
Abstract
Fetal growth restriction (FGR) and preeclampsia are the major causes of neonatal morbidity and mortality, which affect up to 8% of all pregnancies. The pathogenesis in FGR is an abnormal trophoblastic invasion leading to compromised uteroplacental circulation. However, in spite of this understanding and identification of high-risk patients, the management options are limited. There are some new studies which have demonstrated the role of sildenafil citrate in improving vasodilatation of small myometrial vessels and therefore improvement in amniotic fluid index, fetal weight, and even uterine and umbilical artery Doppler patterns. We report here the case of a 31-year-old female with infertility and preconceptional thin endometrium responding well to sildenafil citrate, followed by conception. However, she presented with an early-onset FGR at 26 weeks of gestation, and again after treatment with sildenafil citrate, showed improvement in amniotic fluid index and fetal weight, finally resulting in delivery of a full-term healthy baby with uneventful neonatal course.
Introduction
Early-onset fetal growth restriction (FGR) accompanied by severe oligohydramnios is often associated with high perinatal morbidity and mortality.Citation1 Only a proportion of pregnancies with FGR show altered maternal peripheral vascular resistance, while some women may have elevated maternal peripheral vascular resistance in uterine arteries and hence poor perinatal outcome. In such pregnancies, if resistance values are normalized in later trimesters, there may be a significantly better outcome.Citation2 Some recent studies have shown that sildenafil citrate increases uterine blood flow and potentiates estrogen-induced vasodilation.Citation3 In this case of early-onset FGR, sildenafil citrate therapy was successful in managing FGR and accompanied severe oligohydramnios with a favorable neonatal and maternal outcome.
Case presentation
A 31-year-old female with a history of secondary infertility of 1 year and 6 months was referred to our clinic. She had two spontaneous miscarriages at tenth week of gestation, the last being 2 years and 6 months back, both followed by dilatation and curettage. After her last abortion, she did not conceive for 2 years. Multiple cycles of ovulation induction with oral agents as well as injectable gonadotropins were done. All follicular studies showed consistently thin endometrium of 6–8 mm around the time of ovulation. Routine investigations such as hysterosalpingogram, blood sugar, tuberculosis polymerase chain reaction of the endometrium, and antiphospholipid antibodies were normal. On hysteroscopy done 1 year back, uterine cavity was normal.
At our clinic, we started with follicular growth and endometrial thickness monitoring in natural cycle. Doppler for endometrial blood flow around the time of ovulation was suggestive of absent flow in zones 2, 3, and 4 of endometrium (Applebaum criteria).Citation4,Citation5 An attempt to improve the blood flow was made by starting Aspirin 75 mg, vitamin E, and Pentoxyfylline.Citation6 However, repeat Doppler around the time of implantation did not show any improvement.
In the next cycle, successful ovulation induction with gonodatropins was done, and trigger was given when the follicle was 18 mm, followed by intrauterine insemination. Luteal support was given with oral estrogen, progesterone, and vaginal Sildenafil citrate 25 mg (Alivher®; Akumentis Healthcare Ltd., Mumbai, India) twice a day in view of decreased endometrial blood flow in the previous cycle, which may be one of the causes of repeated abortions.Citation7 Doppler for endometrial blood flow around the time of implantation (7–8 days after ovulation) showed good flow in all the zones.
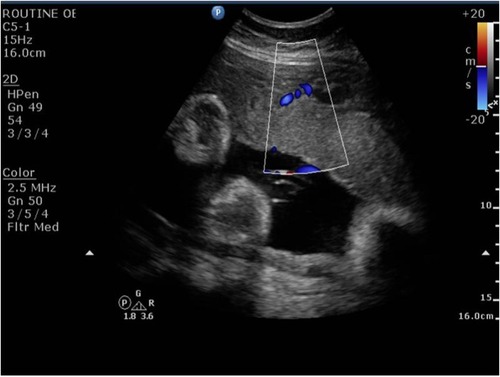
Serum β-human chorionic gonadotropin test done 14 days later confirmed the pregnancy. Sildenafil citrate was stopped on confirmation of pregnancy. First trimester of pregnancy was uneventful. Ultrasound at 12 weeks for nuchal translucency, nasal bone, and dual marker test were normal. Patient was called for follow-up visits every 3 weeks. Ultrasound for congenital malformation at 20 weeks did not reveal any abnormality. Fetal weight at that time was 440 g, and amniotic fluid index (AFI) was 10. Repeat ultrasound at 24 weeks was suggestive of oligohydramnios (AFI 6) with a fetal weight of 490 g (less than fifth percentile). Color Doppler in umbilical arteries showed normal systolic/diastolic (S/D) ratio, pulsatility index, and resistive index. However, there was notching seen in the uterine artery Doppler study. Investigations such as complete blood count, blood sugars, liver function test, renal function test, urine routine, and microscopy were within normal limits. Her blood pressure was normal; there was no peripheral pitting edema or proteinuria and hence no evidence of preeclampsia. The couple was informed regarding the guarded prognosis of pregnancy, and written informed consent was obtained voluntarily. The patient was kept on bed rest and given vitamin supplements, intravenous amino acid infusions, and nitric oxide donor (L-arginine sachets). Ultrasound at 26 weeks showed an estimated fetal weight of 550 g and an AFI of 4.5. Color Doppler showed an increased S/D ratio in the umbilical arteries with brain-sparing effect in the middle cerebral artery (MCA) as shown in and . A repeat ultrasonography at 27 weeks showed reduction in diastolic flow in the umbilical arteries. shows the ultrasonography Doppler image with reduced blood flow at the myometrial placental junction at diagnosis of intrauterine growth restriction.
Figure 1 Doppler of umbilical artery showing an increase in systolic/diastolic ratio (3.54) at the time of diagnosis of intrauterine growth restriction and starting sildenafil citrate.

Figure 2 Doppler of the middle cerebral artery showing an increase in systolic/diastolic ratio (4.29) and brain-sparing effect at the time of diagnosis of intrauterine growth restriction and initiating sildenafil citrate.
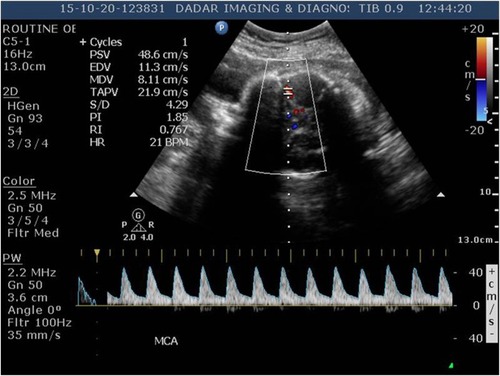
Figure 3 Doppler of the myometrial placental junction showing a reduced flow at the time of diagnosis of intrauterine growth restriction.
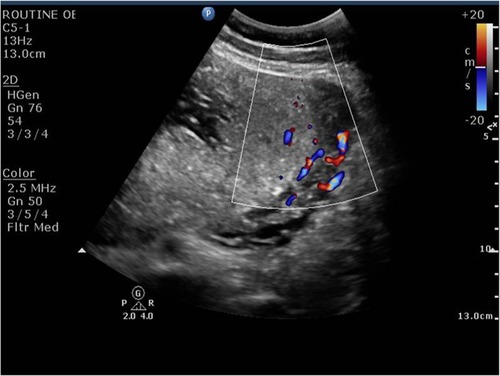
In view of grave prognosis of the pregnancy and unavailability of any other established definitive treatment, the couple was counseled regarding the limited role and experimental nature of Sildenafil citrate in oligohydramnios and FGR. After detailed counseling, the couple opted for Sildenafil citrate 25 mg vaginally twice a day. Repeat ultrasound at 28 weeks showed an improvement in blood flow and an increase in AFI to 6.5 with a fetal weight of 680 g after starting sildenafil citrate as shown in .
Figure 4 Doppler of the myometrial placental junction showing an improvement in flow after starting sildenafil citrate.
The umbilical artery diastolic flow improved after 2 weeks of therapy, with no brain-sparing effect in MCA; however, the S/D ratio was >3.
Furthermore, ultrasound at 30 weeks showed an AFI of 7.5 and a fetal weight of 1,000 g. The patient also experienced a subjective increase in perception of fetal movements. All medications were continued with weekly monitoring of fetal weight and AFI. Gradually at 31 weeks, there was further decrease in pulsatility index, and S/D ratio was <3, in both umbilical and MCAs as shown in and .
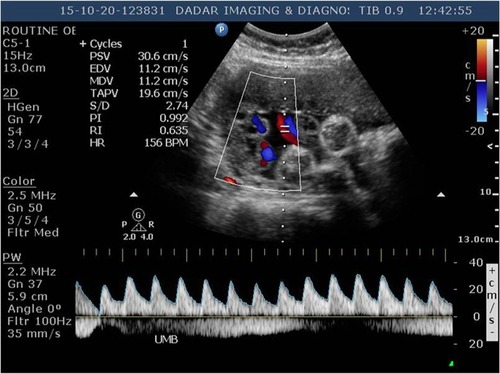
Figure 5 Doppler of umbilical artery showing normalization of systolic/diastolic ratio (2.52) after starting sildenafil citrate.
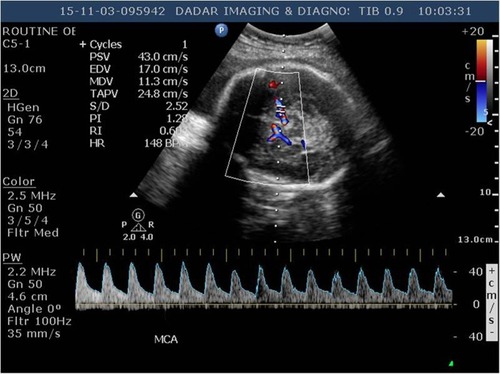
Figure 6 Doppler of umbilical artery showing normalization of systolic/diastolic ratio (2.74) after starting sildenafil citrate.
The fetal well-being was continuously monitored using biophysical profile every 2 weeks. Sildenafil citrate therapy was stopped at 36 weeks. An elective cesarean section was done at 37th week for breech presentation, and a healthy female child of 2.3 kg was delivered. Baby cried immediately after birth, and Apgar score was 7/10 and 9/10 at 1 and 5 minutes, respectively. Placenta was examined after delivery; on gross examination, it was smaller in size (400 g) with areas of calcifications and increased thickness of membranes. On histopathological examination, there were areas of infarction. The maternal and neonatal courses were uneventful. We have followed up the child up to 14 months with normal mental and physical development.
Discussion
Adequate placental blood flow is essential for the optimal delivery of nutrients from mother to fetus and for growth of conceptus. Restricted fetal growth results from pathophysiological and environmental factors, which alters uteroplacental blood flow, placental function, and therefore, nutrient availability to the fetus.Citation8,Citation9 There are still limited data on the efficacy of sildenafil citrate for treatment of FGR. In our case, we found sildenafil citrate useful in pregnancy complicated by severe oligohydramnios with FGR probably as it improves the placental perfusion.
Sildenafil citrate, a specific phosphodiesterase-5 inhibitor, has been proposed as a potential therapeutic strategy to maintain placental function and emerging as a potential candidate for the treatment of intrauterine growth restriction.Citation10 In this case of previous pregnancy losses and thin endometrium, vaginal sildenafil citrate improved the uterine artery blood flow and endometrial thickness and hence reduced the chances of miscarriages.Citation7 Further, when there was problem with the placental perfusion in second trimester, we restarted vaginal sildenafil citrate. Studies have shown that it helps in improvement of uteroplacental blood flow and in turn improves the fetal weightCitation3,Citation11,Citation12 by causing vasodilatation of the intramyometrial and intra-placental blood vessels. Increased uteroplacental blood improves the delivery of oxygen and other nutrients to fetus, which results in improved growth and development. However, there is no definitive treatment to improve the blood flow to the fetus.Citation8 Our case also showed a consistent increase in fetal weight and AFI with sildenafil citrate without any adverse fetal outcome. Sildenafil citrate by augmenting feto-placental blood flow in the setting of placental vascular insufficiency helps in increasing the AFI,Citation13 and this is one of the reasons why patients with oligohydramnios and FGR may benefit from sildenafil citrate. It increases the window of fetal maturity and hence reduces neonatal morbidity and mortality due to prematurity. Further studies and randomized controlled trials are needed to validate its usefulness and safety. In our case, the patient had persistent thin endometrium prior to conception and later also developed abnormal feto-placental blood flow and FGR. Whether there is any correlation between the two needs to be further researched and studied.
Acknowledgments
The authors are grateful to Mr Sandesh Kamdi for his assistance during the writing of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
- SibaiBDekkerGKupfermineMPre-eclampsiaLancet2005365946178579915733721
- SoregaroliMValcamonicoAScalviLDantiLFruscaTLate normalisation of uterine artery velocimetry in high risk pregnancyEur J Obstet Gynecol Reprod Biol2001951424511267718
- ZomaWDBakerRSClarkKEEffects of combined use of sildenafil citrate (Viagra) and 17betaestradiol on ovine coronary and uterine hemodynamicsAm J Obstet Gynecol200419051291129715167832
- CadkinAVApplebaumMUltrasonographic visualization of endometrial vascularity with ectopic pregnancyAm J Obstet Gynecol199116512361853905
- SchillerVLGrantEGDoppler ultrasonography of the pelvisRadiol Clin North Am19923047357421631280
- LebovitzOOrvietoRTreating patients with thin endometrium – an ongoing challengeGynecol Endocrinol201430640941424693854
- SherGFischJDVaginal sildenafil (Viagra): a preliminary report of a novel method to improve uterine artery blood flow and endometrial development in patients undergoing IVFHum Reprod200015480680910739824
- LeeMJConnerELCharafeddineLWoodsJRJrDel PrioreGA critical birth weight and other determinants of survival for infants with severe intrauterine growth restrictionAnn N Y Acad Sci200194332633911594552
- LamCLimKHKarumanchiSACirculating angiogenic factors in the pathogenesis and prediction of preeclampsiaHypertension20054651077108516230516
- Villanueva-GarcíaDMota-RojasDHernández-GonzálezRA systematic review of experimental and clinical studies of sildenafil citrate for intrauterine growth restriction and pre-term labourJ Obstet Gynaecol200727325525917464805
- von DadelszenPDwinnellSMageeLASildenafil citrate therapy for severe early-onset intrauterine growth restrictionBJOG2011118562462821392225
- WareingMMyersJEO’HaraMBakerPNSildenafil citrate (Viagra) enhances vasodilatation in fetal growth restrictionJ Clin Endocrinol Metab20059052550255515713717
- MaharajCHO’TooleDLynchTEffects and mechanisms of action of sildenafil citrate in human chorionic arteriesReprod Biol Endocrinol200973419389232