Abstract
Ospemifene is a selective estrogen receptor modulator (SERM), or estrogen receptor agonist/antagonist, that was recently approved by the US Food and Drug Administration for the treatment of dyspareunia associated with vulvar and vaginal atrophy, a chronic condition that affects up to 60% of postmenopausal women. Ospemifene is the first and only nonestrogen compound approved for this indication. Compared with other approved SERMs, such as tamoxifen, toremifene, bazedoxifene, and raloxifene, the estrogen-like effects of ospemifene in the vaginal epithelium are unique. This review first discusses the rationale for developing ospemifene, including its mechanism of action, and then focuses on the clinical development of ospemifene for the treatment of dyspareunia associated with vulvar and vaginal atrophy. Included are discussions of the effects of ospemifene on the endometrium, serum lipids, coagulation markers, bone, and breast cancer. In conclusion, ospemifene is a SERM with a unique estrogen agonist/antagonist tissue profile that was recently approved in the US for the treatment of dyspareunia associated with vulvar and vaginal atrophy in postmenopausal women. Ospemifene warrants further clinical investigation for the treatment and prevention of osteoporosis and breast cancer.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Introduction
Ospemifene, Z-2-[4-(4-chloro-1,2-diphenyl-but-1-enyl)phenoxy]ethanol, is a novel nonsteroidal, nonhormonal selective estrogen receptor modulator (SERM). It is hypothesized that the primary mechanism of action of ospemifene is mediated through estrogen receptors.Citation1 The rationale for developing ospemifene as a therapeutic came from the observation that ospemifene was considered a weak/inactive hormonal metabolite of toremifene. This characteristic led to the hypothesis that developing a less potent hormonal agent could lead to a therapeutic benefit while carrying fewer adverse effects. By defining the dose-response relationship of ospemifene preclinically, a full clinical development program was initiated for osteoporosis and postmenopausal vulvar and vaginal atrophy (VVA). This ultimately led to the approval of ospemifene (60 mg/day orally) as the first nonhormonal, nonestrogen for the treatment of moderate to severe dyspareunia in women with menopausal VVA.
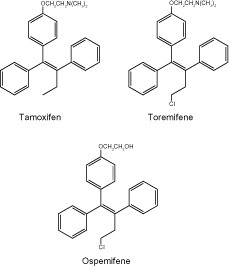
As shown in , ospemifene and tamoxifen, both triphenylethylenes, are structurally related. They differ in the side chain, with ospemifene containing a hydroxyl group in place of the tertiary amine of tamoxifen. Similar to toremifene, ospemifene also contains a chlorine atom. Ospemifene can be administered orally, transdermally, or parenterally. Food intake increases the absorption of ospemifene by 2–3-fold, and the calorie or fat content of the meal does not significantly affect the increase in bioavailability. It is proposed that increased bile production following ingestion of the meal may enhance the solubilization of ospemifene.Citation2 Ospemifene is mainly metabolized in the liver, is primarily excreted in the bile, and is eliminated in the feces.Citation3,Citation4
Figure 1 Chemical structures of approved triphenylethylene SERMs, (selective estrogen receptor modulator) ie, tamoxifen, toremifene, and ospemifene.
Ospemifene in VVA
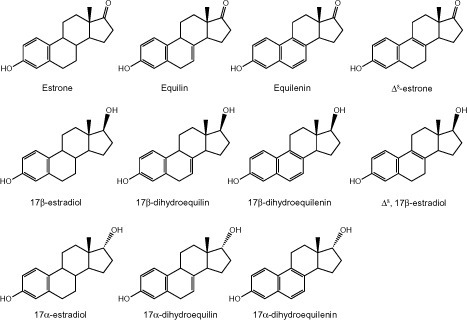
Approximately 60% of postmenopausal women who have never been treated with hormone therapy suffer from VVA.Citation5–Citation7 Among women who were treated with hormone therapy in the Women’s Health Initiative study, 30% reported the reappearance of symptoms within a week after treatment was discontinued.Citation8 Historically, the most effective treatment for VVA has been hormonal therapy with conjugated equine estrogens (), which carries a potential risk of stroke, coronary heart disease, thromboembolism, and breast cancer.Citation9 Local or vaginal estrogen therapy (17β-estradiol) is also used for treating women with VVA; however, systemic absorption and associated systemic side effects may still occur.Citation10–Citation12
Figure 2 Chemical structures of known steroidal estrogens found in the clinical formulation of conjugated equine estrogens.
Ospemifene was studied in two Phase II and three Phase III randomized trials as a treatment for VVA. In a placebo-controlled, randomized Phase II trial, 160 women were studied after 12 weeks of treatment with ospemifene 30 mg, 60 mg, or 90 mg, or placebo. Women in the ospemifene treatment groups showed significant improvement in superficial and intermediate vaginal epithelial cells in Papanicolaou smears.Citation13 Another randomized Phase II trial in 118 participants was conducted to examine the effect of ospemifene on the genital tract in comparison with raloxifene. Ospemifene again showed a clear estrogenic effect on the vaginal epithelium, as reflected by changes in the percentage of cells in the parabasal, intermediate, and superficial layers of Papanicolaou smears. This finding was in sharp contrast with the raloxifene group, which showed no changes from baseline.Citation14
A pivotal, placebo-controlled, randomized Phase III trial was performed in 826 postmenopausal women at 76 centers across the US. Participants were randomized into three groups to receive either 30 mg/day or 60 mg/day of ospemifene or placebo for 12 weeks.Citation15 The study showed a highly significant increase in vaginal epithelial cells and a significant decrease in parabasal cells in both ospemifene groups compared with placebo. In addition, significant improvements in the vaginal maturation index were observed within 4 weeks of treatment. Vaginal pH decreased significantly with both doses, but the pH decrease was higher in the group receiving 60 mg/day. After 12 weeks of therapy, the pH decreases were 0.67, 1.01, and 0.10, respectively, in the 30 mg/day, 60 mg/day, and placebo groups.Citation15
The second placebo-controlled, randomized Phase III trial was performed at 110 sites in the US and included a total of 605 postmenopausal women. This study compared ospemifene 60 mg/day with placebo for 12 weeks.Citation16 Again, there was a highly significant increase in the percentage of epithelial cells, and highly significant decreases in percentages of parabasal cells and vaginal pH. The most common side effects seen with ospemifene are shown in . The results of the Phase III trials led to the approval of ospemifene for the treatment of dyspareunia associated with VVA.
Table 1 Incidence of more common (≥1%) and rare side effects seen with ospemifene (60 mg) treatment compared with placebo
Effects of ospemifene on the endometrium
Endometrial safety has been closely examined in all clinical trials performed to date. In a double-blind, placebo-controlled, repeated-dose Phase I study, 40 healthy postmenopausal women were randomized to 25 mg, 50 mg, 100 mg, or 200 mg of ospemifene or placebo for 12 weeks. After 12 weeks, there were no significant changes in endometrial thickness from baseline, and there were no findings of secretory changes or hyperplasia.Citation17 All other trials additionally addressed endometrial changes and found very weak estrogenic effects on the endometrium. In the vast majority of participants, the endometrium remained atrophic at the end of 12 weeks of treatment. Overall, a slight increase in rate of proliferation was seen but no hyperplasia was found.Citation13–Citation16
The endometrial safety of ospemifene was further assessed in 180 nonhysterectomized postmenopausal women from the initial Phase III trial. These participants were randomized to continue treatment of ospemifene 30 mg/day or 60 mg/day for a total of 52 weeks. At the end of 52 weeks of therapy, endometrial biopsies were performed. There were no cases of endometrial hyperplasia or carcinoma, and the only proliferative findings observed were in one participant each in the 30 mg/day and 60 mg/day treatment groups.Citation18 These findings confirm the preclinical animal dataCitation1,Citation19 showing that ospemifene does not have any clinically relevant effects on the endometrium following one year of therapy.
Effects of ospemifene on lipids and coagulation markers
The effect of ospemifene on lipids was examined in two Phase II studies. In the first study, a randomized placebo-controlled trial in 160 healthy postmenopausal women, ospemifene was administered at 30 mg/day, 60 mg/day, or 90 mg/day. There were statistically nonsignificant decreases in total serum cholesterol, low-density lipoprotein, and oxidized low-density lipoprotein, and a nonsignificant increase in high-density lipoprotein. A significant increase in triglyceride levels was seen in the 90 mg/day ospemifene group. There were no significant changes in endothelial markers or homocysteine levels. However, fibrinogen as a marker for coagulation and fibrinolysis was significantly decreased in the 60 mg/day and 90 mg/day ospemifene groups. No changes were seen in generation of thrombin or D-dimer levels.Citation20
In the other Phase II trial comparing ospemifene with raloxifene, the total cholesterol level was significantly lower in the raloxifene group compared with all ospemifene groups (30 mg/day, 60 mg/day, or 90 mg/day) among a total of 118 participants. The low-density lipoprotein level decreased in the 90 mg/day ospemifene group but not at the 30 mg/day or 60 mg/day dose levels. Raloxifene lowered low-density lipoprotein levels significantly compared with ospemifene 30 mg and 60 mg, but no significant difference was seen between raloxifene and 90 mg/day of ospemifene. No changes in high-density lipoprotein levels were observed in any of the groups. A minor increase in triglycerides was seen in the 90 mg/day ospemifene group.Citation14 The results of these studies are inconclusive, and need to be added as endpoints in Phase IV studies.
Ospemifene and bone
Results from preclinical studies suggested that ospemifene has potential for the treatment and prevention of osteoporosis.Citation1,Citation21 In vitro studies have shown that the effects of ospemifene on osteoclasts are estrogen-like but appear to be distinct from raloxifene.Citation21 In vivo, ospemifene was shown to prevent ovariectomy-induced bone loss and maintain bone strength in ovariectomized rats at doses of 1 mg/kg and 10 mg/kg daily for 4 weeks.Citation1
The effects of ospemifene on serum biochemical markers of bone turnover were evaluated in two Phase II clinical trials in postmenopausal women. In the first trial, ospemifene 30 mg/day, 60 mg/day, and 90 mg/day was compared with raloxifene 60 mg/day, which is the dose approved for osteoporosis, for 12 weeks of treatment. Levels of serum biomarkers for bone resorption, including urinary N- and C-terminal cross-linking telopeptides of type I collagen, serum osteocalcin, bone-specific alkaline phosphatase, and procollagen type I N and C peptides (PINP and PICP, respectively) were not significantly different between raloxifene or ospemifene therapy.Citation22,Citation23 A second Phase II study comparing the effect of ospemifene 30 mg/day, 60 mg/day, and 90 mg/day with a placebo group on bone markers supported the findings of the first study. Levels of PINP, PICP, and bone alkaline phosphatase were significantly decreased after treatment with ospemifene compared with placebo.Citation22 These findings strongly suggest that ospemifene has positive effects on bone markers, justifying further studies aiming to determine if ospemifene lowers fracture rates in women at risk of developing osteoporosis.
Ospemifene and breast cancer
Similar to the development of tamoxifen and toremifene, ospemifene has been extensively studied as an antiestrogen in many preclinical breast cancer models.Citation24 The antiestrogenic activity of ospemifene in breast cancer was recently summarized.Citation25 Given the importance of breast safety during the treatment of VVA with ospemifene, a detailed discussion of these studies is presented.
In a xenograft model where MCF-7 (estrogen receptor-positive) and MDA-MB-231 (estrogen receptor-negative) human breast cancer cells were implanted in nude mice, ospemifene inhibited tumor growth in the implanted MCF-7 cells at oral doses of 10 mg/kg, 25 mg/kg, 50 mg/kg, and 100 mg/kg, whereas no effect was seen in MDA-MB-231 xenografts.Citation1,Citation26 These findings support the estrogen receptor-dependent activity of ospemifene.Citation26 In a chemically-induced estrogen receptor-positive breast cancer model, female Sprague Dawley rats were treated with dimethylbenzantharene, which induces breast cancer in rats. After 7–8 weeks of exposure, the rats were treated with ospemifene at 1 mg/kg, 10 mg/kg, or 50 mg/kg doses orally, and compared with vehicle control. The numbers of breast tumors in the 10 mg/kg and 50 mg/kg dose groups were significantly lower (31% and 5% of those in the vehicle control group, respectively). In the 0.1 mg/kg dose group, a significantly lower number of tumors was only observed after an additional 6 weeks of therapy.Citation1
In another chemically-induced estrogen receptor + breast cancer mouse model, Sencar mice were used to induce breast cancer with dimethylbenzantharene. In this study, ospemifene was compared with tamoxifen and raloxifene. Each mouse was subcutaneously implanted with two 20 mg medroxyprogesterone acetate time-release pellets to accelerate the formation of breast tumors. After 6 weeks of exposure to this carcinogen, 50 mg/kg doses of tamoxifen, raloxifene, or ospemifene were given to three different groups of mice for 37 weeks. The incidence of breast tumors was significantly reduced in the tamoxifen and ospemifene groups but not in the raloxifene group.Citation27 In a follow-up study, ospemifene was compared with tamoxifen directly. In this study, treatments were continued for 52 weeks. Of 20 mice in each group, one mouse in the ospemifene and none in the tamoxifen group developed tumors.Citation27 The findings in these chemically induced breast tumor models in rats and mice show that the chemopreventive effects of ospemifene are comparable with those of tamoxifen.Citation27
The mammary intraepithelial neoplasia outgrowth (MIN-O) mouse model, which resembles human ductal carcinoma in situ, was also used to study the effect of ospemifene in preventing breast cancer. The MIN-O model was derived from polyomavirus middle-T (PyV-mT) transgenic mice. These mice produce stable lines of transplantable MIN-O tissues.Citation28–Citation30 Ospemifene was studied in comparison with tamoxifen in transplanted mice. Mice were treated with 50 mg/kg doses of tamoxifen or ospemifene for 7 days prior to transplantation. At 3 and 10 weeks post transplantation, the mice were euthanized and examined. At 3 weeks, there were significantly smaller tumors in both the ospemifene and tamoxifen groups. At 10 weeks, there were significantly fewer breast tumors in both groups compared with control mice. Significantly smaller MIN-Os were also observed in both groups.Citation30
Most recently, the effects of ospemifene in both preventive and treatment settings were evaluated in a PyV-mT transgenic (MTag.Tg) C57BL/6 immunologically intact mouse model of spontaneous breast cancer.Citation31 This model is related to the MIN-O model described above, and involves the directed expression of the PyV-mT fusion gene in the mammary tissue of C57BL/6 mice, leading to rapid transformation of mammary tissue.Citation32 As in the MIN-O model, the progression of the cancer in this model has been shown to parallel human breast cancer development histologically and biologically.Citation32,Citation33 In this model also, ospemifene was shown to be effective both in prevention of tumor development and also as treatment after tumors were allowed to develop.Citation31
These extensive preclinical data strongly suggest that ospemifene and its major metabolite 4-hydroxyospemifene are antiestrogenic in animal models of estrogen receptor-positive breast cancer and ductal carcinoma in situ, with similar activity to tamoxifen. Future studies examining ospemifene as a chemopreventive agent in breast cancer are warranted.
Discussion
Approval of the nonhormonal estrogen agonist/antagonist ospemifene for the treatment of moderate to severe dyspareunia associated with VVA is a breakthrough for postmenopausal women, and is a stimulus for future drug development efforts. Ospemifene is the first nonhormonal estrogen receptor agonist/antagonist approved for this indication. Prior to approval of ospemifene by the US Food and Drug Administration, the only available treatment options for VVA were lubricants and moisturizers, which fail to address the underlying condition, or locally or systemically administered estrogen-based therapies, which have been the mainstay of treatment for VVA in postmenopausal women for many years.Citation34 Moisturizers and lubricants provide only temporary relief and are largely viewed as messy and cumbersome by postmenopausal women. The use of systemically administered estrogen-based therapies, either in the form of estradiol or conjugated equine estrogens, in hysterectomized women and estrogen plus progesterone in postmenopausal women with an intact uterus, can provide relief from VVA symptoms; however, there are a number of serious side effects associated with these treatments, including stroke, heart disease,Citation9,Citation35 and breast cancer,Citation36 and it remains unclear whether estrogen-based therapies are truly effective in treating VVA.Citation37,Citation38 While locally administered estrogen-based therapies greatly reduce systemic exposure, systemic absorption still occurs.Citation39
Another candidate for postmenopausal VVA currently being considered for approval by the US Food and Drug Administration is bazedoxifene combined with conjugated equine estrogens (BZA/CE). As a single agent, bazedoxifene is approved in Europe for postmenopausal osteoporosis. In a Phase III clinical trial comparing bazedoxifene alone with BZA/CE and placebo, bazedoxifene alone provided no benefit for VVA and hot flashes.Citation40 However, similar to estrogen alone, vasomotor symptoms and VVA were alleviated in postmenopausal women only when combining bazedoxifene with conjugated equine estrogens following 12 weeks of treatment.Citation41 Therefore, the benefits of this combination are solely attributed to conjugated equine estrogens, which is comprised of a multitude of equine estrogens (), and question the wisdom of combining bazedoxifene with conjugated equine estrogens in a 12-week study.Citation42 If the intent of bazedoxifene is to protect the endometrium from conjugated equine estrogens in a short course of therapy, this combination shows no potential advantage over ospemifene. Given the well known risks of chronic conjugated equine estrogen therapy reported in the Women’s Health Initiative trial, the same risks of stroke, cardiovascular events, breast cancer, and venous thromboembolism may still exist for the BZA/CE combination.Citation43 For example, in regard to breast cancer, whether bazedoxifene will protect breast tissue against conjugated equine estrogens is unknown. For these reasons, the use of BZA/CE for the treatment of VVA in healthy postmenopausal women should be approached with caution until long-term safety data are available well beyond 2 years.
Conclusion
Ospemifene is the first and only nonhormonal agent approved for the treatment of moderate to severe dyspareunia associated with menopause. This breakthrough brings a new nonestrogen alternative therapy for postmenopausal women suffering from the psychosocial and physiological effects of dyspareunia associated with VVA. Additionally, preclinical and clinical evidence suggests that ospemifene may have beneficial effects on bone and breast tissues. Future studies addressing these endpoints, as well as defining the safety profile of prolonged use (greater than one year), may provide support for the expanded use of ospemifene in postmenopausal women.
Disclosure
MWD is one of the original inventors of ospemifene and has a potential conflict of interest. The other authors report no conflicts of interest in this work.
References
- QuQZhengHDahllundJSelective estrogenic effects of a novel triphenylethylene compound, FC1271a, on bone, cholesterol level, and reproductive tissues in intact and ovariectomized ratsEndocrinology2000141280982010650964
- AnttilaMInventorHormos Medical Ltd, Turku (FI), assigneeMethod for enhancing the bioavailability of ospemifene US patent 8,470,890 B26252013
- GennariLMerlottiDValleggiFNutiROspemifene use in postmenopausal womenExpert Opin Investig Drugs2009186839849
- McCallJLDeGregorioMWPharmacologic evaluation of ospemifeneExpert Opin Drug Metab Toxicol20106677377920429673
- Calleja-AgiusJBrincatMPUrogenital atrophyClimacteric200912427928519387880
- NappiREPolattiFThe use of estrogen therapy in women’s sexual functioning (CME)J Sex Med20096360361619284468
- SantoroNKomiJPrevalence and impact of vaginal symptoms among postmenopausal womenJ Sex Med2009682133214219493278
- GradyDEttingerBTostesonANPressmanAMacerJLPredictors of difficulty when discontinuing postmenopausal hormone therapyObstet Gynecol200310261233123914662209
- RossouwJEAndersonGLPrenticeRLRisks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results From the Women’s Health Initiative randomized controlled trialJAMA2002288332133312117397
- LabrieFArcherDBouchardCIntravaginal dehydroepiandrosterone (Prasterone), a physiological and highly efficient treatment of vaginal atrophyMenopause200916590792219436225
- North American Menopause SocietyThe role of local vaginal estrogen for treatment of vaginal atrophy in postmenopausal women: 2007 position statement of The North American Menopause SocietyMenopause2007143 Pt 135536917438512
- SucklingJLethabyAKennedyRLocal oestrogen for vaginal atrophy in postmenopausal womenCochrane Database Syst Rev20064CD00150017054136
- RutanenEMHeikkinenJHalonenKKomiJLammintaustaRYlikorkalaOEffects of ospemifene, a novel SERM, on hormones, genital tract, climacteric symptoms, and quality of life in postmenopausal women: a double-blind, randomized trialMenopause200310543343914501605
- KomiJLankinenKSHarkonenPEffects of ospemifene and raloxifene on hormonal status, lipids, genital tract, and tolerability in postmenopausal womenMenopause200512220220915772568
- BachmannGAKomiJOOspemifene effectively treats vulvovaginal atrophy in postmenopausal women: results from a pivotal phase 3 studyMenopause201017348048620032798
- PortmanDJBachmannGASimonJAOspemifene, a novel selective estrogen receptor modulator for treating dyspareunia associated with postmenopausal vulvar and vaginal atrophyMenopause201320662363023361170
- VoipioSKKomiJKangasLHalonenKDeGregorioMWErkkolaRUEffects of ospemifene (FC-1271a) on uterine endometrium, vaginal maturation index, and hormonal status in healthy postmenopausal womenMaturitas200243320721412443837
- SimonJALinVHRadovichCBachmannGAOne-year long-term safety extension study of ospemifene for the treatment of vulvar and vaginal atrophy in postmenopausal women with a uterusMenopause201320441842723096251
- WurzGTHellmann-BlumbergUDeGregorioMWPharmacologic effects of ospemifene in rhesus macaques: a pilot studyBasic Clin Pharmacol Toxicol2008102655255818346046
- YlikorkalaOCacciatoreBHalonenKEffects of ospemifene, a novel SERM, on vascular markers and function in healthy, postmenopausal womenMenopause200310544044714501606
- QuQHarkonenPLVaananenHKComparative effects of estrogen and antiestrogens on differentiation of osteoblasts in mouse bone marrow cultureJ Cell Biochem199973450050710733344
- KomiJHeikkinenJRutanenEMHalonenKLammintaustaRYlikorkalaOEffects of ospemifene, a novel SERM, on biochemical markers of bone turnover in healthy postmenopausal womenGynecol Endocrinol200418315215815255284
- KomiJLankinenKSDeGregorioMEffects of ospemifene and raloxifene on biochemical markers of bone turnover in postmenopausal womenJ Bone Miner Metab200624431431816816926
- MorelloKCWurzGTDeGregorioMWSERMs: current status and future trendsCrit Rev Oncol Hematol2002431637612098608
- WurzGTSoeLHDegregorioMWOspemifene, vulvovaginal atrophy, and breast cancerMaturitas2013743220225
- TarasTLWurzGTDeGregorioMWIn vitro and in vivo biologic effects of ospemifene (FC-1271a) in breast cancerJ Steroid Biochem Mol Biol2001774–527127911457665
- WurzGTReadKCMarchisano-KarpmanCOspemifene inhibits the growth of dimethylbenzanthracene-induced mammary tumors in Sencar miceJ Steroid Biochem Mol Biol200597323024016153821
- MaglioneJEMcGoldrickETYoungLJPolyomavirus middle T-induced mammary intraepithelial neoplasia outgrowths: single origin, divergent evolution, and multiple outcomesMol Cancer Ther20043894195315299077
- MaglioneJEMoghanakiDYoungLJTransgenic polyoma middle-T mice model premalignant mammary diseaseCancer Res200161228298830511719463
- NambaRYoungLJMaglioneJESelective estrogen receptor modulators inhibit growth and progression of premalignant lesions in a mouse model of ductal carcinoma in situBreast Cancer Res200576R881R88916280035
- BurichRAMehtaNRWurzGTOspemifene and 4-hydroxyospemifene effectively prevent and treat breast cancer in the MTag.Tg transgenic mouse modelMenopause20121919610321926925
- GuyCTCardiffRDMullerWJInduction of mammary tumors by expression of polyomavirus middle T oncogene: a transgenic mouse model for metastatic diseaseMol Cell Biol19921239549611312220
- LinEYJonesJGLiPProgression to malignancy in the polyoma middle T oncoprotein mouse breast cancer model provides a reliable model for human diseasesAm J Pathol200316352113212614578209
- BurichRDeGregorioMCurrent treatment options for vulvovaginal atrophyExpert Rev Obstet Gynecol201162141151
- RozenbergSVandrommeJAntoineCPostmenopausal hormone therapy: risks and benefitsNat Rev Endocrinol20139421622723419265
- ChlebowskiRTAndersonGLGassMEstrogen plus progestin and breast cancer incidence and mortality in postmenopausal womenJAMA2010304151684169220959578
- IndhavivadhanaSLeerasiriPRattanachaiyanontMVaginal atrophy and sexual dysfunction in current users of systemic postmenopausal hormone therapyJ Med Assoc Thai201093666767520572371
- PastoreLMCarterRAHulkaBSWellsESelf-reported urogenital symptoms in postmenopausal women: Women’s Health InitiativeMaturitas200449429230315531125
- LabrieFCusanLGomezJLEffect of one-week treatment with vaginal estrogen preparations on serum estrogen levels in postmenopausal womenMenopause2009161303618820592
- BachmannGBobulaJMirkinSEffects of bazedoxifene/conjugated estrogens on quality of life in postmenopausal women with symptoms of vulvar/vaginal atrophyClimacteric201013213214019863455
- MirkinSKommBSTissue-selective estrogen complexes for postmenopausal womenMaturitas7102013 [Epub ahead of print.]
- BhavnaniBREstrogens and menopause: pharmacology of conjugated equine estrogens and their potential role in the prevention of neurodegenerative diseases such as Alzheimer’sJ Steroid Biochem Mol Biol2003852–547348212943738
- StovallDWAprela, a single tablet formulation of bazedoxifene and conjugated equine estrogens (Premarin) for the potential treatment of menopausal symptomsCurr Opin Investig Drugs2010114464471
- Osphena™ (ospemifene) prescribing informationFlorham Park, NJShionogi Inc2013 Available from: http://www.shionogi.com/pdf/PI/Osphena-PI.pdfAccessed August 22, 2013