C–C motif) ligand 5; ECM, extracellular matrix; QD, quantum dot.
Relationship between CCL5/collagen IV ratio and clinicopathological traits
The relationship between CCL5/collagen IV ratio and clinicopathological traits, including age, tumor size, lymph node status and tumor grade, was evaluated. The CCL5/collagen IV ratio was significantly correlated with tumor size and lymph node status. There was no significant correlation with age and tumor grade ().
CCL5 and CCL5/collagen IV ratio expression according to 5-year disease-free survival (5-DFS)
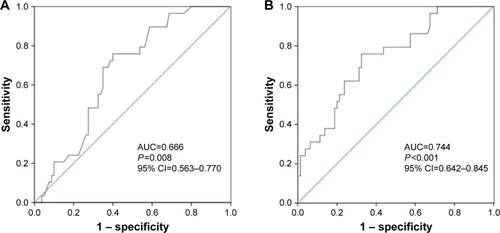
ROC analysis of the CCL5 and CCL5/collagen IV ratio expression according to 5-DFS indicated that they could predict 5-DFS (). According to the optimal sensitivity and specificity of the ROC curve that was based on the 5-DFS status, we chose 54.5 and 0.79 as the cutoffs for the CCL5 and CCL5/collagen IV ratio expression, respectively, where the CCL5 expression had 75.9% sensitivity and 60.0% () specificity and the CCL5/collagen IV ratio had 75.9% sensitivity and 67.5% specificity (). The CCL5/collagen IV ratio had higher specificity and a larger area under the curve than CCL5 expression, suggesting that the ratio has better prognostic value for 5-DFS than CCL5 expression.
Figure 3 ROC analysis of the CCL5 and CCL5/collagen IV ratio expression according to 5-DFS.
Notes: (A) CCL5 ROC (sensitivity=0.759, specificity=0.60, P=0.008, cutoff=54.5, AUC=0.666, 95% CI=0.563–0.770). (B) CCL5/collagen IV ratio ROC (sensitivity=0.759, specificity=0.675, P<0.001, cutoff=0.79, AUC=0.744, 95% CI=0.642–0.845).
Abbreviations: AUC, area under the curve; CCL5, chemokine (C–C motif) ligand 5; 5-DFS, 5-year disease-free survival; ROC, receiver operating characteristic.
CCL5 and CCL5/collagen IV ratio expression and 5-DFS
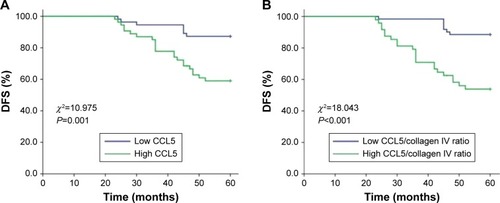
In this study, the 5-DFS rate was 73.4% (80/109) with 19 local recurrences and 10 distant recurrences. We classified the patients as high and low CCL5 expression subgroups that were based on the CCL5 expression cutoff value of 54.5. The 5-DFS rate was 87.3% for the patients who had low CCL5 (n=55) and 59.3% for the patients who had high CCL5 (n=54), the difference was significant (P=0.001, log-rank test; ). Based on the CCL5/collagen IV ratio cutoff value of 0.79, the 109 patients were classified as the high and low CCL5/collagen IV ratio subgroups. The 5-DFS rate was 88.5% for the patients who had low CCL5/collagen IV ratio (n=61), and 54.2% for the patients who had high CCL5/collagen IV ratio (n=48). The 5-DFS of these two groups was significantly different (P<0.001, log-rank test; ).
Figure 4 CCL5 and CCL5/collagen IV ratio and 5-DFS.
Notes: (A) CCL5 and 5-DFS, the cutoff value was 54.5; the 5-DFS of these two groups was significantly different (P=0.001, log-rank test). (B) CCL5/collagen IV ratios and 5-DFS, the cutoff value was 0.79; the 5-DFS of these two groups was significantly different (P<0.001, log-rank test).
Abbreviations: CCL5, chemokine (C–C motif) ligand 5; 5-DFS, 5-year disease-free survival.
Multivariable analyses revealed that the CCL5/collagen IV ratio (cutoff 0.79) was predictive in breast cancer and was an independent prognostic indicator ().
Table 2 Multivariate analysis of 5-DFS in 109 patients with breast cancer
Discussion
It is known that the TM, serving pivotal role in tumor development, is an important factor in identifying recurrence and promoting metastasis.Citation17,Citation31,Citation32 Chemokines can regulate the TM-driven mammary carcinomas.Citation33 CCL5 is a novel therapeutic target for estrogen-dependent breast cancerCitation34 and is essential for tamoxifen resistance in human breast cancer cells.Citation35 B subtype breast cancer is a relatively poor prognosis for Luminal A subtype breast cancer, especially luminal B (HER2−) has no effective therapeutic target. This study focused on luminal B (HER2−) and CCL5 to explore possible therapeutic targets for this type of breast cancer. The existing CCL5 detection method of breast cancer is mainly semiquantitative IHC,Citation36 but we have successfully visualized and quantitatively detected CCL5 by using QD technology. Subsequently, the follow-up results showed that the prognosis of high CCL5 expression group was significantly worse than that of low expression group, indicating that high CCL5 expression is related to tumor infiltration and metastasis and poor prognosis; it was consistent with many studies in recent years.Citation37,Citation38 Collagen IV is an important component of ECM in TM. Therefore, we focused on CCL5 and collagen IV at the same time. QD technology is applied to implement the CCL5 and collagen IV co-imaging; this makes it possible to monitor two indicators of the same samples of breast cancer microenvironment at the same time to become a reality, so that we can observe the dynamic changes between the two indicators. In the study of luminal B (HER2−) breast cancer, we found that there was statistically significant negative association between CCL5 and collagen IV. A number of studies have confirmed that CCL5 is closely related to tumor infiltration and metastasis,Citation39–Citation42 whereas this study further suggests that CCL5 promotes metastasis associated with collagen IV.
The accurate classification of tumor is the premise of individualized treatment of tumor. In recent years, the further classification of luminal breast cancer has attracted much attention. HR+/HER2− tumors were divided into two groups, which were based on the difference between luminal A/B signature (protein expression of ER, AR, Bcl-2, Bim [BCL2L11], GATA3 and INPP4b).Citation43 Luminal B breast tumor is more common, but this type has not been investigated thoroughly, because it has aggressive clinical and biological features and constitutes the most heterogeneous molecular subtype, both clinically and molecularly. The luminal B group can be divided into subtypes according to the expression of Ki-67 (cutoff at 25%).Citation44 Unfortunately, the classification of luminal B subtype breast cancer remains still imprecise by immunohistochemistry, but it is important to define a classification scheme capable of segregating luminal tumors into clinically meaningful subgroups that may be used clinically to guide patient management.Citation6 According to the St Gallen 2015 guidelines, the proportion of BCs classified as luminal B (HER2−) is highly influenced by the Ki67-LI assessment method. But there is no standardized assessment method.Citation3 APOA1, GELS, HS90B, EF1A1, NHRF1 and PRDX3 can identify the type of luminal B breast cancer.Citation45 Attentions are focused on the tumor biomarkers, but the growth of tumor requires microenvironment.Citation46–Citation49 In this study on the basis of synchronous detection of CCL5 and collagen IV, to evaluate further the prognostic value of CCL5/collagen IV ratio, we found that the prognosis of the high CCL5/collagen IV ratio group was significantly worse than the low CCL5/collagen IV ratio group, and the CCL5/collagen IV ratio prediction value was superior to the predicted value of CCL5. Multivariable analyses revealed that the CCL5/collagen IV ratio was an independent predictor. Therefore, it offered more options at the time of treatment; we need to pay attention on the tumor itself and the microenvironment of the tumor as well. Although we explored a new belief for the treatment of patients with luminal B (HER2−) breast cancer, we need to combine more information than study the relationship between them to identify different subtypes through QD-based in situ simultaneous imaging and quantitative analysis to guide individualized and effective treatment.
We used QD-based imaging and computer-aided quantitative analysis to image and quantitatively analyze the key molecules CCL5 and collagen IV successfully in luminal B (HER2−). Our findings demonstrated the QD-based multiplex multispectral technique can be highly sensitive, colocated molecular imaging and quantitative analysis. This technique may help us to assess multiple breast tumor markers and key molecules in microenvironment in specimens with limited available tissue and to observe qualitative and quantitative relationship between tumor cells and microenvironment dynamically and, finally, to explore the subtypes of breast cancer with different prognosis and biological characteristics. Thus, the QD-based in situ simultaneous imaging and quantitative analysis will be widely used in clinical and scientific research.
This study has some limitations. First, it was a retrospective study using a nonrandomized database, and it included only 109 breast cancer specimens, so this study needs to be validated in a large sample and prospective clinical trial. Second, the follow-up was only 5 years, so we need longer follow-up. Third, some slides were too old for QD-based in situ simultaneous imaging and quantitative detection to be performed accurately and were abandoned, so the amount of specimens was small. Fourth, collagen IV is not tumor-specific, it is a major extracellular matrix constituent, so we did not analyze its prognostic value. Nevertheless, QD-based nanotechnology provides a new method to detect multiple biomarkers. This study achieved in situ, highly sensitive, colocated molecular imaging and quantitative detection of CCL5 and collagen IV and demonstrated the prognostic value of the CCL5/collagen IV ratio in patients with luminal B (HER2−) breast cancer who received equivalent individualized treatment.
Conclusion
We capitalized on QD-based multiplex molecular imaging and computer-aided quantitative analysis technology to simultaneously and quantitatively detect CCL5 and collagen IV expression. The new indicator, CCL5/collagen IV ratio, is an effective prognostic factor in patients with luminal B (HER2−) breast cancer and is more specific than CCL5. Our results demonstrate the interactions between cancer cells and microenvironment quantitatively, opening up a new field for predicting the clinical outcome in luminal B (HER2−), and indicate the need for more intensive investigations of the related biomarkers in this unique subtype of breast cancer.
Acknowledgments
This work was supported by funds from the Science and Technology Planning Project of Wuhu China (2017cg21 to Y-YZ), the National Natural Science Foundation of China (81201524 to 81471781 to S-RS) and the National Natural Science Foundation of China (81302314 to J-JL).
Disclosure
The authors report no conflicts of interest in this work.
References
- DeSantisCEMaJGoding SauerANewmanLAJemalABreast cancer statistics, 2017, racial disparity in mortality by stateCA Cancer J Clin201767643944828972651
- YanagawaMIkemotKKawauchiSLuminal A and luminal B (HER2 negative) subtypes of breast cancer consist of a mixture of tumors with different genotypeBMC Res Notes2012537622830453
- FockeCMvan DiestPJDeckerTSt Gallen 2015 subtyping of luminal breast cancers: impact of different Ki67-based proliferation assessment methodsBreast Cancer Res Treat201615921727460637
- EffiABAmanNAKouiBSKoffiKDTraoreZCKouyateMBreast cancer molecular subtypes defined by ER/PR and HER2 status: association with clinicopathologic parameters in Ivorian patientsAsian Pac J Cancer Prev20161741973197827221883
- HolowatyjANRuterbuschJJRatnamMGorskiDHCoteMLHER2 status and disparities in luminal breast cancersCancer Med2016582109211627250116
- BediagaNGBeristainECalvoBLuminal B breast cancer subtype displays a dicotomic epigenetic patternSpringerplus20165111026759740
- LiZHHuPHTuJHYuNSLuminal B breast cancer: patterns of recurrence and clinical outcomeOncotarget2016740650246503327542253
- KnudsenESWitkiewiczAKDefining the transcriptional and biological response to CDK4/6 inhibition in relation to ER+/HER2− breast cancerOncotarget2016743691116912327564114
- ParkCParkKKimJPrognostic values of negative estrogen or progesterone receptor expression in patients with luminal B HER2-negative breast cancerWorld J Surg Oncol201614124427619909
- RajcJGugićDFröhlichIMarjanovićKDumenčićBPrognostic role of nectin-4 expression in luminal B (HER2 negative) breast cancerPathol Res Pract201721391102110828778498
- CancelloGMaisonneuvePRotmenszNProgesterone receptor loss identifies luminal B breast cancer subgroups at higher risk of relapseAnn Oncol201324366166823022996
- MiyagawaYMiyakeTYanaiAAssociation of body mass index with risk of luminal A but not luminal B estrogen receptor-positive and HER2-negative breast cancer for postmenopausal Japanese womenBreast Cancer201522439940524000037
- CriscitielloCDisalvatoreDDe LaurentiisMHigh Ki-67 score is indicative of a greater benefit from adjuvant chemotherapy when added to endocrine therapy in luminal B HER2 negative and node-positive breast cancerBreast2014231697524314620
- MaisonneuvePDisalvatoreDRotmenszNProposed new clinicopathological surrogate definitions of luminal A and luminal B (HER2-negative) intrinsic breast cancer subtypesBreast Cancer Res2014163R6524951027
- ZongYZhuLWuJProgesterone receptor status and Ki-67 index may predict early relapse in luminal B/HER2 negative breast cancer patients: a retrospective studyPLoS One201498e9562925170613
- SatoKMiyashitaMIshidaTPrognostic significance of the progesterone receptor status in Ki67-high and -low luminal B-like HER2-negative breast cancersBreast Cancer201623231031725380989
- CampbellMJBaehnerFO’MearaTCharacterizing the immune microenvironment in high-risk ductal carcinoma in situ of the breastBreast Cancer Res Treat20171611172827785654
- ChengKKDicksonAGujamFJMcMillanDCEdwardsJThe relationship between oestrogen receptor-alpha phosphorylation and the tumour microenvironment in patients with primary operable ductal breast cancerHistopathology201770578279727891654
- WuXLiuHLiuJImmunofluorescent labeling of cancer marker Her2 and other cellular targets with semiconductor quantum dotsNat Biotechnol2003211414612459735
- ChenCPengJXiaHQuantum-dot-based immunofluorescent imaging of HER2 and ER provides new insights into breast cancer heterogeneityNanotechnology201021909510120110584
- YangXQChenCPengCWQuantum dot-based quantitative immunofluorescence detection and spectrum analysis of epidermal growth factor receptor in breast cancer tissue arraysInt J Nanomedicine201162265227322072864
- SunJZChenCJiangGTianWQLiYSunSRQuantum dot-based immunofluorescent imaging of Ki67 and identification of prognostic value in HER2-positive (non-luminal) breast cancerInt J Nanomedicine201491339134624648732
- PengCWLiuXLChenCPatterns of cancer invasion revealed by QDs-based quantitative multiplexed imaging of tumor microenvironmentBiomaterials201132112907291721262536
- LiuXLPengCWChenCQuantum dots-based double-color imaging of HER2 positive breast cancer invasionBiochem Biophys Res Commun2011409357758221609713
- MiZBhattacharyaSDKimVMGuoHTalbotLJKuoPCOsteo-pontin promotes CCL5-mesenchymal stromal cell mesenchymal stromal cell-mediated breast cancer metastasisCarcinogenesis201132447748721252118
- ForstBHansenMTKlingelhöferJMetastasis-inducing S100A4 and RANTES cooperate in promoting tumor progression in micePLoS One201054e1037420442771
- RizviSBRouhiSTaniguchiSNear-infrared quantum dots for HER2 localization and imaging of cancer cellsInt J Nanomedicine201491323133724648731
- MichalskaMFlorczakADams-KozlowskaHGapinskiJJurgaSSchneiderRPeptide-functionalized ZCIS QDs as fluorescent nanoprobe for targeted HER2-positive breast cancer cells imagingActa Biomater20163529330426850146
- XuHChenCPengJEvaluation of the bioconjugation efficiency of different quantum dots as probes for immunostaining tumor-marker proteinsAppl Spectrosc201064884785220719046
- ChenCSunSRGongYPQuantum dots-based molecular classification of breast cancer by quantitative spectroanalysis of hormone receptors and HER2Biomaterials201132307592759921745686
- VelaeiKSamadiNBarazvanBSoleimani RadJTumor microenvironment-mediated chemoresistance in breast cancerBreast2016309210027668856
- WeitzenfeldPMeshelTBen-BaruchAMicroenvironmental networks promote tumor heterogeneity and enrich for metastatic cancer stem-like cells in luminal-A breast tumor cellsOncotarget2016749811238114327835603
- ChenXWangYNelsonDCCL2/CCR2 regulates the tumor microenvironment in HER-2/neu-driven mammary carcinomas in micePLoS One20161111e016559527820834
- SvenssonSAbrahamssonARodriguezGVCCL2 and CCL5 are novel therapeutic targets for estrogen-dependent breast cancerClin Cancer Res201521163794380525901081
- YiEHLeeCSLeeJKSTAT3-RANTES autocrine signaling is essential for tamoxifen resistance in human breast cancer cellsMol Cancer Res2013111314223074171
- NiwaYAkamatsuHNiwaHSumiHOzakiYAbeACorrelation of tissue and plasma RANTES levels with disease course in patients with breast or cervical cancerClin Cancer Res20017228528911234881
- Yaal-HahoshenNShinaSLeider-TrejoLThe chemokine CCL5 as a potential prognostic factor predicting disease progression in stage II breast cancer patientsClin Cancer Res200612154474448016899591
- BiècheILereboursFTozluSEspieMMartyMLidereauRMolecular profiling of inflammatory breast cancer: identification of a poor-prognosis gene expression signatureClin Cancer Res200410206789679515501955
- VittoriaDDomenicoLRosariaAMAdipose microenvironment promotes triple negative breast cancer cell invasiveness and dissemination by producing CCL5Oncotarget2016717244952450927027351
- GaoDRahbarRFishENCCL5 activation of CCR5 regulates cell metabolism to enhance proliferation of breast cancer cellsOpen Biol20166616012227335323
- YasuharaRIriéTSuzukiKThe β-catenin signaling pathway induces aggressive potential in breast cancer by up-regulating the chemokine CCL5Exp Cell Res20153381223126363360
- ZhangQQinJZhongLCCL5-mediated Th2 immune polarization promotes metastasis in luminal breast cancerCancer Res201575204312432126249173
- ReigosaAHardissonDSanziFCharacterization of patient-derived tumor xenografts (PDXs) as models for estrogen receptor positive (ER+HER2− and ER+HER2+) breast cancersJ Steroid Biochem Mol Biol2017170657427154416
- ReigosaAHardissonDSanziFCaleirasESaldiviaFFernándezASubclassification of the molecular types of breast cancer based on the expression of immunohistochemical markers and evolutionInvest Clin201657218721628429898
- PendharkarNGajbhiyeATaunkKQuantitative tissue proteomic investigation of invasive ductal carcinoma of breast with luminal B HER2positive and HER2 enriched subtypes towards potential diagnostic and therapeutic biomarkersJ Proteomics201613211213026642762
- OhlundDLundinCArdnorBOmanMNarediPSundMType IV collagen is a tumour stroma-derived biomarker for pancreas cancerBr J Cancer20091011919719491897
- CavoMFatoMPeñuelaLBeltrameFRaiteriRScaglioneSMicroenvironment complexity and matrix stiffness regulate breast cancer cell activity in a 3D in vitro modelSci Rep201663536727734939
- ChanNWillisAKornhauserNInfluencing the tumor microenvironment: phase 2 study of copper depletion with tetrathiomolybdate in high risk breast cancer and preclinical models of lung metastasesClin Cancer Res201723366667627769988
- OkabeMTohUIwakumaNPredictive factors of tumor immune microenvironment for long-term follow-up in early stage breast cancerCancer Sci201610818190