
Abstract
Caustic ingestion is a common cause of life-threatening upper gastrointestinal tract injuries. It mostly happens in children as accidental exposure, but may occur in adults as a result of suicide attempt. We present a case of an acute abdomen that occurred after a peculiar way of self-administration of sulfuric acid as a suicide attempt in an adult psychiatric male patient, already known for self-harm with caustic agents in the previous years. In a few hours, the patient developed diffuse peritonitis, pneumoperitoneum, and a rapid hemodynamic deterioration, as a consequence of ileum and sigmoid necrosis, requiring an emergency surgery with the application of a damage control strategy. The patient was then transferred to intensive care unit for hemodynamic stabilization, and definitive surgical correction of the abdominal lesions was performed after 3 days with Hartmann procedure. Thirty-nine days after hospital admission, the patient was discharged. In conclusion, to our knowledge, never has been reported in the literature a case of intra-abdominal self-administration of caustic substance causing a rapid evolution of clinical conditions and requiring the application of damage control strategy.
Introduction
Worldwide, caustic injuries mostly occur in pediatric patients, as it is estimated that 80% of cases are accidental ingestion of household cleaning products in children.Citation1–Citation3
Caustic agents poisoning among adults is less frequent and is commonly intentional rather than accidental, as suicidal attempts by ingestion, that causes serious damage to oral mucous membrane, lips, and tongue, as well as esophagus and stomach.Citation4–Citation6
Most of the cases in which the intent is to commit suicide include teens and young adults in their 20s, and psychiatric and alcoholic patients.Citation7,Citation8
We present a peculiar case of caustic poisoning in an adult psychiatric male patient who deliberately self-administered an intra-abdominal injection of concentrated sulfuric acid for suicidal purposes, thus developing diffuse peritonitis and subsequently had to be surgically treated and admitted to our intensive care unit.
The publication of this clinical case report was approved by the Institutional Review Board of the University Hospital “Riuniti” of Foggia. Upon discharge from the psychiatric ward, the patient and his family reviewed the case report and gave written informed consent to publish the report.
Case description
A 37-year-old man was evaluated in the emergency department of the University Hospital of Foggia, Italy, for a suicide attempt by intra-abdominal injection of a caustic agent under the influence of drugs. The patient had a medical history of psychiatric disorder and drug abuse. This event was preceded 3 years before by deliberate ingestion of a household chemical (hydrochloric acid) with the intent of committing suicide. The patient underwent total gastrectomy, subtotal esophagectomy, and reconstruction of the jejunum.
At arrival, the patient was fully conscious, agitated, and complained of abdominal pain. Initial evaluation by the emergency room physician revealed mild tachypnea (respiratory rate of 22 breaths/min), saturation of 98% under room air, 100/60 mmHg arterial blood pressure, heart rate of 98 beats per minute, and 36.5°C body temperature.
Initial blood gas analysis showed pH 7.19, bicarbonate levels 13.4 mEq/L, PaCO2 level 35 mmHg, and anion gap of 26 mEq/L, so bicarbonate infusion was started while the patient was transferred to the emergency surgery department for further evaluation. The remaining initial biochemistry showed normal values, except for positive tests for cocaine and benzodiazepines.
On physical examination, the patient presented clear signs of acute abdomen with three visible different injection sites: left iliac fossa, mesogastrium, and hypogastrium.
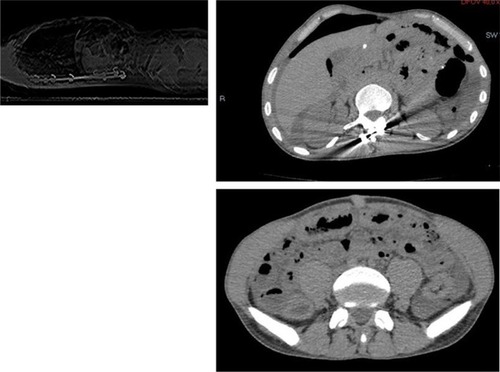
Computerized tomography scan showed “marked pneumoperitoneum and discreet intra-abdominal free fluid, more significant in the upper quadrants with air–fluid level in the right upper quadrant” ().
Figure 1 Computerized tomography scan showing the presence of marked pneumoperitoneum and discreet intra-abdominal free fluid, more evident in the upper quadrants, with air–fluid level in the right upper quadrant.
Due to hemodynamic deterioration (blood pressure 70/40 mmHg, heart rate 130 beats per minute), the patient underwent emergency surgery of a damage control laparotomy: ileal and sigmoid resection was performed due to widespread peritonitis and necrosis of the ileum and sigmoid.
On arrival at the operating room, the anesthesiologist placed two peripheral intravenous catheters and a radial catheter for continuous blood pressure monitoring and blood gas analyses. During the procedure, heated intravenous fluids, two fresh frozen plasma, and one pack red blood cell units were infused in order to manage intraoperative anemia (hematocrit 21% and hemoglobin 7 g/dL) and a contextual alteration of coagulation as documented by viscoelastic test executed during surgery. Furthermore, a warming mattress was positioned to prevent hypothermia.
Upon arrival of the patient at intensive care, the treatment focused on normothermia, tissue perfusion, appropriate values of hemoglobin (target 70–90 g/L Hb), and coagulation profile maintenance (prothrombin time/partial thromboplastin time <1.5 normal; fibrinogen >1.5–2.0 g/L) while monitoring intra-abdominal pressure (intravesicular pressure monitoring) to prevent abdominal compartment syndrome.
Definitive surgical correction of the lesions was performed at day 3 from the self-harming event: the “second look” consisted in peritoneal toilet, ileal recanalization, and terminal colostomy (Hartmann procedure).
Histology confirmed coagulative necrosis of examined tissues, full thickness, much more represented on the serosa than the mucosa, with thrombosis of small vessels, the presence of granulation tissue, hyperemic mucositis and, in some sections, mucosal discoloration.
The patient was discharged from the intensive care unit on day 6 and transferred to emergency surgery department since intensive treatment was no longer required.
Twenty-five days after admission, the patient was transferred to the psychiatric ward and then discharged after another 2 weeks of hospitalization.
Discussion
This is, to our knowledge, the first report of intra-abdominal injections of sulfuric acid.
Sulfuric acid is a colorless, odorless oily liquid; it is soluble in water with release of heat. It is highly corrosive to metals and tissues and is widely used as toilet bowl and drain cleaner.
In the literature, few cases of sulfuric acid drain cleaner ingestion and its consequences are described.Citation5
Caustic agent ingestion can cause severe damage to oral mucous membrane, lips, and tongue, and, above all, to the esophagus and stomach.Citation9–Citation11
The most common caustic-related injury due to ingestion of chemical agents is corrosive esophagitis; in the US, ingestion of acid substances responsible for caustic injury is less frequently reported than the ingestion of alkaline agents,Citation1 such as detergents, cleaning products, and bleaches. On the other hand, the corrosive esophagitis acidic-agent related is characterized by higher rates of complications, such as stricture and perforation, in comparison with alkaline-agent ingestion.Citation11
Alkaline agents cause liquefaction necrosis, which, in a short span of time leads to mucosal destruction, and in 1 or 2 days, the damage caused to the mucosa is exacerbated by thrombosis of small vessels. The lytic action on tissues is particularly destructive.Citation12 Acidic agents, in contrast, cause coagulation necrosis with eschar formation and, in some cases, limited tissue penetration.Citation1
The intensity of destruction depends on various factors: type, concentration, time of contact, and amount of the ingested substance.Citation9,Citation13
In contrast to children, whose poisoning is mainly accidental, a suicide attempt is the usual cause of caustic ingestion in adults, especially among teens, and psychiatric and alcoholic patients.Citation7,Citation8
While in Western countries alkaline agents are responsible for the majority of caustic-related injuries, ingestion of acidic agents is more common in India due to the wider availability among lower socio-economic groups.Citation12–Citation14
Our patient had already attempted suicide 3 years ago by ingesting hydrochloric acid, which resulted in total gastrectomy and subtotal esophagectomy due to necrosis of the stomach and distal esophagus, and had undergone subsequent surgical reconstruction.
The patient, while undergoing psychiatric treatment for his bipolar disorder, attempted suicide again, and the way of self-administration of the caustic is peculiar and never mentioned in the literature: intra-abdominal injection of concentrated sulfuric acid, an easily available cleaning product.
While the caustic ingestion first causes damage on the mucous membrane of the gastrointestinal tract and thereafter perforation may occur, in our patient’s particular way of administration led to immediate coagulation necrosis of the intestinal peritoneum, with widespread peritonitis and intestinal necrosis. The acute abdomen required emergent surgical treatment, which consisted of a damage control laparotomy,Citation15 followed by recovery in the intensive care unit and then a second surgery for definitive damage correction.
The strategy of the damage control laparotomy is applied to patients with severely impaired physiological reserve induced by the trauma. The rationale of the strategy is to quickly check the conditions at risk for survival, perform an abbreviated laparotomy to control the gastrointestinal damage, and delay the definitive correction of the lesions while the patient is admitted and treated in intensive care; only when the lethal triad of hypothermia, metabolic acidosis, and coagulopathy is corrected, the patient may subsequently undergo definitive surgery.Citation15,Citation16
Along with the surgical strategy of temporization, damage control resuscitation had to be applied to limit the physiological derangement of the patient due to both caustic injury and surgery itself.Citation16,Citation17
The treatment focused on normothermia, tissue perfusion, appropriate values of hemoglobin, and coagulation profile maintenance while monitoring intra-abdominal pressure to prevent abdominal compartment syndrome. Physiological and biochemical stabilization was achieved by appropriate vital signs monitoring, frequent blood tests to evaluate organ functions, mechanical ventilation, hemodynamic monitoring, and electrolyte and acid–base balance correction.
In conclusion, this case is paradigmatic of the importance of cooperation between the different figures involved: the emergency room physician, the toxicologist, the surgeon, the anesthesiologist, the resuscitator; their prompt coordination allowed rescue of the patient and the successful outcome.
Disclosure
The authors report no conflicts of interest in this work.
References
- RamasamyKGumasteVVCorrosive ingestion in adultsJ Clin Gastroenterol200337211912412869880
- BeirensTMvan BeeckEFDekkerRBrugJRaatHUnsafe storage of poisons in homes with toddlersAccid Anal Prev200638477277616545327
- McKenzieLBAhirNStolzUNelsonNGHousehold cleaning product-related injuries treated in US emergency departments in 1990–2006Pediatrics2010126350951620679298
- GoldmanLPWeigertJMCorrosive substance ingestion: a reviewAm J Gastroenterol198479285906364797
- MatshesEWTaylorKARaoVJSulfuric acid injuryAm J Forensic Med Pathol200829434034519259022
- ParkKSEvaluation and management of caustic injuries from ingestion of acid or alkaline substancesClin Endos2014474301307
- WuMHLaiWWEsophageal reconstruction for esophageal strictures or resection after corrosive injuryAnn Thorac Surg19925357988021570973
- RollinMJaulimAVazFSandhuGWoodSBirchallMDawasKCaustic ingestion injury of the upper aerodigestive tract in adultsAnn R Coll Surg Engl201597430430726263940
- MamedeRCde Mello FilhoFVIngestion of caustic substances and its complicationsSao Paulo Med J20011191101511175619
- GuptaSKRanaASGuptaDJainGKalraPUnusual presentation of caustic ingestion and its surgical treatment: a case reportJ Maxillofac Oral Surg2011101747622379326
- PoleyJWSteyerbergEWKuipersEJIngestion of acid and alkaline agents: outcome and prognostic value of early upper endoscopyGastrointest Endosc200460337237715332026
- RajabiMTMaddahGBagheriRMehrabiMShabahangHLorestaniFCorrosive injury of the upper gastrointestinal tract: review of surgical management and outcome in 14 adult casesIran J Otorhinolaryngol20152778152125745607
- LahotiDBroorSLCorrosive injury to the upper gastrointestinal tractIndian J Gastroenterol19931241351418270293
- HughTBKellyMDCorrosive ingestion and the surgeonJ Am Coll Surg1999189550852210549740
- LeeJCPeitzmanABDamage-control laparotomyCurr Opin Crit Care200612434635016810046
- MidwinterMJDamage control surgery in the era of damage control resuscitationJ R Army Med Corps2009155432332620397611
- LambCMMacGoeyPNavarroAPBrooksAJDamage control surgery in the era of damage control resuscitationBr J Anaesth2014113224224925038156