
Abstract
Aim
To evaluate the efficacy of transcutaneous triamcinolone acetonide (TA) injection for the treatment of upper eyelid retraction and swelling in thyroid eye disease (TED) patients.
Patients and methods
This is a case series. Three euthyroid TED patients with features of both upper eyelid retraction and swelling were recruited. TED signs appeared within 6 months prior to treatment. Next, 0.5 mL of TA (40 mg/mL) was transcutaneously injected targeting the orbital fat around the levator palpebrae superioris (LPS) muscle. At each visit, eyelid retraction was evaluated by palpebral fissure height and the presence of scleral show above the superior corneoscleral limbus. Eyelid swelling was judged by the appearance of upper eyelid bulging and the lack of an eyelid sulcus. In addition, the LPS muscle, orbital and retro-orbicularis oculi fat were observed using MRI before and after treatment.
Results
Two patients had resolution of their upper lid retraction and swelling within 12 months. In the other patient who had proptosis, eyelid retraction resolved, while eyelid swelling remained mild. In all cases, MRI revealed that treatment resulted in thinner LPS muscle and reduced fat swelling. In addition, both high-intensity signals on T2 images and prolonged T2 relaxation time were normalized. No adverse signs were observed.
Conclusion
Transcutaneous TA injection was effective as a treatment for upper eyelid retraction and swelling in euthyroid TED patients who had signs within 6 months prior to treatment. Transcutaneous TA injection induced reduction of LPS muscle enlargement and fat tissue swelling. These reductions by transcutaneous TA injection were verified using MRI.
Introduction
Upper eyelid retraction and swelling are frequent findings in patients with thyroid eye disease (TED).Citation1,Citation2 The incidences of eyelid retraction and swelling in TED patients are 58%–98% and 47%–75%, respectively.Citation2,Citation3 TED is three to nine times more common in women,Citation4 and patients’ age with upper eyelid retraction and swelling is mostly between 20 and 50 years.Citation2 Therefore, the appearance of such retraction and swelling causes cosmetic discomfort.Citation5,Citation6
Upper eyelid retraction usually widens the palpebral fissureCitation7 and exposes the sclera between the limbus and eyelid margin (referred to as scleral show),Citation8 while the upper eyelids normally cover the superior cornea at the 12 o’clock position. The eyelid retraction is caused by malfunction of muscles in the upper lid, primarily Mueller’sCitation9 and the levator palpebrae superioris (LPS) muscles.Citation3,Citation10 In terms of Mueller’s muscle, it has been suggested that overactivity of the sympathetic nervous system, enhanced by excessive secretion of thyroid hormone due to hyperthyroidism, stimulates the muscle tone, resulting in lid retraction.Citation9 Another mechanism could be inflammation of the LPS muscle, and inflammation of the LPS muscle is thought to be induced by antithyroid autoantibodies, that is, TSH receptor antibodies (TRAb) and thyroid stimulating antibodies (TSAb).Citation11,Citation12 During the early to middle active inflammatory phase, the LPS muscle becomes inflammatorily edematous, increasing the muscle width and restricting movement, resulting in eyelid retraction. In the late active phase, fibrosis arises, causing LPS muscle contracture and maintaining the upper eyelid retraction for a long period. For such eyelid retraction induced by inflammation, steroid therapy could be effective before the late active phase.Citation13
The swelling of the upper eyelid is caused by enlargement of the LPS muscle and eyelid/orbital fat.Citation14 Although there are no strict criteria for eyelid swelling,Citation4 it is clinically defined by eyelid bulging and lack of an upper eyelid sulcus. In MRI, T1-weighted sagittal sections reveal that eyelid swelling is caused by LPS muscle enlargement and orbital fat swelling.Citation10,Citation14 In addition, the degree of inflammatory edema in the LPS muscle could be quantitatively estimated as prolonged T2 relaxation time and high-intensity areas in T2-weighted fat-suppression images.Citation15,Citation16
Clinically, eyelid retraction frequently causes keratoconjunctivitis sicca and superior limbic keratoconjunctivitis.Citation17 The retraction and swelling of the upper eyelid often impacts quality of lifeCitation6 due to its appearance. Various treatments have resolved these issues. An α-adrenergic blocker ophthalmic solution is effective for hypertonia in Mueller’s muscle, but not for inflammation of the LPS muscle.Citation9 Botulinum toxin injection resolves upper eyelid retraction, but needs to be periodically applied.Citation18 Steroid pulse therapy has been an effective treatment, but has some side effects, including diabetes, hyperlipidemia and so on.Citation19 Surgical treatments have been performed; however, these treatments can occasionally have unexpected outcomes, including over-/undercorrection and the undesirable double eyelid line.Citation20
Recently, it has been reported that subconjunctival injection of triamcinolone acetonide (TA) targeting Mueller’s muscle is effective in reducing upper eyelid retraction in the early congestive stage of TED patients.Citation21–Citation24 Several reports suggested that subconjunctival TA injections resulted in an improvement of eyelid retraction in 68%–75% of patients from 1 to 4 times.Citation22–Citation24 In addition, it was reported that such injection reduces inflammatory enlargement of the LPS muscleCitation23 and upper eyelid swelling.Citation24 However, subconjunctival TA injection causes increased intraocular pressureCitation22–Citation24 and menstrual irregularities.Citation23
Herein, we studied whether transcutaneous TA injection targeting the LPS muscle and surrounding orbital fat was effective in reducing upper eyelid retraction and swelling in euthyroid TED patients. Treatment was initiated within 6 months of the appearance of TED signs. Using clinical assessment and MRI, significant improvement in upper eyelid retraction and swelling was observed in these patients.
Patients and methods
Between January and June 2009, patients diagnosed with TED with both upper eyelid retraction and swelling, either unilaterally or bilaterally, were recruited. Thyroid function of all patients was normal with or without medication at their first visit. Treatment was initiated within 6 months of the appearance of TED signs.
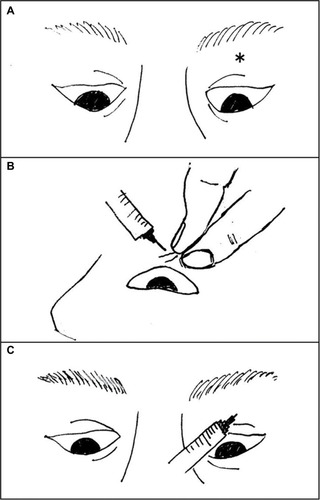
To prepare for transcutaneous TA injection, the upper eyelid was cooled with an ice pack for 1 minute to minimize pain and subcutaneous bleeding. With patients assuming downward gaze in the supine position, the upper eyelid skin was pulled (). A 26-guage needle was inserted to a depth of ~1 cm, and after confirming the absence of blood reflux, 0.5 mL of TA (40 mg/mL) was injected targeting the orbital fat around LPS muscle (). TA was injected only once for each eye.
Figure 1 The skin of the upper eyelid was pulled upward under downward gaze in the supine position).
At each visit, upper eyelid retraction and swelling were clinically evaluated (). Upper eyelid retraction was evaluated by measuring the palpebral fissure height as well as the presence of scleral show. Eyelid swelling was assessed by the presence of eyelid bulging from the upper eyelid margin and the lack of an upper eyelid sulcus. In addition, the LPS muscle and orbital fat tissue were observed using MRI before and at 6 or 8 months after treatment. LPS muscle enlargement and fat swelling were observed in T1-weighted sagittal images, and inflammatory edema in the LPS muscle was quantitatively examined with T2 relaxation time and T2-weighted fat-suppression images. Upper eyelid swelling was evaluated by the orbital fat around LPS muscle and the retro-orbicularis oculi fat (ROOF) thickness with sagittal MRI. To assess the potential for TA-induced complications,Citation22–Citation24 intraocular pressure was measured before and at 1, 3, 6 and 12 months after treatment. Patients were also questioned about any other problems including menstrual disorders.
Table 2 Palpebral fissure height and T2 relaxation time before and after TA injection
Ethics statement
Written informed consent was obtained from the patients for publication of these case reports and accompanying images.
Results
Case 1
A 35-year-old male TED patient presented with right upper eyelid retraction and swelling for 3 months. His thyroid function was normal without any medication, and he was positive for antithyroid autoantibodies, that is, TRAb (≥2.0 IU/L) and TSAb (>180%), as shown in . He was a nonsmoker and did not receive radioiodine (RI) therapy. At the first visit, palpebral fissure height was 11 and 9 mm in the right and left eye, respectively. Scleral show, bulging eyelid and a lack of the upper eyelid sulcus were observed in the right eye (). No proptosis was detected in either eye. MRI taken on the same day revealed LPS muscle enlargement and fat swelling. Prolonged T2 relaxation time and high-intensity areas in T2-weighted fat-suppression images were also noted in the LPS muscle, indicating active inflammatory edema in the muscle (; ). Transcutaneous TA was injected in the right eyelid on the same day without any complication.
Figure 2 Case 1: The right eye was treated. Before treatment, upper eyelid swelling, scleral show and a lack of an upper eyelid sulcus were evident in the right eye. Upper eyelid sulcus (arrow) slightly appeared 1 month after the injection. At 6 months, the scleral show and eyelid bulge resolved. At 12 months, no features of upper eyelid retraction and swelling were observed. Subcutaneous white particles of TA (arrowhead) were observed at 1 and 6 months. These were not detectable right after injection. The particles were not visible at 12 months. Case 2: The left eye was treated. Before treatment, scleral show, upper eyelid swelling and lack of an upper eyelid sulcus were evident in the left eye. At 1 month after treatment, a slight upper eyelid sulcus (arrow) could be detected. At 6 months, the scleral show and palpebral fissure height reduced. At 12 months, the scleral show resolved. Case 3: Both eyes were treated. Before treatment, scleral show, bulging eyelids and lack of an upper eyelid sulcus were evident in both eyes. At 1 month after treatment, the eyelid bulge reduced. At 6 months, the scleral show resolved and the palpebral fissure height reduced. At 12 months, the eyelid bulge resolved, although the upper eyelid sulcus was still not observable.
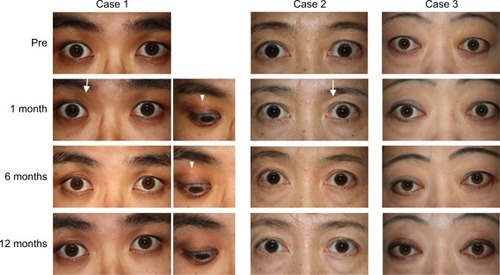
Figure 3 Case 1: Pretreatment: The top left image shows T1-weighted MRI sagittal sections. Enlargement of the LPS muscle (arrow) and swelling of eyelid fat (arrowhead) are observable in the right eye, but not in the left eye (top right). Bottom image shows high-intensity signal in the LPS muscle (arrow) on a T2-weighted fat-suppressed image. Eight months posttreatment: Top left image shows that enlargement of the LPS muscle (arrow) was reduced and swelling of fat tissue (arrowhead) was not apparent. Bottom image shows that high-intensity signal in the LPS muscle (arrow) disappeared. Case 2: Pretreatment: Top right image shows mild enlargement of the LPS muscle (arrow) and mild swelling of eyelid fat (arrowhead) in the left eye. Bottom images show high-intensity signal in the LPS muscle (arrow) on a T2-weighted fat-suppressed image. Eight months posttreatment: Top right image shows that the LPS muscle (arrow) enlargement tended to improve slightly and fat tissue (arrowhead) swelling was not observable. Bottom image shows that high-intensity signal in the LPS muscle (arrow) disappeared. Case 3: Pretreatment: Top image shows enlargement of the LPS muscle (arrow) and swelling of fat tissue (arrowhead) in both eyes. Bottom shows high-intensity signals in the LPS muscle (arrow) on T2-weighted fat-suppressed image. Six months posttreatment: Top image shows improvement of enlargement of the LPS muscle (arrow) and swelling of fat tissue (arrowhead). Bottom image shows that high-intensity signals in the LPS muscle (arrow) disappeared on a T2-weighted fat-suppressed image.
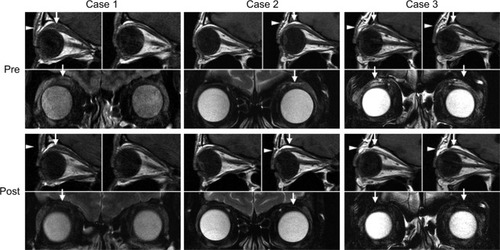
Table 1 Clinical characteristics
At 1 month after treatment, the palpebral fissure height reduced and an upper eyelid sulcus was slightly detected. At 6 months, scleral show was absent and the palpebral fissure height reduced to 9 mm, which was the same as the contra-lateral eye. There was no eyelid bulging, and the upper eyelid sulcus was obvious. At 12 months, no features of upper eyelid retraction or swelling were observed. In terms of post-TA-injective complication, particles of TA () were subcutaneously observed at 1, 3 and 6 months, whereas they were not detected immediately after injection and at 12 months. On MRI taken at 8 months, the LPS muscle and ROOF were clearly thinner than those in images before treatment. In addition, both high-intensity signals on T2-weighted fat-suppressed images and prolonged T2 relaxation time were normalized at 8 months (; ).
Case 2
A 46-year-old female euthyroid TED patient presented with left upper eyelid retraction and swelling for 5 months. She was positive for antithyroid autoantibodies (). She was a nonsmoker and did not receive RI therapy. At the first visit, right and left palpebral fissure height was 10 and 12 mm, respectively. Scleral show, eyelid bulging and lack of an upper eyelid sulcus were all noted in the left eye (). No proptosis was detected. MRI confirmed LPS muscle enlargement and fat swelling along with inflammatory edema (; ). TA was transcutaneously injected at 1 month after the first visit, without any complications.
Improvement was observed at 1 month after treatment, as evidenced by appearance of an eyelid sulcus. At 6 months, scleral show and palpebral fissure height reduced, there was no eyelid bulging, and the eyelid sulcus re-formed. At 12 months, all clinical parameters were similar to those in the contralateral eye (). MRI at 8 months confirmed normalization of swelling and inflammatory edema (; ).
Case 3
A 48-year-old female TED patient presented with bilateral eyelid retraction and swelling for 3 months. Her thyroid function was well controlled with 200 mg propylthiouracil per day, and both antithyroid autoantibodies were present (). She was a nonsmoker and did not receive RI therapy. At the first visit, palpebral fissure height (12 mm) and proptosis (19 mm) were observed in both eyes. Scleral show, eyelid bulging and lack of an upper eyelid sulcus were noted bilaterally (). MRI confirmed bilateral LPS muscle enlargement and fat swelling, along with inflammatory edema (; ). Transcutaneous TA was injected in both eyelids at 1 week after the first visit, without any complications.
At 1 month after TA injection, bilateral eyelid bulging was reduced. At 6 months, scleral show completely disappeared and palpebral fissure height reduced. At 12 months, palpebral fissure height was 10 mm in both eyes and eyelid bulging had resolved. An upper eyelid sulcus, however, was still not observable in either eye (). MRI at 6 months revealed improvement, as indicated by a thinner LPS muscle and less ROOF, along with normalization of inflammatory edema.
In all cases, thyroid function was well controlled during the follow-up period. In addition, no adverse effects arising from TA injection, for example, pigmentation and menstrual disorder, and no recurrence of eyelid retraction or swelling were detected.
Discussion
To reduce inflammation in the LPS muscle and eyelid fat, TA was transcutaneously injected targeting the orbital fat around the LPS muscle in three TED patients with eyelid retraction and swelling. In all cases, treatment led to resolution of upper eyelid retraction and swelling. Improvement of eyelid retraction was confirmed using MRI, with reduction of LPS muscle enlargement associated with a decrease of inflammatory edema, as evidenced by less LPS high-intensity signal on T2-weighted fat-suppressed images and normalization of T2 relaxation time.Citation16 In terms of eyelid swelling, improvement was detected at 1 month after treatment in all cases and an eyelid sulcus reappeared in two cases eventually. Reduced eyelid fat swelling was observed in all cases on MRI. Less improvement, however, was observed in case 3, as an eyelid sulcus was not observable up to 12 months after treatment. As case 3 was the most severe, being the only case with pro-ptosis and having higher TRAb and TSAb than others,Citation25,Citation26 this phenomenon may have affected the amount of improvement in eyelid swelling.
In a previous report,Citation23 reduction of LPS muscle enlargement was detected after subconjunctival TA injection on MRI, consistent with resolution of inflammatory edema in the LPS muscle and eyelid fat. In this study, a similar improvement in inflammatory edema was confirmed with our MRI findings, including T2-weighted fat-suppressed images and normalization of T2 relaxation time. Our patients were treated with single transcutaneous TA injection, which is considered an easier administration of the drug to the target tissue, that is, the LPS muscle and eyelid fat in these cases. Our single transcutaneous TA injection demonstrated similar efficacy to single, as well as multiple, subconjunctival TA injection,Citation21–Citation24 perhaps with fewer adverse reactions. It is thought that trans-cutaneous TA injection provides a better approach to target the LPS muscle and surrounding fat tissues.
No adverse reactions following subconjunctival TA injection were noted, although small subcutaneous nodule was noted in one case. In this case, the injection may have been shallower, resulting in TA particles becoming visible through the skin as eyelid fat swelling reduced. These visible white particles, however, were not cosmetically obvious and completely disappeared by the 12-month assessment point.
We found in this study that transcutaneous TA injection was clinically effective for upper eyelid retraction and swelling in euthyroid TED patients when treatment was initiated within 6 months of the appearance of TED signs. Thus, transcutaneous TA injection may be a promising first-line treatment for upper eyelid retraction and swelling with inflammation of the LPS muscle in euthyroid TED patients. However, our sample size was small, and further studies with larger sizes are needed to validate the efficacy of transcutaneous TA injection.
Author contributions
All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work. All authors read and approved the final manuscript.
Acknowledgments
The authors would like to thank R Inoue, G Ito, C Funaki, N Yaji and K Nishiyama for useful discussions.
Disclosure
The authors report no conflicts of interest in this work.
References
- BartleyGBFatourechiVKadrmasEFClinical features of Graves’ ophthalmopathy in an incidence cohortAm J Ophthalmol199612132842908597271
- KozakiAInoueRKomotoNProptosis in dysthyroid ophthalmopathy: a case series of 10,931 Japanese casesOptom Vis Sci201087320020420081550
- DickinsonAJClinical ManifestationsGraves’ orbitopathy: a multidisciplinary approach questions and answersWiersingaWMKahalyGJBaselKarger2010125
- DaumerieCEpidemiologyGraves’ orbitopathy: a multidisciplinary approach questions and answersWiersingaWMKahalyGJBaselKarger2010339
- PontoKAPitzSPfeifferNQuality of life and occupational disability in endocrine orbitopathyDtsch Arztebl Int20091061728328919547630
- TerweeCBGerdingMNDekkerFWPrummelMFWiersingaWMDevelopment of a disease specific quality of life questionnaire for patients with Graves’ ophthalmopathy: the GO-QOLBr J Ophthalmol19988277737799924370
- Duke-ElderSMacFaulPAMotor disorders and deformations of the lidsSystem of OphthalmologyXIII part I, chap VIIILondonHenry Kimpton1974568570
- MouritsMPHistorical Note on Graves’ diseaseGraves’ orbitopathy: a multidisciplinary approach questions and answersWiersingaWMKahalyGJBaselKarger20102719
- GayAJWolksteinMATopical guanethidine therapy for endocrine lid retractionArch Ophthalmol19667633643675952755
- OhnishiTNoguchiSMurakamiNLevator palpebrae superioris muscle: MR evaluation of enlargement as a cause of upper eyelid retraction in Graves diseaseRadiology199318811151188511284
- SmithTJHegedüsLGraves’ diseaseN Engl J Med2016375161552156527797318
- HiromatsuYSatoMInoueYLocalization and clinical significance of thyrotropin receptor mRNA expression in orbital fat and eye muscle tissues from patients with thyroid-associated ophthalmopathyThyroid1996665535629001189
- BartalenaLBaldeschiLDickinsonAConsensus statement of the European Group on Graves’ orbitopathy (EUGOGO) on management of GOEur J Endocrinol2008158327328518299459
- InoueYHigashideTYoshikawaKInoueTSagittal magnetic resonance imaging of dysthyroid ophthalmopathyEur J Ophthalmol19933131368485396
- OhnishiTNoguchiSMurakamiNExtraocular muscles in Graves ophthalmopathy: usefulness of T2 relaxation time measurementsRadiology199419038578628115640
- HiromatsuYKojimaKIshisakaNRole of magnetic resonance imaging in thyroid-associated ophthalmopathy: its predictive value for therapeutic outcome of immunosuppressive therapyThyroid1992242993051493371
- IsmailovaDSFedorovAAGrushaYOOcular surface changes in thyroid eye diseaseOrbit2013322879023565763
- ShihMJLiaoSLLuHYHyLA single transcutaneous injection with Botox for dysthyroid lid retractionEye200418546646915131675
- ZangSPontoKAKahalyGJClinical review: intravenous glucocorticoids for Graves’ orbitopathy: efficacy and morbidityJ Clin Endocrinol Metab201196232033221239515
- KazimMGoldKGA review of surgical techniques to correct upper eyelid retraction associated with thyroid eye diseaseCurr Opin Ophthalmol201122539139321730842
- CheeECheeSPSubconjunctival injection of triamcinolone in the treatment of lid retraction of patients with thyroid eye disease: a case seriesEye200822231131517917686
- LeeJMLeeHParkMBaekSSubconjunctival injection of triamcinolone for the treatment of upper lid retraction associated with thyroid eye diseaseJ Craniofac Surg20122361755175823147303
- XuDLiuYXuHLiHRepeated triamcinolone acetonide injection in the treatment of upper-lid retraction in patients with thyroid-associated ophthalmopathyCan J Ophthalmol2012471344122333849
- LeeSJRimTHJangSYTreatment of upper eyelid retraction related to thyroid-associated ophthalmopathy using subconjunctival triamcinolone injectionsGraefes Arch Clin Exp Ophthalmol2013251126127022968823
- EcksteinAKPlichtMLaxHThyrotropin receptor autoantibodies are independent risk factors for Graves’ ophthalmopathy and help to predict severity and outcome of the diseaseJ Clin Endocrinol Metab20069193464347016835285
- MukasaKYoshimura NohJKouzakiATSH receptor antibody titers measured with a third-generation assay did not reflect the activity of Graves’ ophthalmopathy in untreated Japanese Graves’ disease patientsEndocr J201663215115726581710