
Abstract
Objective
Penicillium species are abundant, generally saprophytic, and widely distributed in the environment. On rare occasions, they cause endophthalmitis in immunocompromised patients or in immunocompetent patients with uncontrolled diabetic mellitus or immunosuppressive agents. We report a case of endophthalmitis caused by Penicillium species in an immunocompetent patient without any disorders.
Case presentation
A 67-year-old woman presented with ocular pain, hyperemia, and blurred vision in her right eye. She was in an immunocompetent condition and had received cataract surgery without complications 3 months ago. Severe cell infiltration and a clump of 3 mm diameter were found in the anterior chamber of the right eye, and there was no abnormality in the posterior segment. Serum β-d-glucan was not elevated; bacterial culture, histological analysis, and PCR using aqueous humor did not detect any pathogen (28S rDNA 2.4×102 copies/mL). However, because the clinical findings suggested fungal endophthalmitis, anti-fungal medication was initiated. The inflammation was gradually resolved with contraction of the clump; however, it recurred 47 days after the initiation by discontinuation of antifungal medication. Examination of culture identified Penicillium species in samples from both the anterior chamber and the vitreous.
Conclusion
Chronic postoperative endophthalmitis by Penicillium species can occur in an immunocompetent patient without any systemic diseases.
Introduction
Penicillium species are abundant, generally saprophytic, and widely distributed in the environment.Citation1,Citation2 They rarely cause disease in humans, although they are increasingly recognized as a potential pathogen in immunocompromised hosts.Citation3 In the eye, Penicillium species can cause infectious keratitis,Citation4 but rarely is endophthalmitis developed, even in patients who are immunocompromised or using an immunosuppressive agent.Citation5 Exogenous fungal endophthalmitis accounts for ~10% of cases of postoperative endophthalmitis and mainly occurs in immunosuppressed patients.Citation6 Candida, Aspergillus, and Fusarium species are the most common culture-positive isolates from such patients.Citation7 We report a case of chronic postoperative endophthalmitis after cataract surgery caused by a filamentous fungus, Penicillium species, in an immunocompetent patient without any systemic diseases.
Case report
A 67-year-old woman was referred to our department with ocular pain, hyperemia, and blurred vision in the right eye. Cataract surgery had been performed for both eyes in a clinic at 3 months ago. She had no history of systemic disease and was in an immunocompetent condition. At first presentation, best-corrected visual acuity (BCVA, measured with a standard Japanese visual acuity chart and converted to Snellen visual acuity) and intraocular pressure (IOP) in the right eye were 20/20 and 17 mmHg, but slit-lamp biomicroscopy revealed a white clump of 3 mm diameter, anterior inflammatory cells, and an iris posterior synechia in the anterior segment (). There was no inflammation in the posterior segment (). Serum examination showed a slight increase in white blood cells (8,600/mm3) but not in β-d-glucan (9 pg/dL) or inflammatory proteins. Bacterial culture of the anterior humor and histological analysis of the white clump did not detect the cause of the endophthalmitis. As well, increase of 18S/28S rDNA (18S rDNA, not detected; 28S rDNA 2.4×102 copies/mL) was not presented by broad-range PCR using the aqueous humor. Because the white clumps in the anterior chamber strongly suggested fungal endophthalmitis, treatment with systemic and topical antifungal agents (systemic fosfluconazole [504 mg/d, 4 days] and topical pimaricin ophthalmic ointment [4 times/day]) was initiated in addition to antibacterial treatment (systemic cefepime [1,000 mg/d, 4 days] and topical moxifloxacin hydrochloride [6 times/day], vancomycin eyedrops [6 times/day], and ceftazidime eyedrops [6 times/day]). These medications were tapered according to the remission of the clump and inflammation in the anterior segment. At 14 days, the endophthalmitis was resolved () and the subjective symptoms had disappeared.
Figure 1 Photographs of the right eye on days 1 and 17.
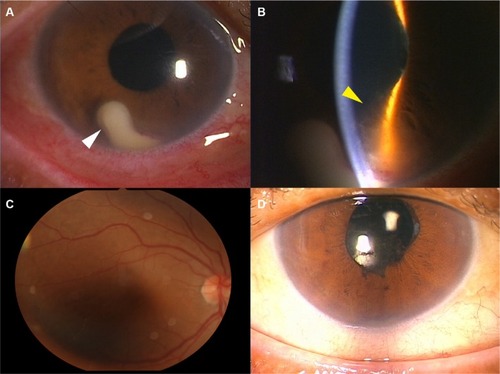
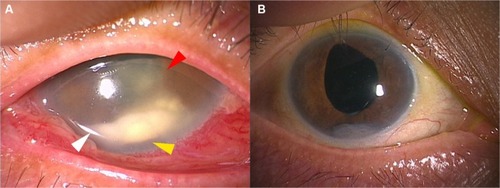
On day 47 after the initiation of treatment, she visited our hospital for headache, recurrence of ocular pain, hyperemia, and blurred vision in the right eye. BCVA was decreased to hand motion, and IOP was elevated to 40 mmHg in the right eye. Slit-lamp biomicroscopy showed reappearance of a white clump in the anterior segment, anterior inflammatory cells, large iris nodules, fibrin formation, and a posterior synechia (). The posterior segment was not visible due to inflammation in the anterior segment. Serum examination did not present an increase in β-d-glucan. Vitrectomy was emergently performed, and the aqueous humor and vitreous humor samples were obtained. Examination of microbial culture using samples from both the anterior chamber and the vitreous identified Penicillium species. We diagnosed fungal endophthalmitis caused by Penicillium species, and treatment with systemic micafungin (100 mg/d, 9 days), oral voriconazole (200 mg/d, 9 days) and flucytosine (6,000 mg/d, 9 days), and voriconazole eye drop (4 times/day) was initiated. The ocular inflammation by fungal endophthalmitis was gradually resolved with contraction of the clump after 14 days (), although the iris nodules remained. BCVA was improved to 20/16, and IOP was decreased to 16 mmHg. No recurrence was found 16 months after the second treatment.
Figure 2 Anterior segment at recurrence and at the last visit.
Informed consent
Written informed consent has been provided by the patient for the publication of her case details and images.
Discussion
Postoperative fungal endophthalmitis shows a variable presentation, ranging from localized in the anterior chamber to more diffuse intraocular inflammation.Citation6 The present case had a prolonged latency period, as in previous reports of fungal endophthalmitis, and followed these trends with diffuse anterior segment inflammation. The presence of iris nodules, as shown in this case, has been also documented in other cases of inflammation with fungal etiologies, including Candida, Fusarium, and Coccidioides species.Citation8 Therefore, endophthalmitis by Penicillium species was suspected due to the clinical findings along with the latency period.
Since Penicillium species are sometimes encountered in the clinical laboratory as culture contaminants,Citation9 diagnosis is established by histological demonstration of fungus-invaded tissue or PCR. In this case, biopsy of the iris nodules and broad-range PCR for 18S/28S rDNA were performed, as in previous reports.Citation5,Citation10 However, these methods could not detect Penicillium infection. We diagnosed Penicillium species infection from the results of microbial cultures using both the anterior humor and the vitreous samples and the efficacy of antifungal agents. We set the positive threshold value in PCR for 18S/28S rDNA because a trace amount of contamination can be detected.
Fungal contamination sometimes detected by elevation of 28S rDNA by PCR using the intraocular fluids.Citation11,Citation12 Although 2.4×102 copies/mL of 28S rDNA was detected by PCR using the aqueous humor in this case, we determined the result was negative based on these reports. However, it should be finally considered as positive.
Treatment of fungal endophthalmitis is difficult; no clear protocols exist because of the lack of well-controlled double-blind studies and the low incidence of the diseases.Citation2 In the present case, systemic fosfluconazole and topical pimaricin ophthalmic ointment did not lead to complete remission, whereas systemic flucytosine indicated a splendid effect. For Penicillium infection in HIV patients, antifungal medication including flucytosine is selected,Citation13 and flucytosine is highly active against Penicillium species.Citation1 It has been also reported that flucytosine penetrates into vitreous with higher concentration than other antifungal agents,Citation14 although the eye is a protected compartment and penetration of systemically administered antifungal agents are highly variable, particularly in the posterior segment.
Conclusion
This is a rare case of postoperative fungal endophthalmitis caused by Penicillium species in an immunocompetent patient without any systemic diseases. In these cases, if examination of microbial culture or PCR for 18S/28S rDNA using intraocular fluids are negative, antifungal treatment based on the clinical findings should be performed, which leads to the diagnosis.
Acknowledgments
This study was funded by Grant-in-Aid for Scientific Research C (M Takeuchi, 16K11337) and Grant-in-Aid for Young Scientists B (K Takayama, 17K16964) from the Ministry of Education, Culture, Sports, Science and Technology (http://www.jsps.go.jp/).
Disclosure
The authors report no conflicts of interest in this work.
References
- RandhawaPSNouraeiSRHowardDJSandhuGSPetrouMAPenicillium species as a rare isolate in tracheal granulation tissue: a case seriesJ Med Case Rep2008218418346276
- AsencioMAHuertasMCarranzaRTeniasJMCelisJGonzalez-del ValleFA case-control study of post-traumatic endophthalmitis at a Spanish hospitalInt Ophthalmol201636218519426220873
- LiYLinZShiXRetrospective analysis of 15 cases of Penicillium marneffei infection in HIV-positive and HIV-negative patientsMicrob Pathog201710532132528104384
- TakezawaYShiraishiANodaEEffectiveness of in vivo confocal microscopy in detecting filamentous fungi during clinical course of fungal keratitisCornea201029121346135220847667
- GargAStuartAFajgenbaumMLaidlawDAStanfordMChronic postoperative fungal endophthalmitis caused by Penicillium citrinum after cataract surgeryJ Cataract Refract Surg20164291380138227697258
- DurandMLBacterial and fungal endophthalmitisClin Microbiol Rev201730359761328356323
- SmithTCBenefieldRJKimJHRisk of fungal endophthalmitis associated with cataract surgery: a mini-reviewMycopathologia20151805–629129726318595
- SowmyaPMadhavanHNDiagnostic utility of polymerase chain reaction on intraocular specimens to establish the etiology of infectious endophthalmitisEur J Ophthalmol200919581281719787602
- CaggianoGNapoliCCorettiCMold contamination in a controlled hospital environment: a 3-year surveillance in southern ItalyBMC Infect Dis20141459525398412
- TakayamaKOgawaMMochizukiMTakeuchiMCytomegalovirus retinitis in a patient with proliferative diabetes retinopathyOcul Immunol Inflamm201321322522623480605
- OgawaMSugitaSWatanabeKShimizuNMochizukiMNovel diagnosis of fungal endophthalmitis by broad-range real-time PCR detection of fungal 28S ribosomal DNAGraefes Arch Clin Exp Ophthalmol2012250121877188322527320
- SugitaSShimizuNWatanabeKDiagnosis of bacterial endophthalmitis by broad-range quantitative PCRBr J Ophthalmol201195334534920675730
- LimperAHAdenisALeTHarrisonTSFungal infections in HIV/AIDSLancet Infect Dis2017
- O’DayDMHeadWSRobinsonRDSternWHFreemanJMIntra-ocular penetration of systemically administered antifungal agentsCurr Eye Res1985421311343987346