
Abstract
Background
Diabetes is one of the most common medical conditions affecting pregnancy and is associated with a number of adverse fetal, infant, and maternal outcomes. These adverse outcomes can be avoided or minimized with appropriate prepregnancy care (PPC). However, the uptake of PPC is limited in women with type 2 diabetes mellitus (T2DM). The reasons for poor uptake are multifactorial, reflecting both women’s understanding of pregnancy risks, and limitations in care delivery.
Methods
A systematic literature review with meta-synthesis was undertaken to identify qualitative studies exploring experiences of PPC for women with T2DM incorporating the views of women with T2DM and health care professionals (HCPs). Identified studies included were synthesized in a meta-ethnography to develop an understanding of the elements contributing to the uptake of PPC among women with T2DM.
Results
The systematic review identified seven studies yielding data from 28 women with T2DM and 83 HCPs. The following six third-order constructs were identified from the synthesis: understanding PPC, emotive catalysts, beliefs about reproduction among women with T2DM, relationships and social factors, HCP behaviors and perspectives, and health care system factors. These constructs were used to develop a multifactorial model expressing the interactive issues that shape the reproductive health-seeking behaviors of women with T2DM to identify potential areas for intervention.
Conclusion
The uptake of PPC among women with T2DM seems to be informed by their personal orientation to their reproductive needs, their interactions with HCPs, and system-level influences. Future interventions to enhance PPC uptake need to address these underlying issues.
Introduction
Diabetes is one of the most common medical conditions affecting pregnancyCitation1 and is associated with adverse fetal, infant, and maternal outcomes.Citation2 Many of these adverse outcomes can be avoided or minimized with appropriate care prior to and during pregnancy.Citation3,Citation4 Prepregnancy care (PPC) is particularly important as fetal development commences in the first trimester of pregnancy, before many women are aware of their pregnancy. Hence, current National Institute for Health and Care Excellence guidance stipulates that all women with diabetes considering pregnancy should receive PPC to normalize glucose levels, discontinue teratogenic therapies, and introduce high-dose folic acid.Citation5
Traditionally, the focus on PPC has been on women with type 1 diabetes mellitus (T1DM). However, with increasing obesity levels, the prevalence of type 2 diabetes mellitus (T2DM) is rising among women of childbearing ageCitation6,Citation7 and is particularly high in women of African or Asian origin.Citation8 The recent UK National Pregnancy in Diabetes (NPID) audit showed that women with T2DM now constitute 47% of pregnancies with preexisting diabetes.Citation9
While there is good evidence to show that PPC can significantly reduce adverse pregnancy outcomes,Citation10–Citation13 uptake of this care is limited, particularly in women with T2DM.Citation3,Citation4,Citation9 Consequently, studies consistently showed that women with T2DM were generally more likely to be poorly prepared for pregnancy compared to those with T1DM.Citation3,Citation4,Citation14 The NPID audit found that less than a third and a fifth of women with T2DM entering pregnancy care had adequately optimized glycemic control and been prescribed an appropriate dose of folic acid, respectively. They also reported that 10% of pregnant women with T2DM were still taking teratogenic drugs.Citation9 It is also increasingly recognized that many pregnancies in women with T2DM are unplanned. Hence, PPC also needs to consider wider aspects of reproductive care, including the provision of effective contraception.
In the UK, a further impediment for accessing PPC in women with T2DM is that most T2DM care is delivered in primary care, whereas the majority of PPC is situated in specialist diabetes centers.Citation15 Therefore, unlike T1DM, where the diabetes and PPC services are integrated, PPC is not co-located with routine T2DM care. This dissociation may impact on the accessibility of PPC to women with T2DM and restrict their access to health care professionals (HCPs) with expertise in reproductive health in the context of diabetes care.
To address this problem, interventions have been developed to enhance PPC uptake utilizing multimodal approaches that have included the following: patient education, health professional education, leafleting, and clinical guidelines.Citation3,Citation4,Citation14 However, such interventions have shown limited increases in PPC uptake in women with T2DM. The reasons for this poor uptake are likely to be multifactorial, reflecting both the women’s beliefs about pregnancy risks and the limitations of current care delivery models (including the women’s interactions with HCPs). Therefore, to develop more targeted and effective interventions, it is important to better understand the barriers and facilitators involving a combination of person and system factors. To this end, we present a meta-synthesis of the views and experiences of women and HCPs on PPC.
Methods
A systematic literature review with meta-synthesis was undertaken to address the following research questions:
What are women’s and HCPs’ views and experiences of PPC?
What factors contribute to the uptake of PPC?
Synthesis approach
The approach adopted for this synthesis was meta- ethnography, following the methods outlined by Noblit and HareCitation16 as adapted for health services research by Britten et al.Citation17 The synthesis was conducted in seven phases, and it is detailed as follows:
Phase 1: identify topic for synthesis: The review questions were developed from an analysis of current evidence for the uptake of PPC and an assessment of previously studied interventions to promote PPC uptake.
Phase 2: study identification: A systematic search was performed in the following databases: MEDLINE, Embase, PsycINFO, CINAHL, Maternity and Infant Care, and Web of Science. The search strategy was informed by an initial scoping review and included an extensive list of key terms and synonyms for the following: “type 2 diabetes”, “preconception”, “pre-pregnancy care”, and “pregnancy planning”. The titles and abstracts of all the identified studies were screened independently by two researchers and were selected according to the following inclusion criteria:
Studies that addressed the topic of PPC
Original research using qualitative methodologies
Participants were women with T2DM or HCPs who care for them.
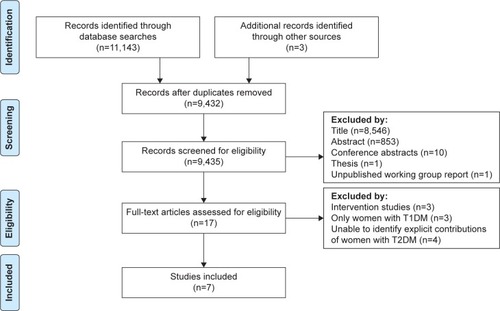
The interrater agreement between the two researchers was high with a Cohen’s kappa coefficient of 0.98. Given the complexity of the research topic, the electronic search was supplemented by secondary citation searching, key author searches and contacts with experts in the field of PPC.Citation18 The results of the search are summarized in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram in .
Figure 1 PRISMA flow diagram of database searches: summary of search strategy.
Data were extracted from the identified studies using a data extraction tool detailing: the research question, the aims and design of the study, the theoretical approach and analysis methods, participant characteristics and setting, and the findings of the studies (themes and data extracts). All of the identified studies included women with both T1DM and T2DM; however, only the data attributed to women with T2DM were extracted for inclusion in the synthesis. The data from the women with T2DM and HCPs were handled independently as separate syntheses. The extracted data were organized into first- and second-order constructs. First-order constructs were all the verbatim quotes attributable to women with T2DM or HCPs in each study, and the second-order constructs were the themes identified in the studies. Each study was critically appraised and scored using the Critical Appraisal Skills Programme qualitative research appraisal tool.Citation19 Data extraction and critical appraisal were undertaken independently by two researchers separately and then discussed until a consensus was reached.
Phase 3: initial reading and familiarizing: All of the articles were scrutinized thoroughly by two researchers; this involved reading and rereading each study.
Phase 4: determining how the studies are related: This involved a thematic tabulation of the primary data from all the studies to allow cross-study comparisons, integrate the themes from each study, and facilitate the identification of new concepts.Citation17,Citation20,Citation21 This tabulation was independently verified by two researchers.
Phase 5: translating the studies into one another: The first- and second-order constructs from each study were viewed within the tabulation detailed in phase 4 to develop third-order constructs, which are new ways of considering the studied phenomena. This involved translating the first- and second-order constructs from the original studies within a comparative matrix from which integrated themes were identified. These integrated themes were then used to identify the third-order constructs.
Phase 6: synthesizing the translations: A line of argument synthesis was used to validate the emerging themes and third-order constructs using both reciprocal (where findings are concordant) and refutational (where findings are divergent) synthesis. This ensured that the new third-order constructs identified provided a novel assessment of the collected data, while remaining connected to the data from the original studies. This synthesis involved collective discussions by the two researchers who conducted the previous phases of the synthesis.
Phase 7: communicating the synthesis: This must provide an account that enhances an understanding of the observed phenomena in the context of the underlying purpose of the inquiry.Citation16 A line-of-argument synthesis recognizes that studies address different aspects of a phenomenon.Citation22 Therefore, to better understand what contributes to the uptake of PPC among women with T2DM, which is the phenomena under investigation, this synthesis explored the experiences of women with T2DM and HCPs. An integrated model was then developed formulating the relationships between the identified constructs which also highlight areas for further study.
Findings
A total of seven studies met the inclusion criteria exploring the experiences and views of 28 women with T2DM and 83 HCPs from primary and secondary care inclusive of all members of the multidisciplinary team. provides an overview of all the included studies, and summarizes the second-order constructs supported by examples of first-order data from each study.
Table 1 Included studies for meta-synthesis
Table 2 First- and second-order constructs
The authors identified four third-order constructs related to the synthesis of the data pertaining to women with T2DM and two constructs expressing the experiences of HCPs. A detailed description of each of these constructs and their subthemes are presented in the following sections, supported by data from the original studies.
Construct 1: understanding PPC
The extent to which the women engaged with PPC was reflective of their understanding of the relationship between T2DM and pregnancy and the need for PPC.
Theme 1: information provision
Many women reported a lack of engagement with PPC, because they were not informed about why it was needed, and one woman stated that “she would have attended preconception care had she known that the service existed.”Citation23 The information was often delivered in an ad hoc way, such that the women could conceive prior to the information being imparted.
I’ve only been told the second time I went [for clinic appointment], and they said “Oh, by the way, if you’re planning to get pregnant, you know, you have to go on insulin ….” I could have got pregnant all that time before!Citation24
Theme 2: interactions with HCPs
Women with T2DM reported that the way HCPs approached a discussion about pregnancy and the need for PPC influenced how receptive they were to the guidance given.
It’s just the whole attitude, you know, it was like it didn’t matter … maybe I’m just one person, but it’s important for me if it’s not for them.Citation24
Some women perceived that HCPs did not consider their reproductive needs or provide supportive information about pregnancy or PPC due to biased views about their age or because they were obese.
I feel they just look at me and say, “she’s fat – just push her off to one side and that’s it,” … that’s how I feel all the time.Citation24
Theme 3: perceived relevance of PPC information
The women’s engagement with PPC was related to how receptive they were to receiving information on planning for pregnancy. Some women reported that they did not want information about PPC and were ambivalent about a potential pregnancy. Others avoided discussing plans for pregnancy with their health care team, as it might be a “deterrent to having children”.Citation24
I mean we weren’t really thinking about it (pregnancy) at that time so I mean it was all like pushed to one side. Yeah, so I probably wouldn’t have taken much notice about it.Citation25
The focus of the information and its perceived relevance also influenced how the women responded to PPC advice. Some women reported having received PPC but felt that the central focus was on general factors such as diet and exercise rather than the relationship between diabetes and a future pregnancy. The women felt that the relevance of information would be enhanced if it emphasized the potential benefits of PPC for both themselves and their offspring, as a partner of one woman voiced:
She didn’t like the horror stories as she calls them; all the bad things that could happen …. I suppose looking back, in hindsight, they could have counterbalanced that with all the good things that could happen. (Partner)Citation25
Construct 2: emotive catalysts
Many of the women voiced strong emotions (guilt, fear, and anxiety) about their reproductive capacity and risks. These emotional responses were associated with concerns for the health of a future baby and the loss of control over their reproductive intentions. These emotive catalysts can induce negative behavioral responses such as avoidance behaviors in respect of PPC.
Theme 1: health concerns for their offspring
The decision to become pregnant while having diabetes can lead to anxieties as to whether they would be able to “adequately control” their diabetes to protect their baby. Such thoughts may inhibit women from engaging in PPC if those anxieties were not addressed.
It’s more miscarriage, its more stillbirth … […] but it seems to me that if you’ve already got problems they just escalate, so I don’t know, I’m frightened … you just have to wait and see if something really horrible happens to it [baby].Citation23
Previous pregnancy experiences can heighten women’s concerns about their offspring. One woman while reflecting on a previous unplanned pregnancy described how her experience would make her more likely to take up PPC for a future pregnancy.
I’ve never been this scared or shocked in my whole life … it’s still sinking in so I would definitely want to get my, the whole of my body sorted before I did anything like this ever again.Citation25
Theme 2: pregnancy eclipsed by diabetes
Women also expressed emotions in relation to how their diabetes may lead to a loss of personal control over their pregnancy. Such perceptions were a deterrent to engaging with PPC as they wanted a normal pregnancy experience and PPC could mean that even prior to their pregnancy their diabetes would take precedence.
I would not want to bother with it’ cause I would want that bit of my life to be as normal as possible.Citation25
The women also reported an underlying anxiety about their ability to control their diabetes and how this could impact on their pregnancy.
… this may sound really silly but by focusing on the diabetes, I feel I lose control of it because it nerves me, it frightens me then and I start panicking about it [pregnancy].Citation23
Construct 3: beliefs among women with T2DM about reproduction
Beliefs and cultural perspectives about reproductive health were strongly reflected in the women’s narratives. These beliefs were influential in the women’s reproductive behaviors, including internalized beliefs about reproduction and diabetes and the desire to conform to cultural norms.
Theme 1: beliefs about contraception
The women reported contrasting beliefs about contraception. There were beliefs that contraception was not necessary because the women’s diabetes meant they would not get pregnant or that contraception, particularly oral contraception, was inappropriate for people with diabetes.
Well my doctor didn’t give me the pill … No, “cause I’ve got diabetes and you know, I’m not the most em, the best diabetic I think …”Citation25
Some beliefs may have resulted in the suboptimal use of contraception.
… I wasn’t takin’ it as regular as I should have done. Yeah, I was sort of missing one and thinking Oh that’s all right, I’ll take two in the morning and … it doesn’t work like that, does it?Citation25
Theme 2: fertility beliefs
Beliefs about fertility and diabetes among women with T2DM influenced their behaviors related to pregnancy planning. In particular, some women believed that diabetes or the consequence of diabetes would diminish their fertility reducing the perceived relevance of PPC.
… because I didn’t ever think that I would be able to have children. I just thought that that was a lot harder to conceive with having diabetes.Citation25
Theme 3: ambivalence toward planning pregnancy
Some women with T2DM held the belief that pregnancy outcomes were more down to chance or the “luck of the draw”.Citation24 This belief undermined the significance of diabetes for pregnancy, and they did not recognize the importance of PPC. As one multiparous woman relayed: “[they were] all surprises … all just happened.”Citation26
Construct 4: relationships and social factors
External relationships particularly the views of partners were influential in women’s pregnancy planning behaviors. For some women, gender power dynamics were evident in these relationships with women ceding control to their partners over their reproductive practices.
Yes I was given information by my GP’s nurse, but I did not use contraception … My husband said, do not use any contraception we want a baby.Citation25
Other women recounted that having a supportive relationship increased their readiness to plan for pregnancy.
… We finally sort of sat down and said, Look you know, if we’re going to do this, we need to do it now, or forget about it.Citation26
Construct 5: HCP behaviors and perspectives
The accounts of HCPs identified a number of underlying perspectives on PPC that influenced their behaviors in relation to the initiation of PPC and the advice and support they provided to women.
Theme 1: HCPs’ understanding of PPC
The extent to which HCPs engaged in PPC was related to their understanding of the needs of women with T2DM. Some HCPs felt this aspect of diabetes care was not adequately addressed in their professional education, and hence they were unaware and ill-prepared to deliver PPC.
Not much attention was paid to this issue during the training courses, and now that we have only received subtle training; our information is not sufficient.Citation27
Knowledge deficits impacted on the proficiency of the care they provided, with some HCPs believing that care can be optimized after, rather than before conception. There was also a tendency to focus on glucose control, neglecting other aspects of PPC, such as discontinuing teratogenic medications.
… if they got pregnant and I would get there control as good as it was and I’d emphasize they must come and see us as soon as they’re pregnant.Citation28
Some HCPs reported that they were unaware that women with T2DM need PPC, but if informed that they would be more mindful of providing this care.
I’ve never really thought about this topic before but … I would say it’s definitely in primary care, we have to be aware, we have to highlight these cases where we probably hadn’t been doing.Citation28
Theme 2: recognizing reproductive potential
Many HCPs acknowledged that women with T2DM were not routinely considered in terms of their reproductive potential. Consequently, PPC was often not incorporated into diabetes care for these women.
… part of the problem is, type 2 diabetes for a lot of people is seen as a disease of the elderly. And more of our patients are middle-aged to old people, so thinking about pregnancy, is not automatic at all …Citation28
Some HCPs recognized the importance of avoiding and actively planning for pregnancy, as one general practitioner (GP) suggested that many women miss out on appropriate reproductive care if the focus is exclusively on those who declare a pregnancy intention.
I actually think rather than talking about preconception care, you talk about the … care of the potentially pregnant, rather than preconception, because you’ll miss a lot of people because people won’t be ready for preconception care advice.Citation28
Theme 3: HCPs’ perceptions of PPC
In general, HCPs perceived PPC to be very demanding for women and tended to emphasize the work commitments required and hazards in relation to pregnancy, rather than emphasizing the potential benefits of PPC.
The whole course of the pregnancy is going to be a lot of work. She’s going to be doing her blood sugars a lot more often than she usually does and her diet is going to have to be under much tighter control.Citation29
Some HCPs also held skeptical views about women’s ability to adhere to the self-management practices involved in PPC and pregnancy.
I think it’s just denial … [they think] Nothing’s going to happen to the baby. I’ll be OK if I skip a few days of my medication. I’ll be Ok if I don’t check my sugars …Citation29
Theme 4: the impact of sociocultural factors
HCPs identified that underlying sociocultural factors may influence how women view pregnancy. They attributed information deficits in relation to PPC to language and literacy deficiencies, particularly among women with T2DM from ethnic minority communities.
Language problems, education level and not being able to read, not comprehending.Citation29
They also felt that cultural factors within families and communities influenced women’s reproductive behaviors to a greater extent than HCP advice.
It’s really interesting, the cultural things going on sometimes. In what he [the husband] perceives to be good for the pregnancy or what the patient’s mother-in-law thinks should go on for their future grandchild.Citation29
Addressing the views and knowledge deficits of family members was identified by one HCP as being helpful. However, cultural beliefs could be modified through addressing knowledge deficits helping to promote the uptake of PPC.
Husbands are usually unaware [about the need for pre-pregnancy care]. When they find out about the complications, they accept and pursue the matter.Citation27
Construct 6: health care system factors
Many HCPs identified limitations in the health care system as having a significant impact on the delivery of PPC.
Theme 1: integrated working
The views expressed by HCPs suggested a number of difficulties with care integration that inhibited PPC. A particular challenge relates to the delivery of care across different services and professional disciplines. One area of complexity was the relationship between primary and specialist diabetes care. HCPs described a lack of shared understanding and agreement between these services in how to best provide PPC and who should provide the care. There was a perception among some specialist HCPs that primary care professionals lacked the skills and resources to deliver PPC.
I would be very happy for GPs to deliver preconception care and then to tap into our system, into our team […] The problem is that some GPs … have no interest at all and their general level of diabetes care is very poor.Citation28
In contrast, other HCPs emphasized that it was not about who delivered the care, but rather the need to ensure the provision of reliable consistent information across the multidisciplinary team.
I don’t think it matters who gives the message as long as we’re all giving the same consistent message, GPs, practice nurses, health visitors, community midwives, everyone …Citation28
HCPs offered ideas on how to enhance care integration suggesting a more blended and collaborative care approach.
You might do a bit of collaboration and mix and match … I might say why don’t you [the patient] go and have a one-off appointment, talk about what are issues for preconception care, maybe … and then let us [primary and secondary care] share the care.Citation28
Theme 2: resource constraints
The HCP accounts suggested that a barrier to women accessing PPC was either implicit or explicit care rationing. There was a perception that referring women to a specialist PPC clinic may not be an appropriate use of resources, as expressed by this primary care HCP:
If they’re not pregnant when do you make the referral without hugely increasing the workload of the clinic at hospital? Will they be able to cope if you’re referring 10 women who are trying to get pregnant but none of them are pregnant.Citation28
The resource question was further complicated by the impact of remuneration and commissioning models. These models can reduce the incentive for HCPs to refer women to PPC, as they may be outside of current remuneration frameworks particularly in primary care.
The government has set up conflicting incentives. On the one hand you must identify all disease groups and all risks. And be judged upon how well you do that. On the other hand if you refer patient to hospital, you’re going to be financially penalized.Citation28
Theme 3: system-level constraints
For many HCPs, particularly those in primary care, rationing in the organization and delivery of health care placed significant constraints on the PPC they provided. The most significant of these was the difficulty in incorporating a PPC strategy within an overburdened care system.
[…] you’re under such pressure in terms of time in a general consultation, you know, you might have 10 minutes, it’s um, unless there is a system that alerts you to consider it, it’s unlikely to get into, you know, you’re just dealing with now.Citation28
HCPs also identified that the overall care system is orientated to priorities other than PPC. In primary care, priority is given to clinical outcome targets and compliance with following embedded protocols that do not include PPC.
People often go by what’s on the templates and, you know, that’s not a part of it. So, I think if you’re rushing and you’re filling in templates, it’s not on it, it might be an idea to put that in …Citation28
Integrative model
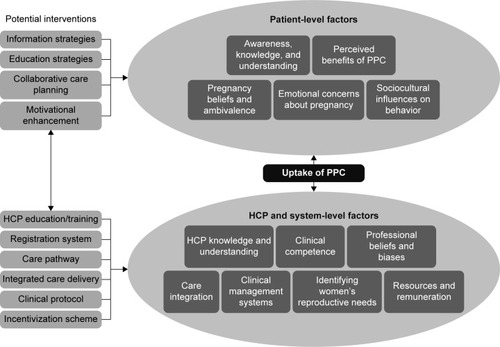
To represent the co-dependent relationships between the patient, HCP, and system-level elements contributing to the uptake of PPC, a model is shown in . This illustrates the complex nature of the issues involved in providing support for women with T2DM in managing their reproductive needs. At the patient level, this extends beyond having an awareness of why it is important to manage fertility or prepare for pregnancies, to include an understanding of the emotional, cognitive, motivational, and social phenomena that influence their health-seeking behaviors and responsiveness to care. Similar factors contribute to the care-providing behaviors of HCPs and indeed their awareness, knowledge, clinical skills, and beliefs about the reproductive needs of women with T2DM. The model also highlights the multiple care system limitations that prejudice the delivery of appropriate PPC. In presenting competing priorities and tensions within the wider care system, it was possible to identify key areas for intervention to enhance PPC uptake. The limitations in time and specialist resources combined with malaligned financial incentives prejudice the delivery of appropriate PPC, and these areas are explored further in the “Conclusion” section.
Figure 2 Integrated model of elements contributing to PPC uptake and potential interventions.
Conclusion
This synthesis, generated from the integrated views and experiences of women with T2DM and HCPs, has provided a deeper understanding of elements contributing to the uptake of PPC among women with T2DM. It is clear that the uptake and effectiveness of PPC require more than simply providing information to women about the importance of managing their reproduction and pregnancy planning.Citation30 While such information may increase the awareness of women about PPC, underlying beliefs, emotional concerns, and social factors also need to be considered to ensure that the women become actively engaged with and benefit from PPC. This suggests that in addition to using various media for a multimodal and staged approach, women’s beliefs and anxieties about pregnancy are actively explored prior to interventional strategies to increase the women’s engagement and activation in relation to their reproductive health. This may require the development of more collaborative and motivational methods of care delivery such as collaborative care planning.Citation5
The synthesis has highlighted that the approach of HCP to woman in providing support is also important. Previous studies have emphasized that a positive relationship between the patients and HCPs can influence the experience of PPC for women with T1DM.Citation31 However, this synthesis has shown that HCPs often do not consider the reproductive potential of women with T2DM and in some cases may hold negative views of the women, particularly in relation to weight, prejudicing discussions about pregnancy.Citation24 Hence, HCPs should be supported in developing consultation skills that elicit women’s pregnancy intentions, allow them to voice any concerns or anxieties, and foster a productive relationship for the delivery of PPC.Citation32,Citation33
The synthesis of both the women with T2DM and HCPs identified the impact of social and cultural factors on women’s reproductive choices. Interventions may need to consider not only the women’s views but wider family and community influences. Social relationships, especially spouses, may be influential, involving them in the PPC discussion may help women adopt protective behaviors by encouraging women to voice their beliefs and views on pregnancy. At a wider level, it may be useful to work with specific ethnic communities to help promote an understanding of PPC. Given the preponderance of diabetes in women of childbearing age in some ethnic communities, such approaches may enhance PPC awareness and uptake.Citation34
Patient education has a role to play in promoting an understanding of reproductive health issues in diabetes. Women observed that there can be a delay between diagnosis of diabetes and when they receive advice about pregnancy. During that period, women are vulnerable to an unplanned pregnancy. Currently, while all people newly diagnosed with T2DM are offered structured education,Citation35 most education does not address reproduction.Citation36 Therefore, education strategies may be useful soon after diagnosis and need to address the wider factors associated with women’s reproductive behaviors. Women reported that experiencing a pregnancy can influence future pregnancy planning, thus it may be useful to include the personal experiences of multiparous women as part of educational resources.
The HCPs’ accounts suggest that there is a need to extend training and skills in managing the reproductive care needs of women with T2DM, especially in primary care where most T2DM is managed. Such training needs to consider the requirements of women not only actively aiming for pregnancy but also preventing unplanned pregnancies. HCP education needs to address potentially unhelpful beliefs about obesity, age, and diabetes in terms of fertility and fecundity. Education should challenge HCP biases that can negatively impact the therapeutic relationship with women with T2DM.
Finally, unlike the general population where ∼55% of pregnancies are considered planned,Citation37 women with T2DM require specific care to target their additional risk factors. This synthesis has identified that the current care system is not orientated to promoting and delivering effective PPC for women with T2DM. There are inconsistencies in the care provided and lack of integration between primary care and the specialist diabetes teams running PPC services. While the recent guidelines for pregnancy in diabetesCitation5 incorporating PPC and current practice make many recommendations, there is a disconnect between PPC models of delivery; hence, new strategies are required to implement these guidelines. PPC has been more prudently addressed for other medical conditions, such as epilepsy, and the resulting rates of planned pregnancies are more reflective of the general population.Citation38 Internationally, there are registries for epilepsy and pregnancy,Citation39,Citation40 and within the UK the provision of PPC for these women is incentivized within primary care.Citation41,Citation42 Future recommendations from our findings suggest that a new model of service delivery is required for women with T2DM. This new approach would incorporate comprehensive methods for registering and reviewing women of childbearing age, better care protocols with built-in decision-making tools and prompts, and clear clinical pathways with criteria for referral to specialist PPC. In the UK, a significant barrier is that reproductive health in diabetes is not part of the national incentive program in primary care and consequently is given a low priority.Citation43 Incentivizing PPC or bringing in performance monitoring either locally or nationally may increase the performance in reproductive care.Citation44 While some areas of the UK have already begun to adapt systems to enhance the uptake of PPC,Citation45,Citation46 these developments have not targeted women with T2DM specifically and the impact has not been systematically evaluated.
Limitations
While the review was designed and conducted following an explicit and rigorous methodological approach, there are some limitations to consider. Principal among these were the limited number of qualitative studies for the synthesis and the fact that these studies were not exclusive to women with T2DM. While we attended to the latter issue by only including data from women with T2DM, this restricted the scope of our interpretation and hence there may be additional factors that we have not identified. Nevertheless, the synthesis has provided novel insights into the collective factors impacting on PPC. These insights will be a useful reference for further exploratory studies and in developing new interventions.
In conclusion, the limited uptake of PPC is multifactorial and depends on patient, HCP, and care system. The findings suggest that multimodal approaches are required to improve PPC uptake with a view to optimizing the health of women with T2DM and their babies and reducing the number of unplanned pregnancies. Acknowledging the complexities exposed in this synthesis, the development of such approaches should involve women with T2DM and HCPs to ensure that interventions are sensitive to their needs. The synthesis also emphasizes the need to address system- and policy-level inconsistencies.
Acknowledgments
This study was funded by the Foundation of European Nurses in Diabetes (FEND). Open access for this article was funded by King’s College London.
Disclosure
The authors report no conflicts of interest in this work.
References
- BrydonPSmithTProffittMGeeHHolderRDunneFPregnancy outcome in women with type 2 diabetes mellitus needs to be addressedInt J Clin Pract200054741841911070563
- NegratoCAMattarRGomesMBAdverse pregnancy outcomes in women with diabetesDiabetol Metab Syndr2012411622260334
- MurphyHRRolandJMSkinnerTCEffectiveness of a regional prepregnancy care program in women with type 1 and type 2 diabetes: benefits beyond glycemic controlDiabetes Care201033122514252021115765
- MustafaEKhalilSKirwanBA regional pre-pregnancy care (PPC) programme for women with type 1 and type 2 diabetesIr Med J20121055 suppl111322838100
- National Institute for Health and Care Excellence (NICE)Diabetes in Pregnancy: Management from Preconception to the Postnatal PeriodLondonNICE2015
- BellRBaileyKCresswellTNorthern Diabetic Pregnancy Survey Steering GroupTrends in prevalence and outcomes of pregnancy in women with pre-existing type I and type II diabetesBr J Obstet Gynaecol20081154445452
- DabeleaDMayer-DavisEJSaydahSSEARCH for Diabetes in Youth StudyPrevalence of type 1 and type 2 diabetes among children and adolescents from 2001 to 2009J Am Med Assoc20143111717781786
- ThanabalasinghamGOwenKRType 2 diabetes in the young: why we should worryPract Diabetes2014316225227
- Healthcare Quality Improvement Partnership (HQIP) NDANational Pregnancy in Diabetes Audit 2014England, WalesIsle of Man2015
- SteelJMJohnstoneFDHepburnDASmithAFCan prepregnancy care of diabetic women reduce the risk of abnormal babies?Br Med J19903016760107010742249069
- KitzmillerJLGavinLAGinGDJovanovic-PetersonLMainEKZigrangWDPreconception care of diabetes. Glycemic control prevents congenital anomaliesJ Am Med Assoc19912656731736
- RosennBMiodovnikMCombsCAKhouryJSiddiqiTAPreconception management of insulin-dependent diabetes: improvement of pregnancy outcomeObstet Gynecol19917768468492030855
- McElvySSMiodovnikMRosennBA focused preconceptional and early pregnancy program in women with type 1 diabetes reduces perinatal mortality and malformation rates to general population levelsJ Matern Fetal Med200091142010757430
- WillhoiteMBBennertHWJrPalomakiGEThe impact of preconception counseling on pregnancy outcomes: the experience of the Maine diabetes in pregnancy programDiabetes Care19931624504558432216
- McDowellJRSMcPhailKHalyburtonGBrownMLindsayGPerceptions of a service redesign by adults living with type 2 diabetesJ Adv Nurs20096571432144119457006
- NoblitGWHareRDMeta-Ethnography: Synthesizing Qualitative StudiesNewbury ParkSage1988
- BrittenNCampbellRPopeCDonovanJMorganMPillRUsing meta-ethnography to synthesis qualitative research: a worked exampleJ Health Serv Res Policy2002720921512425780
- GreenhalghTPeacockREffectiveness and efficiency of search methods in systematic reviews of complex evidence: audit of primary sourcesBr Med J200533175241064106516230312
- Critical Appraisal Skills Programme (CASP) [homepage on the Internet]2014 Available from: http://www.casp-uk.net/Accessed October 18, 2016
- CampbellRPoundPPopeCEvaluating meta-ethnography: a synthesis of qualitative research on lay experiences of diabetes and diabetes careSoc Sci Med200365671684
- AtkinsSLewinSSmithHEngelMFretheimAVolminkJConducting a meta-ethnography of qualitative literature: lessons learntBMC Med Res Methodol20088111018215293
- ThorneSJensonLKearneyMNoblitGSandelowskiMQualitative metasynthesis: reflections on methodological orientation and ideological agendaQual Health Res200414101342136515538004
- LavenderTPlattMJTsekiriEWomen’s perceptions of being pregnant and having pregestational diabetesMidwifery201026658959519250724
- SpenceMAlderdiceFAHarperRMcCanceDRHolmesVAEducation and psychological aspects an exploration of knowledge and attitudes related to pre-pregnancy care in women with diabetesDiabet Med201027121385139121059091
- MurphyHRTempleRCBallVEEast Anglia Study group for Improving Pregnancy Outcomes in women with Diabetes (EASIPOD)Personal experiences of women with diabetes who do not attend pre-pregnancy careDiabet Med20102719210020121895
- LetherbyGStephenNStenhouseEPregnant women with pre-existing diabetes: family support in managing the pregnancy processHum Fertil2012154200204
- NekueiNKohanSKazemiAPreconception care in diabetic womenJ Educ Health Promot20154825767819
- MortagyIKielmannKBaldewegSEModderJPierceMBIntegrating preconception care for women with diabetes into primary care: a qualitative studyBr J Gen Pract20106058081582121062548
- MersereauPWilliamsJCollierSAMulhollandCTurayKPrueCBarriers to managing diabetes during pregnancy: the perceptions of health care practitionersBirth201138214214921599737
- VedharaKDaweKWetherellMAIllness beliefs predict self-care behaviours in patients with diabetic foot ulcers: a prospective studyDiabetes Res Clin Pract20141061677225112923
- HolingEVBrownZABeyerCSConnellFAWhy don’t women with diabetes plan their pregnancies?Diabetes Care19982168898959614603
- OlsonJKRelationships between nurse-expressed empathy, patient-perceived empathy and patient distressImage J Nurs Sch19952743173228530122
- GoldkampJAndersonSLifits-PodorozhanskyYGavardJAWomen’s perceptions regarding obesity and comorbidities and provider interactionJ Obstet Gynecol Neonatal Nurs2015446784792
- ZehPSandhuHKCannabyAMSturtJAThe impact of culturally competent diabetes care interventions for improving diabetes-related outcomes in ethnic minority groups: a systematic reviewDiabet Med201229101237125222553954
- National Institute for Health and Care Excellence (NICE)Type 2 Diabetes in Adults: ManagementLondonNICE2015
- DaviesMJHellerSSkinnerTCEffectiveness of the diabetes education and self management for ongoing and newly diagnosed (DESMOND) programme for people with newly diagnosed type 2 diabetes: cluster randomised controlled trialBr Med J2008336764249149518276664
- WellingsKJonesKGMercerCHThe prevalence of unplanned pregnancy and associated factors in Britain: findings from the third National Survey of Sexual Attitudes and Lifestyles (Natsal-3)Lancet201338299071807181624286786
- SabellaLDeaconCSauvéNEvaluation of counselling received by women with epilepsy in their reproductive years, types of antiepileptic drugs used and pregnancy outcomesJ Neurol Sci2015357e156
- Hernández-DíazSSmithCRShenANorth American AED Pregnancy RegistryNorth American AED Pregnancy RegistryComparative safety of antiepileptic drugs during pregnancyNeurology201278211692169922551726
- TomsonTBattinoDBonizzoniEEURAP Study GroupDose-dependent risk of malformations with antiepileptic drugs: an analysis of data from the EURAP epilepsy and pregnancy registryLancet Neurol201110760961721652013
- National Institute for Health and Care Excellence [webpage on the Internet]National Institute of Clinical Excellence Clinical Guideline 137: the epilepsies: the diagnosis and management of the epilepsies in adults and children in primary and secondary care2012 Available from: http://www.nice.org.uk/cg137Accessed August 25, 2016
- Health TDoInvesting in General Practice: The New General Medical Services Contract2003 Available from: http://webarchive.national-archives.gov.uk/20130107105354/http://www.dh.gov.uk/prod_con-sum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_4082710.pdfAccessed August 25, 2016
- Department of Health (DoH)Six Years on – Delivering the Diabetes National ServiceLondonDepartment of Health (DoH)2010
- HansenPGJespersenAMNudge and the manipulation of choice: a framework for the responsible use of the nudge approach to behaviour change in public policyEur J Risk Regul20131328
- NHS LutonThe Diabetes Pre-Conception Care Pilot ProjectLutonNHS Luton2011
- KingPA new model for preconception care in women with diabetesJ Diabetes Nurs20131725661
- MoherDLiberatiATetzlaffJAltmanDGThePGPreferred reporting items for systematic reviews and meta-analyses: The PRISMA StatementPLoS Med200967e100009719621072