
Abstract
Objective
To report a rare case of spontaneous ectopic pregnancy (EP) after partial salpingectomy treated by laparoscopy.
Case Report
A 30-year-old gravida 1 para 0 woman with a history of left adnexectomy, due to left ovarian torsion 13 years ago, was referred to our hospital. She had experienced lower abdominal pain for 1 day and amenorrhea for 1 week. Transvaginal ultrasonography did not reveal an intrauterine pregnancy, but showed a suspected extrauterine gestational sac on the left adnexal area. The patient was diagnosed with ectopic pregnancy, and laparoscopy was performed. During the operation, we found a gestational sac on the left fallopian tube stump.
Conclusion
The most significant risk factors for ectopic pregnancy (EP) are previous procedures and conditions that cause tubal injury. Therefore, it is necessary to be alert to the occurrence of the disease even if there is a history of tubal resection and ensure no part of the fallopian tube is left behind during removal.
Introduction
Ectopic pregnancy happens approximately 1.5–2.0% among all pregnancies, but accounts for 5–10% of all pregnancy-related deaths.Citation1,Citation2 Ninety-five percent of ectopic pregnancies occur in the fallopian tube, and approximately 2.5% of cases occur in the interstitial position.Citation3,Citation4 Approximately 10% of patients with ectopic pregnancies will experience a recurrent ectopic pregnancy.Citation5 Tubal stump pregnancy is rare, Ko et al reported that tubal stump pregnancy after tubectomy with a prevalence of about 0.4%.Citation4 Previous literature reports that tubal stump pregnancies are predominantly interstitial tubal pregnancies, often due to the patient having had an ectopic pregnancy and a subsequent salpingectomy.Citation6,Citation7 Some tubal stump pregnancies occur secondary to post-tubal ligation.Citation3,Citation8 We report a case of spontaneous tubal stump pregnancy after partial salpingectomy due to torsion of the left ovarian cyst pedicle.
Case Report
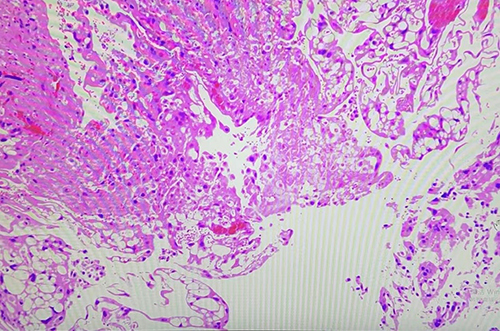
A 30-year-old gravida 1 para 0 woman with a history of left adnexectomy due to left ovarian torsion 13 years ago was referred to our hospital. She had experienced lower abdominal pain for 1 day and amenorrhea for 1 week. Her serum human chorionic gonadotropin (HCG) level was 2278 IU/L and a pelvic transvaginal ultrasound (TVUS) showed a heterogeneous echo (0.9 cm ×0.8 cm× 0.7 cm) near the left ovary ( and ). CDFI (Color Doppler Flow Imaging) indicates blood flow signal in ectopic pregnancy mass (). The clinical examination revealed abdominal pain with stable vital signs. The patient was suspected to have a left interstitial tubal pregnancy; thus, emergency laparoscopy was performed. At laparoscopy, there was no free blood in the pelvic cavity, and on the left salpingeal stump, an ectopic pregnancy was noted (). The uterus was of normal size, its surface was smooth, and no abnormalities were seen in the bilateral ovary morphologies. No obvious abnormalities were found in the right fallopian tube (). The left salpingeal stump tube was removed, and villous tissue was found in it (). The pelvic cavity was washed with saline solution, and the operation was ended. On the first day following the surgery, the patient’s HCG levels decreased to 662.1 IU/L. The blood HCG levels continued to decline, and the patient’s recovery proceeded without complications. The patient was discharged on the third postoperative day and received follow-up care in an outpatient setting. Histological analysis indicated the presence of trophoblastic tissues, confirming the diagnosis of an ectopic pregnancy ().
Figure 1 The ultrasound imaging demonstrates a mass at the residual segment of the left fallopian tube (isthmus) consistent with an ectopic pregnancy.
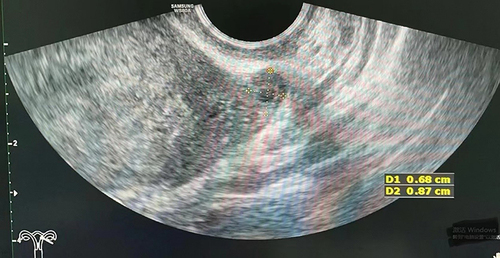
Figure 2 The size of the ectopic pregnancy mass in the left tubal remnant.
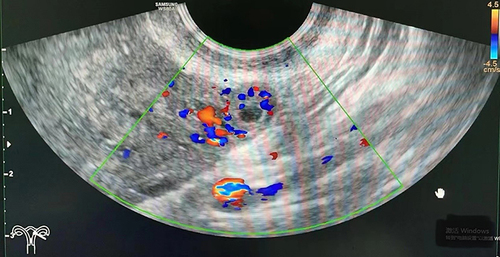
Figure 3 The blood flow pattern of the ectopic pregnancy mass.
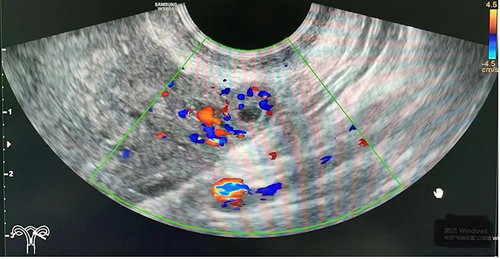
Figure 4 The pregnancy in the left tubal remnant was observed during laparoscopy.
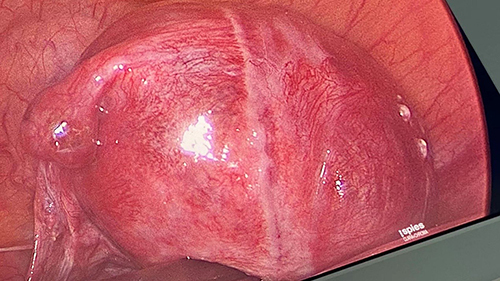
Figure 5 The right fallopian tube exhibits a normal appearance.
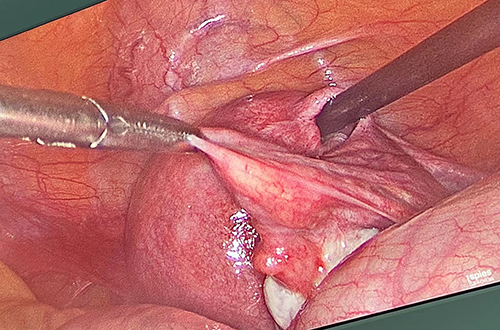
Figure 6 The villous tissue was present within the pregnancy sac of the left tubal remnant.

Figure 7 The pathological specimen confirmed chorionic villi (CV) within the ectopic pregnancy mass (haematoxylin and eosin stain, 200×magnification).
Discussion
Ectopic pregnancy (EP) poses a significant threat to the lives of women of childbearing age. In recent years, the incidence of EP has shown an increasing trend, attributed to factors such as delayed childbearing and the use of in vitro fertilization (IVF)-assisted fertility treatments. Notably, half of the patients diagnosed with ectopic pregnancy present with no known risk factors.Citation9 Previous surgery on the fallopian tubes or damage to the fallopian tubes constitutes risk factors for ectopic pregnancy (EP).Citation10 The rates of recurrent ectopic pregnancy following salpingectomy and salpingostomy are reported to be 5% and 8%, respectively.Citation11 Ectopic pregnancy can manifest in either the proximal or distal remnants of the operated fallopian tube. Drakopoulos P reported the inaugural case of an ectopic pregnancy occurring in the distal remnant following a laparoscopic partial segmental isthmic salpingectomy.Citation12 Subsequently, Lin CM and Xue Ke documented a rare instance of a left ampullary ectopic pregnancy subsequent to the ligation of the left fallopian tube.Citation3,Citation8 Both of these ectopic pregnancies occurred after resection of the ipsilateral proximal fallopian tube. In this case, distinct from the cases described in the literature above, the patient had previously undergone a left adnexectomy due to torsion of the pedicle of a left ovarian cyst, left part of the proximal fallopian tube tissue. Under the condition of an unobstructed contralateral fallopian tube, an ectopic pregnancy (EP) occurred in the stump of the fallopian tube previously partially removed, which is extremely rare. Notably, this was her first natural conception. In the existing literature, only one case resembling our description has been documented. However, that case was situated nearer to the interstitial segment of the fallopian tube and was characterized as a recurrent ectopic pregnancy within the fallopian tube.Citation13 This phenomenon can be explained by two theories.Citation14 The first theory suggests that a fertilized ovum could migrate from the intact right fallopian tube, across the endometrial cavity, to the proximal stump of the salpinx on the opposite side, a process known as internal migration of the fertilized ovum. The second theory posits that the ectopic pregnancy’s anatomical location may result from the transperitoneal migration of an ovum from the contralateral ovary to the opposite salpinx via the pouch of Douglas, with the early embryo subsequently being captured by the left distal tubal stump. This is called the theory of external migration.Citation13,Citation14 It is certain that even the fallopian tube stump still retains physiological function. As such, recurrent ectopic pregnancy is more likely following partial salpingectomy than total salpingectomy. To prevent ectopic pregnancy, complete excision of the affected fallopian tube is recommended. Furthermore, some scholarsCitation15 believe that sufficient diathermy of proximal fallopian tube or its ligation might be used to reduce the risk of re-implantation.
Conclusion
The etiology of ectopic pregnancies following salpingectomies remains uncertain, and they are clinically significant due to their potential to be overlooked and associated high mortality rates. Clinicians should be cognizant of the fact that ectopic pregnancies can present atypically, and it is especially important to remember that a salpingectomy does not completely preclude the diagnosis of an ectopic pregnancy. Since the fallopian tube stump still retains physiological function, complete removal during surgery is necessary.
Abbreviations
EP, ectopic pregnancy; REP, repeated ectopic pregnancy; HCG, human chorionic gonadotropin; TVUS, transvaginal ultrasound; IVF, in vitro fertilization.
Ethical Approval
The study was approved by the ethics committee of Hangzhou Women’s hospital (2023-A-181).
Declaration of Patient Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest in this work.
Acknowledgments
We would like to acknowledge our patient for consenting to the publication of this case report.
References
- Houser M, Kandalaft N, Khati NJ. Ectopic pregnancy: a resident’s guide to imaging findings and diagnostic pitfalls. Emerg Radiol. 2022;29(1):161–172. doi:10.1007/s10140-021-01974-7
- Jin XY, Li C, Xu W, Liu L, Wei ML. Factors associated with the incidence of ectopic pregnancy in women undergoing assisted reproductive treatment. Chin Med J. 2020;133(17):2054–2060. doi:10.1097/CM9.0000000000001058
- Ke X, He L, Zheng J-F, Lin Y-H, Wang F. Rare occurrence of left ampullary ectopic pregnancy after ligation of the left fallopian tube: a case report. Int J Women’s Health. 2023;4(15):965–970. doi:10.2147/IJWH.S417186
- Ko PC, Liang CC, Lo TS, Huang HY. Six cases of tubal stump pregnancy: complication of assisted reproductive technology? Fertil Steril. 2011;95(7):2432. doi:10.1016/j.fertnstert.2011.03.069
- Bouyer J, Coste J, Fernandez H, Pouly JL, Job-Spira N. Sites of ectopic pregnancy: a 10 year population-based study of 1800 cases. Hum Reprod. 2002;17(12):3224–3230. doi:10.1093/humrep/17.12.3224
- Horwood G, Warshafsky C, Singh SS. A cautionary tale of the tubal stump. J Minim Invasive Gynecol. 2023;30(5):344–345. doi:10.1016/j.jmig.2023.01.009
- Bernstein M, Han M. Laparoscopic management of short-interval interstitial pregnancy after recent tubal ectopic pregnancy: a case report. Case Rep Women’s Health. 2024;41:e00585. doi:10.1016/j.crwh.2024.e00585
- Lin CM, Ku YL, Cheng YT, Giin NY, Ou YC. An uncommon spontaneous right distal tubal pregnancy post bilateral laparoscopic sterilization: a case report. Medicine. 2019;98(4):e14193. doi:10.1097/MD.0000000000014193
- Hendriks E, Rosenberg R, Prine L. Ectopic pregnancy: diagnosis and management—American Family Physician. Am Fam Physician. 2020;101(10):599–606.
- Mullany K, Minneci M, Monjazeb R, Coiado OC. Overview of ectopic pregnancy diagnosis, management, and innovation. Women’s Health. 2023;19:17455057231160349. doi:10.1177/17455057231160349
- Mol F, van Mello NM, Strandell A, Strandell K, Jurkovic D. Salpingotomy versus salpingectomy in women with tubal pregnancy (ESEP study): an open-label, multicentre, randomized controlled trial. Lancet. 2014;383(9927):1483–1489. doi:10.1016/S0140-6736(14)60123-9
- Drakopoulos P, Julen O, Petignat P, et al. Spontaneous ectopic tubal pregnancy after laparoscopic tubal sterilization by segmental isthmic partial salpingectomy. BMJ Case Rep. 2014;2014:bcr-2013-203131. doi:10.1136/bcr-2013-203131
- Janbakhishov T, Dogan S, Dogan E. Laparoscopic treatment of recurrent ectopic pregnancy in the ipsilateral salpinx after ovulation induction and intrauterine insemination. Taiwanese J Obstetrics Gynecol. 2013;52(4):568–570. doi:10.1016/j.tjog.2013.10.020
- Banzai C, Matsumoto A, Higeta D, et al. A case of cornual pregnancy after ipsilateral salpingectomy for isthmic pregnancy. Gynecol Minim Invasive Ther. 2023;12(1):48–50. doi:10.4103/gmit.gmit_11_22
- Samiei-Sarir B, Diehm C. Recurrent ectopic pregnancy in the tubal remnant after salpingectomy. Case Rep Obstet Gynecol. 2013;2013:753269. doi:10.1155/2013/753269