
Abstract
Placenta percreta is an obstetric condition in which the placenta invades through the myometrium. This is the most severe form of placenta accreta and may result in spontaneous uterine rupture, a rare complication that threatens the life of both mother and fetus. In this case report, we describe a 32-year-old woman in her fourth pregnancy, diagnosed with repeated placenta accreta, which was eventually complicated by spontaneous uterine rupture at 24 weeks’ gestation. This patient had a history of abnormal placentation in prior pregnancies and previous uterine injuries. This case demonstrates a pattern of escalating placental invasiveness, and raises questions regarding the process of abnormal placentation and the manifestation of uterine rupture in scarred uteri.
Introduction
Placenta accreta is a pathology characterized by abnormal and firm attachment of the placenta to the myometrium.Citation1 The depth of penetration of the placental villi into the myometrium defines three severity levels of placenta accreta; accreta, increta, and percreta. Accreta, the least severe and most common of the three, occurs when the placental villi attach directly to the myometrium rather than to the decidua basalis. Increta occurs when placental villi penetrate into the myometrium. Percreta, the most rare and severe manifestation of accreta, is the invasion of the placental villi through the entire thickness of the myometrium, and even further.Citation2
Placenta accreta tends to reoccur; however, little is known regarding the pathophysiological processes leading to this invasive placentation. The most severe complication of placenta accreta is spontaneous rupture of the uterus, which poses diagnostic challenges and management dilemmas, and can be a life-threatening event to the mother and fetus.
Herein, we describe a woman diagnosed with repeated placenta accreta that was complicated by spontaneous rupture of the uterus. This case demonstrates increasing placental invasiveness and, to the best of our knowledge, is a first report of this kind. Furthermore, repeated invasive placentation occurred at the same site, and not at the cesarean section (CS) scar, which raises a fundamental question regarding the mechanism of trophoblast implantation and location of recurrence of placenta accreta. After four consecutive pregnancies with abnormal placentation, spontaneous rupture of the uterus occurred. Understanding the processes that influence the timing and location of this life-threatening complication may set the basis for better diagnosis and management protocols.
Case report
A 32-year-old woman in her fourth pregnancy, with parity of 2, presented at 19 weeks’ gestation to the gynecologic emergency department with lower abdominal pain for the past 2 days. Her obstetric history included retained placenta in both first and second deliveries, which necessitated manual revision of the uterine cavity and curettage. She had a perforation of the left posterior uterine wall during curettage in her second delivery that was laparoscopically repaired. In her third pregnancy, she presented with an acute abdomen at 19 weeks’ gestation and underwent exploratory laparoscopy that demonstrated a 2.5 cm rupture in the posterior uterine wall at the site of the previous perforation. Laparoscopy was turned into laparotomy; the rupture was sutured and the patient recovered well. Magnetic resonance imaging (MRI) performed at 21 weeks’ gestation demonstrated placental tissue penetrating, but not perforating, the myometrium of the posterior uterine wall, which was indicative of placenta increta (). After counseling, the couple chose to terminate the pregnancy, and hysterotomy was performed at 22 weeks’ gestation.
Figure 1 MRI of placenta increta (third pregnancy).
Abbreviation: MRI, magnetic resonance imaging.

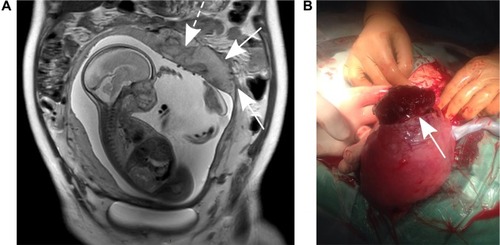
In the current pregnancy, upon admission to the emergency department, the patient presented normal vital signs, and the gynecologic examination revealed 19 weeks’ gestation – sized uterus, a closed cervix, and no vaginal bleeding. Transabdominal ultrasound scan suggested abnormal placentation (). This suspicion raised by sonography, together with the patient’s history, prompted an MRI at 24.2 weeks that demonstrated the presence of placenta percreta at the site of the previous placenta increta (). Following counseling, the couple decided to continue the pregnancy, and the patient was hospitalized for observation. Two days later, the woman reported severe abdominal pain. Rapid bedside ultrasound examination demonstrated intraabdominal bleeding, and emergency CS was performed. During laparotomy, massive intraabdominal bleeding was observed, originating from a uterine rupture with a perforating placental tissue (). Following the delivery of the fetus and complete placental removal, as well as suturing of the uterine wall, the bleeding stopped and hysterectomy was avoided. The mother recovered well, while her neonate died of prematurity complications. Due to the ominous nature of the patient’s obstetric history, she was advised to avoid future pregnancies.
Figure 2 MRI of placenta percreta (fourth pregnancy).
Abbreviation: MRI, magnetic resonance imaging.
Discussion
Placenta accreta, at any level of severity, is a rare obstetric complication with an estimated incidence of between 1 in 533 (as reported by Wu et alCitation3) and 1 in 2,500 pregnancies (as reported by Miller et alCitation1). However, once placenta accrete is diagnosed, it has a tendency to reoccur in subsequent pregnancies.Citation4,Citation5 Little is known about recurrence of placenta accreta, and specifically its location, histopathological invasiveness, and prognosis. The only known risk factor for repeated placenta accreta is parity.Citation6 Here we report, for the first time, a case of four consecutive pregnancies complicated by abnormal placentation.
In primary placenta accreta, the strongest independent risk factor has been found to be previous CS.Citation1,Citation7 This is explained by the tendency of implantation and placentation to occur in the scarred area.Citation1 In the case presented here, recurrence occurred in the left uterine cornu, the site of the previous placenta increta, rather than the CS scar. Additionally, the clinical manifestation was aggravated with each consecutive pregnancy: retained placenta necessitating manual lysis and curettage in the first and second, placenta increta in the third, and spontaneous uterine rupture due to placenta percreta in the fourth. Therefore, this case presents not only placenta accreta recurrence but also increased invasiveness of the placentation.
Even though placentation is prone to develop within previous CS scars, other prior uterine injuries may play a similar role, and hence are considered to be a risk factor for placenta accreta.Citation7 It is not known whether injury location affects the risk for placenta accreta. The correlation between scarred uteri and placenta accreta is explained by a relative hypoxic environment in the scar tissueCitation8 or the histologically abnormal structure of the scar. This abnormal structure is characterized by defective re-epithelialization and relative abundance of extracellular matrix.Citation9 Alternatively, prior uterine injury is associated with dynamic changes in decidual leukocyte distribution,Citation10 which subsequently affects the homing of the blastocyst to its implantation site.
Once placenta accreta is diagnosed, proper counseling and discussion with the patient should be undertaken regarding further management of the pregnancy in light of the complications involved.Citation11 The most severe complication is spontaneous rupture of the uterus, as seen in this case, which poses both a diagnostic challenge and an immediate risk to the life of both mother and fetus. The incidence of spontaneous uterine rupture is reported to be approximately one in 5,000; however, this includes etiologies other than placenta accreta.Citation12 Uterine rupture due to placenta accreta is extremely rare, and a systematic review of reported cases is yet to be done. In the past, most cases were managed by hysterectomy, but conservative treatment is becoming common recently.Citation13,Citation14 During the operation, active bleeding stopped promptly and the patient remained hemodynamically stable. Completing the procedure outweighed the risk of blood loss involved in hysterectomy, and uterine repair was technically feasible. Hence, we chose a conservative treatment approach and repaired the uterus.
The location where spontaneous uterine rupture occurs has not been thoroughly studied; however, some reports associate first trimester ruptures with the fundus and third trimester ruptures with the lower uterine segment.Citation15 In case of previous CS, the rupture usually occurs at the site of the old scar.Citation12 In our patient, the rupture appeared in the left uterine cornu, where the placenta was invading through the myometrium, rather than in the CS scar. This could be explained by the fact that the uterine wall was already disrupted by the placenta percreta prior to the rupture, as was seen in the MRI.
As with rupture location, factors affecting the timing of uterine rupture due to placenta accreta are unknown. While it is well established that spontaneous uterine rupture usually occurs in the third trimester,Citation15 there have been reports of firstCitation8 and secondCitation16–Citation19 trimester ruptures as well. In our case, spontaneous rupture occurred at 24 weeks’ gestation; a critical time for the fetus. This gestational age marks the limit of viability, since preterm delivery around this time results in 50% long-term survival probability of the newborn.Citation20 In the face of immediate risk for the mother, urgent CS was inevitable, even when considering the probable prematurity complications for the fetus. With the increase in conservative management of placenta percreta, this case highlights the grave prognosis of pregnancies following placenta accreta. Although systematic reviews of these complications are not yet available, this insight should be taken into account during counseling following conservative management of placenta accreta.
Acknowledgments
The authors advise that the Ben-Gurion University of the Negev institutional review board does not require that institutional review board approval or patient consent be obtained for case reports of a single patient.
Supplementary material
Video S1 Sonography of placenta percreta (fourth pregnancy).
Notes: Transabdominal two-dimensional ultrasound in the transverse plane showing an abnormal placenta with thinning of the myometrium in the left posterior uterine wall, indicated by an asterisk. Similar findings are seen in the longitudinal plane in addition to fundal placental lacunas (arrow head) with increased blood flow by color Doppler scanning.
Disclosure
The authors report no conflicts of interest in this work.
References
- MillerDACholletJAGoodwinTMClinical risk factors for placenta previa–placenta accretaAm J Obstet Gynecol19971772102149240608
- SalehJHHaneyEIPlacenta previa and accretaSciarraJJGynecology and ObstetricsPhiladelphiaLippincott Williams & Wilkins2004
- WuSKocherginskyMHibbardJUAbnormal placentation: twenty-year analysisAm J Obstet Gynecol20051921458146115902137
- VinogradAWainstockTMazorMA prior placenta accreta is an independent risk factor for post-partum hemorrhage in subsequent gestationsEur J Obstet Gynecol Reprod Biol2015187202425681995
- SentilhesLKayemGAmbroselliCFertility and pregnancy outcomes following conservative treatment for placenta accretaHum Reprod201025112803281020833739
- GielchinskyYRojanskyNFasouliotisSJEzraYPlacenta accreta – summary of 10 years: a survey of 310 casesPlacenta20022321021411945088
- UstaIMHobeikaEMAbu MusaAAGabrielGENassarAHPlacenta previa-accreta: risk factors and complicationsAm J Obstet Gynecol20051931045104916157109
- Timor-TritschIEMonteagudoAUnforeseen consequences of the increasing rate of cesarean deliveries: early placenta accreta and cesarean scar pregnancy. A reviewAm J Obstet Gynecol20122071142922516620
- JauniauxEJurkovicDPlacenta accreta: pathogenesis of a 20th century iatrogenic uterine diseasePlacenta201233424425122284667
- Sindram-TrujilloAPScherjonSAvan Hulst-van MiertPPKanhaiHHRoelenDLClaasFHComparison of decidual leukocytes following spontaneous vaginal delivery and elective cesarean section in uncomplicated human term pregnancyJ Reprod Immunol20046212513715288188
- OyeleseYSmulianJCPlacenta previa, placenta accreta, and vasa previaObstet Gynecol2006107492794116582134
- GardeilFDalySTurnerMJUterine rupture in pregnancy reviewedEur J Obstet Gynecol Reprod Biol1994561071107805960
- AlanisMHurstBSMarshburnPBMatthewsMLConservative management of placenta increta with selective arterial embolization preserves future fertility and results in a favorable outcome in subsequent pregnanciesFertil Steril20068651514.e3e717007851
- SentilhesLGoffinetFKayemGManagement of placenta accretaActa Obstet Gynecol Scand2013921125113423869630
- JangDGLeeGSYoonJHLeeSJPlacenta percreta-induced uterine rupture diagnosed by laparoscopy in the first trimesterInt J Med Sci2011858
- SiwatchSChopraSSuriVGuptaNPlacenta percreta: rare presentation of haemorrhage in the second trimesterBMJ Case Rep201310.1136/bcr-2012-007782
- MatsuzakiSMatsuzakiSUedaYA case report and literature review of midtrimester termination of pregnancy complicated by placenta previa and placenta accretaAJP Rep20151212611
- DahiyaPNayarKDGulatiAJSDahiyaKPlacenta accreta causing uterine rupture in second trimester of pregnancy after in vitro fertilization: A case reportJ Reprod Infertil2012131616323926525
- ZeemanGGAllaireAWhitecarPMoiseKJSecond-trimester presentation of placenta percretaAm J Perinatol199916947547810774763
- AllenMDonohuePDusmanAThe limit of viability – Neonatal outcome of infants born at 22 to 25 weeks gestationN Engl J Med1993329159716018179651