
Abstract
Introduction
Tuberculosis (TB) is one of the endemic diseases with a challenging diagnosis in the absence of pulmonary disease. On the other hand, rheumatoid arthritis (RA) is a systemic autoimmune disease with extra-articular manifestations that occur at any age after onset, such as nodules, Sjögren’s syndrome, anemia of chronic disease, and pulmonary manifestations, which are more frequently seen in patients with severe, active disease. Here we present a case of RA with intestinal TB.
Case report
A 55-year-old woman with a 30-year history of RA using prednisolone and hydroxychloroquine presented with a nonpositional hypogastric pain and a weight loss of 20 kg over 7 months. No history of biological therapy was recorded. Colonoscopy revealed an ulcerated mass that was suspicious for malignancy. The pathobiological assessments confirmed ulceration and granulation tissue formation, foci of necrotizing granulomatous inflammation in lamina propria with adjacent mild crypt regenerative changes. Also, Ziehl–Neelsen staining for acid-fast bacilli in the granulomas was positive though the polymerase chain reaction assay did not detect the Mycobacterium tuberculosis. Anti-TB medication for 2 weeks eliminated the symptoms.
Conclusions
Intestinal TB in patients with vague abdominal symptoms and relevant physical findings such as pain and palpable mass should be considered to prevent late or misdiagnosis.
Introduction
Tuberculosis (TB) remains a major health problem in developing countries.Citation1 Regarding the advent of effective therapy,Citation2 the probability of the rare extrapulmonary tuberculosis is not negligible.Citation3 Intestinal TB (ITB) is the sixth most common extrapulmonary presentationCitation4 with notorious innate which should be considered before a definite diagnosis, especially in areas where TB is prevalent.Citation5
According to the existing reports in the literature, several conditions such as after anti-tumor necrosis factor therapy including concomitant use of immunosuppressants, history of latent or active TB, and being born in or spending extensive time in endemic areas would make patients susceptible for TB development.Citation1
Case report
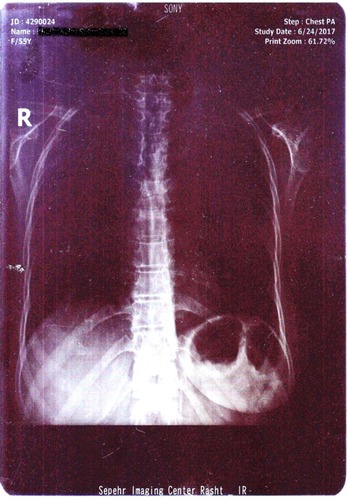
A 55-year-old woman was admitted to the Internal Medicine Department of Razi Hospital in Rasht (a city in the north of Iran) with a 30-year history of rheumatoid arthritis (RA). She declared a hypogastric, nonpositional pain without any relation to defecation or feeding, for 2 months, with previous constipation (had been cured with lactulose). Each pain episode lasted for ~5–10 minutes. She had a weight loss of 20 kg over the last 7 months. Also, had undergone endoscopy the previous year for the symptoms of nausea, diarrhea, and epigastric pain with eradicated Helicobacter pylori gastritis after a 4-week treatment. Although she had chronic anemia, there was no history of drinking alcohol or smoking, diabetes mellitus, cardiovascular disease, hyperlipidemia, or hypertension. In addition, she took prednisolone 5 mg, hydroxychloroquine 20 mg, hematinic, and supplements such as calcium, folic acid, and multivitamins daily. Furthermore, a self-discontinuation of methotrexate (MTX) was noted. The colonoscopy was performed, and only an ulcerated mass in the hepatic flexure was seen, and a biopsy was taken. As the endoscope could not pass through the hepatic flexure, the procedure was stopped (). The pathobiological features revealed ulceration and granulation tissue formation, foci of necrotizing granulomatous inflammation in lamina propria with adjacent mild crypt regenerative changes (). Moreover, Ziehl–Neelsen stained sections () revealed few acid-fast positive bacilli in the granuloma. No evidence of dysplasia or malignancy was found in the received sample. Meanwhile the polymerase chain reaction (PCR) for ITB was negative. In order to rule out pulmonary TB, radiography was performed with no evidence of pulmonary involvement (). Follow-up after a 2 week treatment with anti-TB medication demonstrated the complete disappearance of the symptoms. A written informed consent form has been provided by the patient to have the case details and any accompanying images published.
Figure 1 An ulcerated mass in the hepatic flexure.

Figure 2 The histology showed ulceration and granulation tissue formation, foci of necrotizing granulomatous inflammation in lamina propria with adjacent mild crypt regenerative changes (H&E, original magnification, 10×).
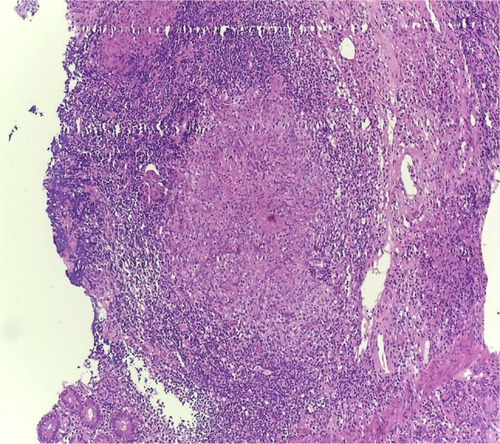
Figure 3 Acid-fast positive bacilli in the granuloma (Ziehl-Neelsen’s stain, 100×).
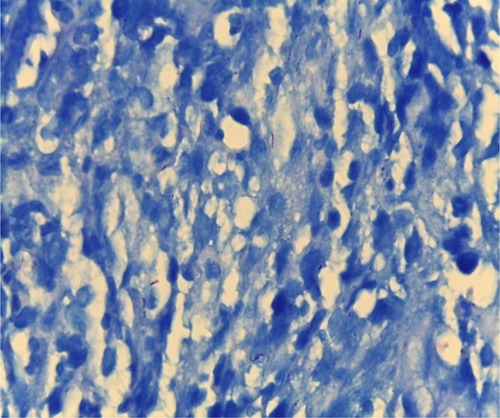
Figure 4 The chest X-ray showed no evidence of pulmonary involvement.
Discussion
TB is one of the infectious diseases prevalent all around the world.Citation6 The gastrointestinal TB leads to significant morbidity and mortality as most of the time it is not timely diagnosed and mimics other disorders such as colon cancer, lymphoma, appendicitis (as the main presumptive diagnosis),Citation6 Crohn’s disease (CD), actinomycosis, or other infectious diseases.Citation5 The coexistence of pulmonary TB (active or healed) and gastrointestinal TB is not common. It is reported that approximately <25% of patients have both.Citation7 Also, colonic tuberculosis cases without systemic features have been published.Citation8 According to its nonspecific gastrointestinal symptoms, the diagnosis is more difficult in the absence of pulmonary TB.Citation9
The total involvement of gastrointestinal tract from the esophagus to rectum through the swallowed bacterium by a hematogenous spreading or from adjacent organs is probable.Citation7,Citation10,Citation11 The frequency of involvement is different. It is stated that just 1%–3% of TB cases have ITB. In addition, it’s occurrence in distal parts of the ileocecal junction is very rare.Citation12 However, terminal ileum has more inclination for the infection after a long term intestinal mucosa contact.Citation7,Citation10,Citation11
Abdominal pain is the frequent symptom in almost all cases (>85%). Also, abdominal distension, poor absorption, nausea, vomiting, diarrhea, constipation, and weight loss are the other symptoms.Citation13,Citation14 Furthermore, palpable abdominal mass in physical examination is the other common finding. Nevertheless, the digestive bleeding is very rare.Citation15 Our patient’s symptoms were more relevant to a neoplastic mass.
Although diffuse tuberculosis colitis is not common, inflammatory stricture, polyps or tumors, and segmental ulcers are the most probable presentations.Citation16 The most important endoscopic findings are ulceration, nodularity, and luminal narrowing, which mostly impact the right colon. Also, ulcers are usually seen in the colonoscopy of patients with colonic TB (70%).Citation17 Alvares et al have reported granulomas in >54% of the colonic biopsies,Citation17 which are the most common histopathological feature of colonic TB. In endemic areas for TB, distinguishing between ITB and CD is very demanding due to the presence of granuloma.Citation5 However, the morphology of tuberculous ulcers is not the same as Crohn’s ulcers. They are typically linear, transverse, fissured, or circumferential with abnormal surrounding mucosa.Citation4 One of the considerable findings in our case was the negative result of PCR for TB while bacilli acid-fast staining was positive. According to the evidence of a recent systematic review study, PCR for Mycobacterium tuberculosis is suggested as a promising and highly specific diagnostic method to distinguish ITB from CD. However, negative results cannot exclude ITB because of its low sensitivity. Additional prospective studies are needed to further evaluate the diagnostic accuracy of PCR.Citation12 In nonendemic countries, the colonic diagnosis requires a high suspicion index of migrant population and immunosuppressed individuals. Though the deficient immune response among immunosuppressed patients can elevate the incidence and the severity of ITB,Citation18 in rare cases, it would appear in a healthy immune system, such as in Brambilla et al’s report.Citation2 Our case had a 30-year history of RA using hydrocortisone and prednisolone with self-discontinuation of MTX. There was no evidence of latent TB existence, based on no history of the tuberculin skin test; however, being infected with TB in our endemic region is not unexpected. As it is known that the majority of cases are treated properly with anti-TB treatment, and follow-up colonoscopy is not required in those who have symptomatic improvement,Citation4 after completing the treatment, the colonoscopy was not performed.
Conclusion
The role of considering ITB in patients with vague abdominal symptoms and relevant physical findings, such as pain and a palpable mass, in early diagnosis and treatment is highly effective to prevent misdiagnosis of similar disorders such as CD or colonic malignancies. Also, it should be stated that the sensitivity of PCR rather than other diagnostic methods is low.
Author contributions
All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Acknowledgments
We would like to thank all the members of Gastrointestinal and Liver Diseases Research Center (GLDRC). We also thank the patient’s family for providing consent for this case report.
Disclosure
The authors report no conflicts of interest in this work.
References
- WangMHLiuXShenBDisseminated tuberculosis in a patient taking anti-TNF therapy for Crohn’s diseaseACG Case Rep J201531454826504878
- BrambillaEDal PonteMRuschelLGSilvaPGDIntestinal tuberculosis in immunocompetent/HIV negative patients: case report of two patientsJ Coloproctol (Rio de Janeiro)2012323304307
- SantraGPaniABiswasKDIsolated rectal tuberculosis with multiple ulcersJ Assoc Physicians India2013611293493624968559
- MukewarSMukewarSRaviRPrasadADuaKSColon tuberculosis: endoscopic features and prospective endoscopic follow-up after anti-tuberculosis treatmentClin Transl Gastroenterol20123e2423238066
- WuYFHoCMYuanCTChenCNIntestinal tuberculosis previously mistreated as Crohn’s disease and complicated with perforation: a case report and literature reviewSpringerPlus2015432626180746
- KhanMZahoorIHaqEHuman immunodeficiency virus and multiple sclerosis risk: probing for a connectionJ Mult Scler2015223762389
- HorvathKDWhelanRLIntestinal tuberculosis: return of an old diseaseAm J Gastroenterol19989356926969625110
- ChoudharyAGuptaNMColorectal tuberculosisDis Colon Rectum1986297383769689
- ShahSThomasVMathanMColonoscopic study of 50 patients with colonic tuberculosisGut19923333473511568653
- AlvaresJFDevarbhaviHMakhijaPRaoSKottoorRClinical, colonoscopic, and histological profile of colonic tuberculosis in a tertiary hospitalEndoscopy200537435135615824946
- DasHSRathiPSawantPColonic tuberculosis: colonoscopic appearance and clinico-pathologic analysisJ Assoc Physicians India2000487708711011273506
- JinTFeiBZhangYHeXThe diagnostic value of polymerase chain reaction for mycobacterium tuberculosis to distinguish intestinal tuberculosis from Crohn’s disease: a meta-analysisSaudi J Gastroenterol201723131028139494
- UzunkoyAHarmaMDiagnosis of abdominal tuberculosis: experience from 11 cases and review of the literatureWorld J Gastroenterol200410243647364915534923
- LazarusAAThilagarBAbdominal tuberculosisDis Mon2007531323817224321
- KuntanapreedaKTuberculous appendicitis presenting with lower gastrointestinal hemorrhage-a case report and review of the literatureJ Med Assoc Thai200891693794218697397
- MarshallJBTuberculosis of the gastrointestinal tract and peritoneumAm J Gastroenterol19938879899998317433
- AlvaresJFDevarbhaviHMakhijaPRaoSKottoorRClinical, colonoscopic, and histological profile of colonic tuberculosis in a tertiary hospitalEndoscopy200537435135615824946
- DonoghueHDHoltonJIntestinal tuberculosisCurr Opin Infect Dis200922549049619623062