
Abstract
Gestational diabetes mellitus (GDM) is associated with an increased risk of complications for both mother and baby during pregnancy as well as in the postpartum period. Screening and identifying these high-risk women is important to improve short- and long-term maternal and fetal outcomes. However, there is a lack of international uniformity in the approach to the screening and diagnosis of GDM. The main purpose of this review is to provide an update on screening for GDM and overt diabetes during pregnancy, and discuss the controversies in this field. We take on debatable issues such as adoption of the new International association of diabetes and pregnancy study groups criteria instead of the Carpenter and Coustan criteria, one-step versus two-step screening, universal screening versus high-risk screening before 24 weeks of gestation for overt diabetes, and, finally, the role of HbA1c as a screening test of GDM. This discussion is followed by a review of recommendations by professional bodies. Certain clinical situations, in which a pragmatic approach is needed, are highlighted to provide a comprehensive overview of the subject.
Introduction
Gestational diabetes mellitus (GDM) has classically been defined as any glucose intolerance first identified during pregnancy.Citation1 Recently, the American Diabetes Association (ADA) defined it as “Diabetes diagnosed in the second or third trimester of pregnancy that is not clearly overt diabetes”.Citation2 However, as per IADPSG (International association of diabetes and pregnancy study groups) criteria, women can be diagnosed to have GDM even in the first trimester, if fasting plasma glucose (FPG) is ≥5.1 mmol/L (92 mg/dL), but <7 mmol/L (126 mg/dL).Citation3
GDM is associated with an increased risk of complications for both mother and baby, during pregnancy as well as in the postpartum period. Screening and identifying these high-risk women is important to improve short and long-term maternal and fetal outcomes.Citation4 However, there is lack of international uniformity in the approach to the screening and diagnosis of GDM.Citation5 This is surprising, given that the strategies for making a diagnosis of diabetes mellitus are uniform across the world.Citation2 The main reason for the diagnostic dilemma of GDM is the large number of procedures and glucose cutoffs proposed for the diagnosis of glucose intolerance in pregnancy.Citation6 The first diagnostic criteria proposed by O’Sullivan in 1964 and its subsequent modifications (Carpenter and Coustan) were based on the maternal risk of developing type 2 diabetes, rather than on pregnancy outcomes. Recently, the recommendations from IADPSG attempt to redefine GDM in terms of adverse pregnancy outcomes, based on Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study results.Citation6 But, we are still far from attaining a holistic criteria which is based on both short and long-term outcomes.
The main purpose of this review is to provide an update on screening for GDM and overt diabetes during pregnancy, and discuss the controversies in this field. We take on debatable issues such as adoption of the new IADPSG criteria instead of the Carpenter and Coustan criteria, one-step versus two-step screening, universal screening versus high-risk screening before 24 weeks of gestation for overt diabetes, and, finally, the role of HbA1c as a screening test of GDM. This discussion is followed by a review of recommendations by professional bodies. Certain clinical situations, in which a pragmatic approach is needed, are highlighted to provide a comprehensive overview of the subject.
Evolution of screening criteria for GDM
The first systematic evaluation of the oral glucose tolerance test (OGTT) for the diagnosis of diabetes in pregnancy was done by O’Sullivan et al in the 1950s and 1960s. Since then, the 100-g OGTT has undergone extensive modifications, to its present form, that is, Carpenter and Coustan criteria (1982).Citation6,Citation7 Recently, IADPSG criteria have also come into the picture.Citation3
100-g OGTT
The original diagnostic criteria, based on blood glucose testing before and hourly for 3 hours after 100-g glucose intake for GDM, were proposed by O’Sullivan and Mahan in 1964,Citation8 based on a series of 752 women who underwent OGTTs during pregnancy. Means and standard deviations (SDs) were derived for each of four whole blood glucose values (defined as mean plus 1, 2, or 3 SD). O’Sullivan and Mahan decided that two abnormal values would be needed for GDM diagnosis. The decision was based upon the desire to avoid misclassification due to laboratory error or the occasional individual with a single high glucose peak due to rapid absorption. Approximately 2% of pregnant women fulfilled the criteria of mean plus 2 SD, and these criteria became the basis for the diagnosis of GDM in the USA. The diagnostic criteria were applied to a separate group of 1,013 women who underwent 100-g OGTTs during their pregnancy. The risk of subsequent diabetes was 27% after a follow-up period of 8 years, when values at 2 SD were used as the diagnostic threshold during pregnancy.Citation6–Citation8
In 1979, the National Diabetes Data Group criteria (NDDG) converted the whole blood glucose thresholds to the plasma values (approximately 14% higher as compared with the original O’Sullivan and Mahan criteria), in response to the general change in laboratory standards from whole blood to plasma or serum.Citation6,Citation9 Subsequently, new laboratory technology for glucose measurements using glucose oxidase and hexokinase methods, led to the formulation of the Carpenter and Coustan criteria.Citation6,Citation10 The original O’Sullivan and Mahan criteria were established using Somogyi–Nelson technology. The Somogyi–Nelson method is not specific for glucose, and also measures approximately 0.27 mmol/L (5 mg/dL) of nonglucose reducing substances. Glucose oxidase and hexokinase methods, on the other hand, measure only glucose. In 1982, Carpenter and Coustan used the glucose oxidase method to derive a set of criteria by first subtracting 5 mg/dL from O’Sullivan and Mahan’s original values and then adding 14% to each (to account for the conversion from whole blood to plasma glucose values), and, finally, rounding to the nearest 5 mg/dL (0.27 mmol/L). This formulated the Carpenter and Coustan criteria.Citation6,Citation7,Citation10
75-g OGTT
The initial recommendation for using 75-g OGTT in pregnancy was from the World Health Organization (WHO). The WHO used the same criteria for diagnosing diabetes both during and outside of pregnancy.Citation11 This approach was criticized, as it ignored the physiological changes in carbohydrate metabolism that occurs during pregnancy. In 1999, the WHOCitation11 lowered the threshold for FPG from 7.8 mmol/L (140 mg/dL) to 7.0 mmol/L (126 mg/dL) and recommended that pregnant women meeting the criteria for diabetes mellitus or impaired glucose tolerance (IGT) be classified as having GDM.
All these criteria had a common problem, namely, they were validated for predicting the future risk of diabetes only in the mother.Citation6–Citation10 A need was felt to derive new criteria linking level of glycemia to pregnancy and fetal outcomes. The current 75-g IADPSG criteria have been devised keeping this fact in mind and evaluating evidence that associates abnormal glucose tolerance in pregnancy with adverse perinatal outcomes.Citation3 Unblinded studies since 1995 have shown adverse perinatal outcomes to be linearly linked with glycemic levels in gestation.Citation5 The landmark study in this respect was the HAPO study.Citation12 The HAPO study was a large, multicenter, multinational, epidemiologic study in which 23,316 women (>30 times larger than the O’Sullivan cohort) underwent blinded 2-hour, three-sample, 75-g OGTTs at 24–32 weeks of gestation. All women with a fasting plasma glucose (FPG) ≤5.8 mmol/L (105 mg/dL) and 2 hours values up to 11.1 mmol/L (200 mg/dL) were included. The HAPO clearly established a linear relationship between each of the glucose values (fasting, 1 hour, and 2 hours) on OGTT and a broad range of predefined pregnancy outcomes. The primary outcomes in the HAPO study were the frequency of large-for-gestational-age (LGA, >90th centile) babies, primary cesarean section, clinical neonatal hypoglycemia, and neonatal hyperinsulinemia. All of these primary outcomes as well as secondary outcomes like fetal adiposity, preeclampsia, and birth trauma/shoulder dystocia were related to each of the maternal OGTT glucose results in a continuous fashion. The independent associations of hyperglycemia with pregnancy outcomes persisted after extensive adjustment for potential confounders including maternal body mass index (BMI), age, height, mean arterial pressure, and parity.Citation5,Citation12
In 2008, the IADPSG recommended the establishment of new diagnostic criteria for GDM based on data from the HAPO study. The diagnostic threshold would have to be somewhat arbitrary, because of the linear association between glycemic values and pregnancy outcomes. The diagnostic thresholds that were decided by the IADPSG consensus panel are based on glucose levels that give 75% increased risk of birth weight ≥90th centile, cord C peptide ≥90th centile, and percentage body fat ≥90th centile as compared with mean glucose levels of women of HAPO cohort. On this basis, the IADPSG recommended a fasting glucose level of 5.1 mmol/L (92 mg/dL), a 1-hour level of 10.0 mmol/L (180 mg/dL), or a 2-hour value of 8.5 mmol/L (153 mg/dL) as diagnostic for GDM.Citation3 The IADPSG criteria have been endorsed by WHO, ADA, and the Endocrine Society of USA.Citation2,Citation13,Citation14
Controversy: should IADPSG criteria be adopted universally?
The prevalence of GDM increases by two- to threefold if the IADPSG criterion is adopted for screening. There is an ongoing debate whether such an increase in prevalence allows identification of previously ignored risks, or results in overmedicalization of healthy pregnancies.Citation5,Citation15–Citation20 There is a need to closely look at arguments on both sides.
Arguments against adopting IADPSG criteria universally
Weak association of complications with glycemic levels
The lack of association between perinatal mortality and higher blood glucose levels, as observed in the HAPO study, has been used as a strong counterpoint by the detractors of the IADPSG criteria.Citation12,Citation16 The association between secondary endpoints (shoulder dystocia, premature delivery, hyperbilirubinemia, and preeclampsia) and glycemic levels was significant, but clinical relevance of this finding is limited as these complications are relatively infrequent. The association between maternal blood glucose and certain endpoints like neonatal hypoglycemia, birth weight, cesarean section rate, and preeclampsia either disappeared or became weak when maternal characteristics such as BMI were taken into account.Citation12,Citation16–Citation19
Increased rate of intervention and adverse effects
The diagnosis of GDM, irrespective of the degree of glucose control achieved, per se leads to increased interventions, earlier delivery, an increased cesarean section rate (even if birth weight is normalized by treatment), and a higher number of neonatal admissions to special care nurseries.Citation16,Citation17,Citation20 This phenomenon has been observed in the Australian Carbohydrate Intolerance Study in Pregnant Women (ACHOIS).Citation21 The basis for this finding is not entirely clear, but it may be related to the overcautious approach adopted by caregivers in pregnancies with diabetes. These complications may be more frequent in routine clinical settings, outside of controlled research settings.Citation16,Citation17
Lower diagnostic values will apparently lower target glucose values implying that more women will be treated with glucose-lowering therapy. This may increase the risk of maternal hypoglycemia and poor fetal growth, which in turn will contribute to metabolic disorders in adulthood. All these interventions create stress and anxiety among women diagnosed as having GDM.Citation16,Citation20
Evidence of no treatment benefit for mild GDM from RCTs
Two landmark randomized trials performed by Crowther et al (ACHOIS) and Landon et al (Maternal-Fetal Medicine Units, MFMU) influenced the recommendations for GDM diagnosis, by IADPSG.Citation21,Citation22 Analysts point out that these two trials were different from the HAPO study and should not have been considered along with it.Citation16,Citation17 The broad differences between them and the HAPO study are discussed here.
Trial design: These were intervention trials to investigate the effect of GDM treatment (diet and/or insulin) on perinatal outcomes, whereas the HAPO study was an observational study.
Inclusion/exclusion criteria: Unlike HAPO, where women irrespective of previous GDM were included, both studies excluded women with such a history.
Diagnostic criteria: Both studies used a two-step diagnostic procedure but with different diagnostic criteria. The criteria for the ACHOIS study were positive 50 g glucose challenge test (GCT) at 24–34 weeks’ gestation (≥7.8 mmol/L) and FPG ≤7.8 mmol/L and 2 hours value 7.8–11 mmol/L on 75-g OGTT. For the MFMU study, the criteria were positive 50 g GCT at 24–31 weeks’ gestation (7.5–11.1 mmol/L) and FPG ≤5.3 mmol/L and 2 or 3 postload levels elevated (1 hour >10.0; 2 hours >8.6; 3 hours >7.8 mmol/L) on 100-g OGTT. The MFMU study excluded women with FBG values >5.3 mmol/L (95 mg/dL), so the participants were less hyperglycemic than those of the ACHOIS cohort. The HAPO study used a single-step testing protocol without a prior GCT.
Outcomes: Both studies included perinatal mortality as a serious outcome, unlike in the HAPO study, in which perinatal mortality was not a part of the assessment. In the ACHOIS study,Citation21 the routine care group showed a higher prevalence (4% vs 1%) of composite primary outcome of “any serious perinatal complication.” However, some of the deaths could not plausibly be attributed to the non-treatment of GDM: for example, one infant had a lethal congenital anomaly, and another had severe intrauterine growth retardation. In the MFMU trial,Citation22 no difference was found between the groups in the composite primary outcome score.
Meta-analysis of treatment trials
A recent meta-analysis of the treatment RCTs (including, and dominated by, the ACHOIS and MFMU trials) concluded that the only pregnancy outcomes affected by lowering the threshold for detection and treatment of GDM are a reduction in macrosomia (odd ratio [OR] 0.38; 95% CI, 0.30–0.49), LGA infants (OR 0.48; 95% CI, 0.38–0.62), and the incidence of shoulder dystocia (OR 0.40; 95% CI, 0.21–0.75).Citation23 In summary, the intervention trials in GDM confirmed that treatment contributes to a 2%–3% reduction in birth weight, leading to a lower incidence of “big babies” and shoulder dystocia. Moreover, the risk–benefit ratio for treatment is debatable. The authors of the ACHOIS trial calculated an NNT (number-needed-to-treat) of 34 to prevent “any serious perinatal complication,” but an NNH (number-needed-to harm) of 11 for induction of labor or admission to neonatal nursery.Citation21
Arguments in favor of adopting IADPSG criteria universally
Experts in favor of IADPSG criteria argue that the National Institute of Health (NIH) panel’s report and other critiques have failed to address the issue of increasing prevalence of prediabetes and undiagnosed type 2 diabetes, outside pregnancy, in women of childbearing age.Citation16–Citation18,Citation24 Moreover, considering the metabolic milieu in pregnancy, the threshold for diagnosis of diabetes has to be lower and more stringent than for the general population. Given the NHANES prevalence estimates for impaired glucose metabolism reaching 30% in women of childbearing age, the two- to threefold increase in prevalence of GDM, using the IADPSG approach may actually represent the true picture.Citation24
Association of complications with glycemic levels
According to the investigators of the HAPO study, glycemia was more strongly associated with the primary study outcomes as compared with maternal BMI.Citation25,Citation26 The effects of these two variables on primary outcomes were additive, without a statistically significant interaction.Citation25 The consensus panel chose features of diabetic fetopathy, namely, the frequency of birth weight >90th centile, percent body fat >90th centile, and cord C peptide >90th centile for the determination of diagnostic glucose thresholds. These are key phenotypic features of babies directly related to the pathophysiology of GDM and may also link with future metabolic abnormalities in adulthood. The selected thresholds also identify an increased risk of more severe, though less frequent, adverse pregnancy outcomes.Citation27
Increase in adverse effects and interventions
IADPSG recommendations represent a well-reasoned consensus view as to the levels of glycemia that are “sufficient to merit identification and treatment.” These criteria, if thoughtfully implemented, will appropriately identify and allow treatment of the metabolic abnormalities of GDM. This will lead to well-established benefits, in terms of immediate pregnancy outcomes, and likely benefits, in terms of future maternal and offspring health.Citation5,Citation15
Evidence of treatment benefit for mild GDM from RCTs
Experts favoring the IADPSG criteria argue that there is a high degree of congruence in the results of these two trials (ACHOIS and MFMU),Citation21,Citation22 as discussed in detail here:
Glycemic threshold at entry: Despite different diagnostic criteria of the two trials, as compared with the HAPO study, the subjects recruited in all studies had glycemic values comparable to those in the HAPO study.Citation5,Citation12,Citation15,Citation21,Citation22 In the ACHOIS study, the FPG value was used only to exclude women, initially using FPG 7.8 mmol/L (140 mg/dL) and changing it later to 7.0 mmol/L (126 mg/dL) after a change in the WHO recommendations. Thus, it would have been possible for women with marked fasting hyperglycemia to be included in this trial. However, as this degree of fasting hyperglycemia is very uncommon in pregnancy when the 2-hour plasma glucose is <11.1 mmol/L (200 mg/dL), this criterion was rarely invoked.Citation15,Citation21 Landon et alCitation22 applied a much more stringent criterion, excluding women with FPG 5.3 mmol/L (95 mg/dL).
The mean FPG of 4.8 mmol/L (86 mg/dL) is similar in both ACHOIS and MFMU RCTs. The median 2-hour glucose of the ACHOIS cohort was actually close to the IADPSG recommended 2-hour diagnostic threshold, meaning that if this value alone were to be used for diagnosis, around 50% of these women, who benefited from intervention, would not have been diagnosed as having GDM.Citation15
Advantages of treatment of GDM: Both studies showed a reduction in complications with the identification and active treatment of mild GDM. This was seen in terms of mean birth weight, frequency of LGA,Citation21,Citation22 reduction in fat mass, and in the reduction of shoulder dystocia.Citation22 Hypertensive disorders of pregnancy (gestational hypertension and preeclampsia) were also substantially reduced by active GDM treatment.Citation21,Citation22 Maternal weight gain was lessened by active therapy.Citation21,Citation22 Induction of labor was increased by active treatment in the Crowther study,Citation21 but not in the Landon study.Citation22 The frequency of cesarean sections was unchanged in the ACHOIS study,Citation21 and reduced in the MFMU study.Citation22 A subsequent systematic review concluded that the observed reductions in LGA, shoulder dystocia, and preeclampsia are consistent across these and other available reports.Citation28 As for perinatal mortality, the HAPO study was not powered to detect a difference in perinatal mortality, and for ethical reasons, the protocol was designed to minimize the risk of perinatal mortality.
Consensus
The relationship between hyperglycemia and adverse pregnancy outcomes is well defined through a large volume of congruent observational epidemiologic data, which were also considered for IADPSG recommendations.
The major observational studies have generally been performed with a 75-g OGTT, without prior GCT. The results, in particular the associations with excess fetal growth and its complications and the risk of pregnancy hypertension, remain consistent despite varying methods of analysis. No study found a clear diagnostic threshold or “inflection point” for any glucose measure above which risk increased sharply. Therefore, any decision regarding threshold values for GDM diagnosis will, by definition, be arbitrary, based on an individual or consensus view of the level of risk that is “sufficient” to merit the GDM label. The underlying principles of the IADPSG consensus process were 1) that women with equivalent levels of glucose-associated risk should be classified in a similar manner, and 2) that glucose criteria should be standardized internationally.Citation27
Universal testing for hyperglycemia in pregnancy in first trimester
Pregnant women with overt diabetes and suboptimal blood glucose control in early pregnancy are at increased risk of having a fetus with congenital anomalies and are also at increased personal risk of worsening of diabetic retinopathy and nephropathy. Early diagnosis of previously undiscovered overt diabetes in a pregnant woman may allow for the rapid institution of therapy to mitigate these risks. As the frequency of obesity and T2DM in young adults is increasing worldwide, most guidelines now recommend screening for overt diabetes at the first prenatal visit, especially in high-risk groups.Citation2,Citation13,Citation14,Citation18,Citation19,Citation29
The cutoffs for tests, recommended to detect diabetes in early pregnancy are FPG: 126 mg/dL (7.0 mmol/L); random plasma glucose: 200 mg/dL (11.1 mmol/L); or HbA1c: 6.5% (47 mmol/mol), same as recommended for nonpregnant population.Citation3 However, the WHO does not consider HbA1c for the diagnosis of overt diabetes in pregnancy.Citation14 It is generally considered that there is not enough evidence to recommend the screening and treatment of GDM before 24 weeks of gestation,Citation30 and some professional organizations still recommend risk factor-based screening in the first trimester.Citation18,Citation19
IADPSG recommends that an FPG 92 mg/dL (5.1 mmol/L) in early pregnancy be classified as GDM.Citation3 This recommendation remains highly debatable as the figure is based on data extrapolated from the cutoff value used on the 75-g OGTT later in pregnancy. A recent evaluation of the FPG in the first prenatal visit to diagnose GDM in People’s Republic of China showed that an FPG level between 110 and 125 mg/dL (6.1–6.9 mmol/L) was a much better predictor of the development of GDM and that, for their population, an FPG level of 92 mg/dL (5.1 mmol/L) at the first prenatal visit could not be supported as the criterion for the diagnosis of GDM.Citation31
However, the recommendation of IADPSG for the diagnosis of overt diabetes is agreed upon even by the strong critics of the proposed criterion of IADPSG for the diagnosis of GDM.Citation16 Based on available evidence, universal screening for GDM has to be carried out after 24 weeks, without any doubt or controversy.Citation30 On the pragmatic side, it is worthwhile to test blood glucose in the first trimester to rule out overt diabetes.Citation13
Two-step screening: GCT followed by OGTT
In the two-step screening approach, a 50-g GCT is followed by a 100-g, 3-hour OGTT if warranted by the results from the GCT. The screening threshold for GDM in the United States of either 7.8 mmol/L (140 mg/dL) or 7.2 mmol/L (130 mg/dL) on the 50-g, 1-hour oral GCT is used. Those who screen positive are followed up by an oral 100-g glucose tolerance test (OGTT, in which four blood samples are drawn over a 3-hour period after a woman drinks 100 g of glucose solution). GDM is officially diagnosed with a positive result on two abnormal values on OGTT. The current diagnostic thresholds for the OGTT are: ≥5.3 mmol/L (95 mg/dL) (fasting); ≥10 mmol/L (180 mg/dL) (1 hour); ≥8.6 mmol/L (155 mg/dL) (2 hours); and ≥7.8 mmol/L (140 mg/dL) (3 hours). In the USA, the American College of Obstetricians and Gynecologists (ACOG) along with the NIH still promotes a two-step process with initial 50-g nonfasting GCT.Citation2
Arguments favoring two-step method
An advantage of the widely used two-step test (nonfasting 50 g glucose challenge, followed, if positive, by a fasting OGTT) is that women have to “fail” two tests to be diagnosed with GDM, so one can be more confident that indeed they have significant glucose intolerance. The proposed one-step test, while administratively more convenient, loses this discriminating power.Citation16 This concern has been raised in view of poor reproducibility of OGTT. As illustrated by studies that have looked at the results of women having two 100-g OGTTs at short intervals (with two elevated glucose results out of four required to diagnose GDM), nearly a quarter of women changed diagnostic category on the second test – with a similar number going from abnormal to normal as the other way round.Citation32,Citation33 Reliance on a single blood glucose result in a one-step screening test, especially using lower thresholds, will have even poorer precision. Moreover, first step by GCT has the advantage that it can be performed throughout the day without the need to be in fasting conditions.Citation19
Arguments opposing two-step method
Detractors opine that reproducibility was more of a problem with older methods of estimation of glucose, rather than with the current assays. The decision of diagnosis of GDM on the basis of two abnormal values in 100-g OGTT was also arbitrary. How GCT evolved and got incorporated into a two-step strategy is also a speculation, as it was not evidence based.Citation5
The two-step screening preceded by GCT followed by full OGTT inevitably delays the diagnosis of GDM and therefore treatment.Citation34 A systematic review compared the 50-g GCT and the OGTT (either 75 or 100 g) to estimate the sensitivity and specificity of the GCT for GDM.Citation35 For consecutively recruited patients, the pooled sensitivity was 0.74 for a specificity of 0.85, meaning that the process of performing GCT and then OGTT misses around 26% of potential GDM diagnoses.Citation35 At certain places, the figures may be even higher, as GCT screening misses many of those with GDM with a modestly elevated fasting glucose. Recent data from the HAPO study suggested that 63%–73% of cases in North American centers were diagnosed on the basis of an elevated fasting glucose level alone.Citation36 The other serious concern about using a GCT is the no-show rate for the definitive OGTT for women who are abnormal. In the Toronto Tri-Hospital Gestational Diabetes Project, 10% of women did not proceed with the GTT;Citation37 in a New Zealand study, the rate was 23%.Citation38 A recent North American report found that only 36% attended the OGTT.Citation39 The cost-effectiveness of two-step screening has to be weighed against inadvertent delay and missed diagnosis, and with their resultant potential maternal and fetal complications.Citation40
The result of GCT is influenced by the timing of meals, and that of testing. A recent study showed that among women with a positive GCT, those tested in the afternoon have better metabolic function and a lower risk of GDM on subsequent OGTT.Citation41 This suggests that the time of testing may lead to misclassification of patients with markedly elevated GCT results if GDM is diagnosed without confirmation by OGTT.
A recent prospective observational study randomized 786 pregnant women to screen for GDM either with a one-step method using a 75-g OGTT using IADPSG criteria (n=386) or with a two-step method with a 50-g GCT and a 100-g OGTT using the Carpenter and Coustan criteria (n=400), and then analyzed the prevalence of GDM using the one- and two-step methods. This study also aimed to determine whether women diagnosed as having normal glucose tolerance by the two-step method had any worse neonatal outcome than those determined to have normal glucose tolerance by the one-step method.Citation42 Women diagnosed with GDM by either process were treated according to the local management protocol including endocrinology review, glucose monitoring, dietary advice, and medication if required. The one-step method had a GDM prevalence of 14.5%, and the two-step method a prevalence of 6%. Women determined to have normal glucose tolerance in the two-step method had a greater risk of preeclampsia and macrosomia compared with the women defined as having normal glucose tolerance in the one-step method. On the basis of their study, authors strongly advocate elimination of the two-step process.
The advantages and disadvantages of the two-step and one-step screening protocol are summarized in .
Table 1 Advantages and disadvantages of two-step and one-step testing for GDM
Role of HbA1c in screening for gestational diabetes mellitus
Although the HbA1c reference intervals for the general population are well established, reference intervals for healthy pregnant women are not clearly defined.Citation43 A study in India showed that by using different ranges of HbA1c for the IADPSG criteria and the old ADA criteria, an OGTT could be avoided in approximately 40% (IADPSG) and 60% (ADA) of women, respectively.Citation44 However, the HAPO study showed that associations with adverse outcomes were significantly stronger with glucose measures than with HbA1c.Citation45
Different studies report different trends in HbA1c during pregnancy. Increase, decrease, and no change in HbA1c levels during pregnancy have been reported by different research groups.Citation43 Davies and WelbornCitation46 showed that mean HbA1c levels tend to rise after the first trimester of pregnancy in both normal and diabetic patients. This occurs despite the fact that FBG levels tend to fall in normal pregnancy, and in the diabetic patient, control of blood glucose levels improves with the progress of pregnancy. They proposed that some factor other than the level of glucose in the blood must be operating, since if HbA1c reflects only the average blood glucose level, it must fall with the progress of pregnancy. An explanation for this phenomenon is not clear. Pollak et alCitation47 indicated that HbA1c did not alter with the progress of pregnancy. Widness et alCitation48 found in a group of 13 nondiabetic women a significant fall in HbA1c from the first to the third trimester. McFarland et al also reported a decrease in HbA1c from the first half of pregnancy to the third trimester.Citation49
Altogether, the findings suggest that an HbA1c measurement is not a useful alternative to an OGTT in pregnant women.
Recommendations
Adoption of IADPSG criteria
The “IADPSG criteria” have been accepted by a variety of professional and other health care bodies including the Endocrine Society,Citation13 Australasian Diabetes in Pregnancy Society,Citation29 and WHO,Citation14 but challenged by others including the NIH consensus panel and the ACOG.Citation18,Citation19 The ADA has recommended that any one of them could be used for the diagnosis of GDM.Citation2
Universal screening for overt diabetes in pregnancy
IADPSG recommends opportunistic screening of pregnant women for preexisting diabetes at the first antenatal visit either universally in all women or in high-risk ones. The decision is being left to the discretion of the treating physician/obstetrician. The Endocrine Society Guidelines recommend testing all pregnant women, using the same diagnostic cutoffs that are recommended in the nonpregnant population,Citation13 whereas the ADA recommends testing women with risk factors for diabetes.Citation2 The WHO have adopted the entire IADPSG recommendation except the adoption of HbA1c as a diagnostic tool for diabetes in pregnancy.Citation14 However, all women with significant risk factors must be screened for unrecognized type 2 diabetes in early pregnancy. NIH and ACOG advocate risk factor-based screening before 24 weeks of gestation.Citation18,Citation19 The Australasian Diabetes in Pregnancy Society (ADIPS) recommends risk factor-based screening at the first antenatal visit.Citation29 Women with high-risk ethnicity or a BMI of 25–35 kg/m2 as their only risk factor are considered to be at “moderate risk” and should initially be screened with either a random or an FPG test. This may be followed by a 75-g OGTT (IADPSG criteria) if clinically indicated. Overweight or obese women from high-risk ethnicity should be evaluated by OGTT. OGTT is recommended at the first opportunity after conception for women having any of the high-risk factors for GDM listed in .Citation49
Table 2 High-risk factors for gestational diabetes mellitus
Two-step versus one-step testing
The ACOG and an independent expert panel assigned by the NIH continue to promote the use of the two-step screening strategy with the nonfasting 50-g GCT and if abnormal, followed by the 3-hour 100-g OGTT using the Carpenter and Coustan criteria or the NDDG criteria.Citation18,Citation19 Recently, both the WHO and the Endocrine Society have advocated the use of the IADPSG criteria for the diagnosis of GDM.Citation13,Citation14 ADIPS also advocates one-step testing.Citation29 The 2015 ADA recommendations specify that further research is needed to establish a uniform approach to diagnosing GDM, and now left the option open between the one-step IADPSG recommendation and the two-step screening strategy.Citation2
HbA1c in screening for gestational diabetes mellitus
HbA1c is not recommended for screening of GDM by any of the guidelines.Citation2,Citation13,Citation14,Citation18,Citation19,Citation29 This may be due to scarce data on this aspect. Physiological changes in red cell mass and turnover occurring during pregnancy also make interpretation of HbA1c in relation to glycemic levels difficult in pregnancy.Citation43 However, HbA1c is recommended by IADPSG to rule out overt diabetes in the first trimester.Citation3
The recommendations on various aspects of screening are summarized in .
Table 3 Recommendations on various aspects of screening
Pragmatic approach
Screening for GDM is an essential part of obstetric care. The only controversy is how to screen for the condition. The first diagnostic criterion proposed by O’Sullivan in 1964 and its subsequent modifications (Carpenter and Coustan) were based on the maternal risk of developing type 2 diabetes, rather than on neonatal outcomes. IADPSG, in contrast, attempts to redefine GDM in terms of neonatal and short-term maternal outcomes. But we are still far from attaining a holistic criterion based on both short- and long-term outcomes. Criteria based on the maternal risk of developing type 2 diabetes would appear to underdiagnose; whereas those based on only short-term outcomes may over diagnose GDM. A decision tree that balances neonatal outcome concern with maternal outcome and risk from treatment would seem to be the way forward, eventually. This requires more studies and data, of course.
Even though the IADPSG criteria aim to improve the perinatal outcomes, it may not be practical or feasible for every country/center to adopt it universally. As per the WHO, each health care facility needs to assess their burden of hyperglycemia in pregnancy and decide whether and how it will implement programs to test for and treat such women.Citation50 The WHO have proposed further strategies to overcome barriers of OGTT testing with compromise on missing some cases of GDM.Citation50 But again, the suggestions are made on the basis of limited studies, and the applicability of the results of one study needs to be evaluated in the indigenous population before a particular strategy is adopted. While developed health care practices may follow a two-step method, a one-step approach may be more useful for situations where access or travel to health care centers is limited or arduous. The benefits of a second test, performed in a second visit, must be balanced against the cost and inconvenience of travel. Travel is also associated with health risks. However, if GCT is accomplished on routine antenatal visit, then a two-step strategy may be beneficial in such cases.Citation5 The universal screening to rule out overt diabetes should, however, be adopted in ethnicities/countries with a high prevalence of diabetes.Citation13 We summarize the pragmatic indications for the one- and two-step approaches on the basis of a biopsychosocial model in and an overall pragmatic approach based on guidance from various professional bodies in .
Figure 1 Pragmatic approach to screen women for overt diabetes and GDM.
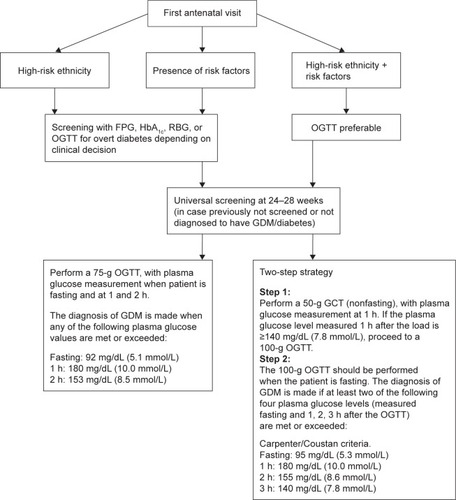
Table 4 Pragmatic indications for one- and two-step approaches based on biopsychosocial model
Future directions
It is felt that most guidelines fail to address the need and constraints of low-resource settings, where the demand for clear and simple directions is the greatest. The screening protocols are often based on evidence from scientific research carried out by well-resourced academic institutions. However, the typical clinical settings in low- and middle-income countries with poor resources and high disease burden face conditions that are often far away from these ideal settings. This calls into question the feasibility of applying screening procedures and diagnostic criteria. Future studies need to address these issues in great detail.Citation50 Data on the preference of pregnant women for a particular diagnostic test are unavailable. Future studies should also evaluate the impact of any strategy on personal satisfaction, quality of life, or psychological aspects of individual patients. Patient preferences, convenience of testing versus outcome of testing and treatment should also be taken into account. This is indeed an important future research imperative as without patient compliance, evidence-based screening decisions are useless. As per our clinical experience and that of other experts, pregnant women are more concerned about the outcome of their pregnancy than by the relatively minor inconveniences of diagnostic testing, GDM labeling and possible treatment of limited duration.Citation14
The NIH consensus panel identifies as a priority the conduct of a new RCT evaluating outcomes in women currently classified as “normal” according to prevalent US criteria but who would be considered abnormal by the IADPSG and the ADA.Citation18 The diagnosis of GDM is generally made in the late second or early third trimester. Early detection and treatment may potentially improve outcomes. However, there is a dearth of evidence in this area. Well-designed studies are needed to determine the most appropriate means of testing for GDM in early pregnancy and to explore the outcomes of early treatment interventions.
The adoption of IADPSG criteria by some professional organizations is mainly due to potential benefits (to mother and child) in the prevention of short-term pregnancies and perinatal outcomes. Data on potential long-term benefits to the health of the mother and her offspring are still scarce. Future studies and/or follow-up of previous cohorts like the HAPO study could answer this question.Citation14
Summary
Apart from the debate on other issues, the first step should be the implementation of universal screening to identify more severe cases of GDM. This step will already be a major one in most countries. The different viewpoints from experts and guidelines underscore the fact that there are data to support each strategy (IADPSG vs Carpenter and Coustan criteria; one-step vs two-step screening). The decision on which strategy to implement must therefore be made on the basis of the relative role of cost considerations, and availability of infrastructure locally, nationally, and internationally. In addition, patient preferences should be taken into account as part of any screening strategy.
Disclosure
The authors report no conflicts of interest in this work.
References
- American Diabetic AssociationDiagnosis and classification of diabetes mellitusDiabetes Care200629Suppl 1S43S4816373932
- American Diabetic AssociationClassification and diagnosis of diabetes mellitusDiabetes Care201538Suppl 1S8S1625537714
- International Association of Diabetes and Pregnancy Study Groups Consensus PanelMetzgerBEGabbeSGPerssonBInternational association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancyDiabetes Care201033367668220190296
- BuchananTAXiangAHPageKAGestational diabetes mellitus: risks and management during and after pregnancyNat Rev Endocrinol201281163964922751341
- McIntyreHDColagiuriSRoglicGHodMDiagnosis of GDM: a suggested consensusBest Pract Res Clin Obstet Gynaecol201529219420510.1016/j.bpobgyn.2014.04.02225242583
- HoushmandAJensenDMMathiesenERDammPEvolution of diagnostic criteria for gestational diabetes mellitusActa Obstet Gynecol Scand201392773974523600679
- CoustanDRDiagnosis of gestational diabetesScand J Clin Lab Invest Suppl2014244273325083890
- O’SullivanJBMahanCMCriteria for the oral glucose tolerance test in pregnancyDiabetes19641327828514166677
- National Diabetes Data GroupClassification and diagnosis of diabetes mellitus and other categories of glucose intoleranceDiabetes1979281210391057510803
- CarpenterMWCoustanDRCriteria for screening tests for gestational diabetesAm J Obstet Gynecol198214477687737148898
- World Health OrganizationDefinition, Diagnosis and Classification of Diabetes Mellitus and its Complications: Report of a WHO Consultation Part 1: Diagnosis and Classification of Diabetes MellitusWHO/NCD/NCS/992nd edGeneva, SwitzerlandWorld Health Organization1999
- HAPO Study Cooperative Research GroupMetzgerBELoweLPDyerARHyperglycemia and adverse pregnancy outcomesN Engl J Med2008358191991200218463375
- BlumerIHadarEHaddenDRDiabetes and pregnancy: an endocrine society clinical practice guidelineJ Clin Endocrinol Metab201398114227424924194617
- World Health OrganizationDiagnostic criteria and classification of hyperglycaemia first detected in pregnancyDiabetes Res Clin Pract2014103334136324847517
- McIntyreHDMetzgerBECoustanDRCounterpoint: establishing consensus in the diagnosis of GDM following the HAPO studyCurr Diab Rep201414649724777652
- LongHCundyTEstablishing consensus in the diagnosis of gestational diabetes following HAPO: where do we stand?Curr Diab Rep2013131435023054748
- RyanEADiagnosing gestational diabetesDiabetologia201154348048621203743
- National Institutes of Health Consensus Development Conference PanelNational Institutes of Health consensus development conference statement: diagnosing gestational diabetes mellitus, March 4–6, 2013Obstet Gynecol20131222 Pt 135836923969806
- Committee on Practice Bulletins – ObstetricsPractice Bulletin No 137: gestational diabetes mellitusObstet Gynecol20131222 Pt 140641623969827
- LongHDiagnosing gestational diabetes: can expert opinions replace scientific evidence?Diabetologia20115492211221321710287
- CrowtherCAHillerJEMossJRMcPheeAJJeffriesWSRobinsonJSEffect of treatment of gestational diabetes mellitus on pregnancy outcomesN Engl J Med2005352242477248615951574
- LandonMBSpongCYThomEA multicenter, randomized trial of treatment for mild gestational diabetesN Engl J Med2009361141339134819797280
- HorvathKKochKJeitlerKEffects of treatment in women with gestational diabetes mellitus: systemic review and meta-analysisBMJ2010340c139520360215
- McIntyreHDDiagnosing gestational diabetes mellitus: rationed or rationally related to risk?Diabetes Care201336102879288024065840
- CatalanoPMMcIntyreHDCruickshankJKThe Hyperglycemia and Adverse Pregnancy Outcome Study: associations of GDM and obesity with pregnancy outcomesDiabetes Care201235478078622357187
- HAPO Study Cooperative Research GroupHyperglycaemia and Adverse Pregnancy Outcome (HAPO) Study: associations with maternal body mass indexBJOG2010117557558420089115
- International Association of Diabetes and Pregnancy Study Groups (IADPSG) Consensus Panel Writing Group and the Hyperglycemia and Adverse Pregnancy Outcome (HAPO) Study Steering CommitteeMetzgerBEGabbeSGPerssonBThe diagnosis of gestational diabetes mellitus: new paradigms or status quo?J Matern Fetal Neonatal Med201225122564256922876884
- FalavignaMSchmidtMITrujilloJEffectiveness of gestational diabetes treatment: a systematic review with quality of evidence assessmentDiabetes Res Clin Pract2012983396e40523031412
- Australasian Diabetes In Pregnancy Society (ADIPS) Consensus Guidelines for the Testing and Diagnosis of Gestational Diabetes Mellitus in Australia Available from: http://www.bhs.org.au/airapps/Services/au/org/bhs/govdoc/files/references/14440.pdfAccessed January 27, 2015
- DonovanLHartlingLMuiseMGuthrieAVandermeerBDrydenDMScreening tests for gestational diabetes: a systematic review for the US Preventive Services Task ForceAnn Intern Med2013159211512223712349
- ZhuWWYangHXWeiYMEvaluation of the value of fasting plasma glucose in the first prenatal visit to diagnose gestational diabetes mellitus in chinaDiabetes Care201336358659023193214
- HarlassFEBradyKReadJAReproducibility of the oral glucose tolerance test in pregnancyAm J Obstet Gynecol199116425645681992702
- CatalanoPMDragoNMAminiSBReproducibility of the oral glucose tolerance test in pregnant womenAm J Obstet Gynecol199316948748818238142
- MosesRGCheungNWPoint: universal screening for gestational diabetes mellitusDiabetes Care20093271349135119564479
- van LeeuwenMLouwerseMDOpmeerBCGlucose challenge test for detecting gestational diabetes mellitus: a systematic reviewBJOG20121194393e40122260369
- SacksDAHaddenDRMareshMFrequency of gestational diabetes mellitus based on IADPSG consensus panel – recommended criteria at collaborating centersDiabetes Care201235352652822355019
- SermerMNaylorCDGareDJImpact of increasing carbohydrate intolerance on maternal-fetal outcomes in 3637 women without gestational diabetes. The Toronto Tri-Hospital Gestational Diabetes ProjectAm J Obstet Gynecol199517311461567631672
- YapaMSimmonsDScreening for gestational diabetes mellitus in a multiethnic population in New ZealandDiabetes Res Clin Pract200048321722310802161
- SievenpiperJLMcDonaldSDGreyVDon-WauchopeACMissed follow-up opportunities using a two-step screening approach for gestational diabetesDiabetes Res Clin Pract2012962e43e4622349298
- SimmonsDMosesRGGestational diabetes mellitus: to screen or not to screen? Is this really still a question?Diabetes Care201336102877287824065839
- GoldbergRJYeCSermerMCircadian variation in the response to the glucose challenge test in pregnancy: implications for screening for gestational diabetes mellitusDiabetes Care20123571578158422723584
- SevketOAtesSUysalOMollaTDansukRKelekciSTo evaluate the prevalence and clinical outcomes using a one-step method versus a two-step method to screen gestational diabetes mellitusJ Matern Fetal Neonatal Med2014271364123617557
- RafatDAhmadJHbA1c in pregnancyDiabetes Metab Syndr201261596423014257
- RaiputRYadavYRaiputMUtility of HbA1c for diagnosis of gestational diabetes mellitusDiabetes Res Clin Pract201298110410722456454
- LowePMetzgerBEDyerARHyperglycemia and Adverse Pregnancy Outcome (HAPO) Study: associations of maternal A1C and glucose with pregnancy outcomesDiabetes Care201235357458022301123
- DaviesDMWelbornTAGlycosylated haemoglobin in pregnancyAust N Z J Obstet Gynaecol19802031471506936014
- PollakAWidnessJASchwartzRMinor hemoglobins: an alternative approach for evaluating glucose control in pregnancyBiol Neonate1979363–4185192486609
- WidnessJASchwartzHCKahnCBOhWSchwartzRGlycohemoglobin in diabetic pregnancy: a sequential studyAm J Obstet Gynecol19801368102410296768294
- McFarlandKFCatalanoEWKeilJEMcFarlandDEGlycosylated haemoglobin in diabetic and nondiabetic pregnanciesSouth Med J19817444104126164102
- ColagiuriSFalavignaMAgarwalMMStrategies for implementing the WHO diagnostic criteria and classification of hyperglycaemia first detected in pregnancyDiabetes Res Clin Pract2014103336437224731475