
Abstract
Cervical ectopic pregnancy is a rare form of ectopic pregnancy. This incidence represents less than 1% of all ectopic pregnancies with reported incidence rates varying from 1:1,000 to 1:95,000 pregnancies. Cervical ectopic pregnancy is difficult to diagnose. Hydronephrosis and hydroureter have never been reported as complications of cervical ectopic pregnancy, and both are diagnosed after laparotomy. The potential morbidity, highlighted in this case study, demonstrates the importance of early diagnosis of a cervical ectopic pregnancy so that early intervention and treatment can be employed.
Introduction
Cervical ectopic pregnancy (CEP) is a rare form of ectopic pregnancy, and it can be defined as the implantation of the blastocyst in the endocervix below the internal os.Citation1,Citation2 The cervical ectopic pregnancy is extremely rare in both naturally conceived pregnancies and assisted reproduction.Citation3,Citation4 The incidence of cervical pregnancy is less than 1% of all ectopic pregnancies, and one in 1,000–95,000 pregnancies.Citation2,Citation3,Citation5,Citation6 When the spontaneous collapse of the conceptus occurs, CEP can cause massive bleeding if it is not treated correctly; therefore, early detection and prompt termination are necessary to prevent the critical condition.Citation7,Citation8 The diagnosis of cervical ectopic pregnancy was confirmed based on the following transvaginal ultrasonographic findings: an empty uterus, a barrel-shaped cervix, a gestational sac below the level of the internal os, and blood flow surrounding the gestational sac from the cervix.Citation7,Citation9 In general, surgical or medical treatment can be considered, but the decision should depend on the symptoms, hemodynamic status, size and location of the pregnancy, and the patient’s desire to preserve fertility in the future. To date, a cervical ectopic pregnancy is often diagnosed as uncontrolled bleeding, which is treated by surgery. Different approaches that can be considered are including a conservative treatment using methotrexate, uterine artery embolization (UAE), surgical evacuation with local tamponade, and vasoconstriction therapy. Surgical intervention is indicated in the late gestation, unstable cases, or failed medical treatment. Hysterectomy may be needed in the massive hemorrhage case or case where fertility does not intend to be maintained.Citation7–Citation12 Hydronephrosis and hydroureter are uncommon complications, and both are mostly identified after laparotomy.
Case report
A 34-year-old woman, gravida 3, para 2, had a history of cesarean section twice, but there was no history of infertility and gynecology surgery. She came to our clinic because of difficult and pain in micturition, which started from one month ago. She also experienced lower abdominal pain, which became worse the longer it felt. The initial pain was cramping, but it spread throughout the lower abdomen. Other symptoms found were nausea, vomiting, recurrent painless vaginal spotting in the last two months, and pain during defecating.
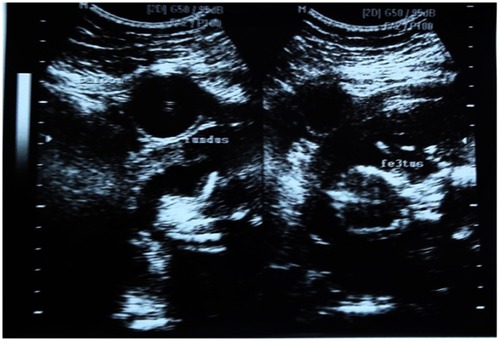
Based on the physical examination, the vital signs were found within the normal limit. The pelvic examination showed that the uterine cervix was enlarged, no adnexal mass was found, and the cervical ostium was closed. Abdominal Ultrasound showed 21–22 weeks of a singleton pregnancy. The fetal biometrics were found Biparietal Diameter (BPD): 49.5 mm, Abdominal Circumference (AC): 160 mm, Femur Length (FL): 36.4 mm and fetal cardiac activity was found. Sonographic findings also showed the bladder and bilateral hydronephrosis in her kidney (see ). After the insertion of an indwelling catheter, the bladder was emptied, the balloon catheter was inflated, and the balloon was identified with ultrasound located at the level as high as the maternal umbilicus (see ). The ultrasound was concluded as 21–22 weeks of gestation cervical ectopic pregnancy with a complication of bladder adhesion attached to the fundus of the uterus and we also included the differential diagnosis, in this case, was intrauterine pregnancy with severe adhesion with the bladder.
Figure 1 Transabdominal sonography findings show the bilateral hydronephrosis.
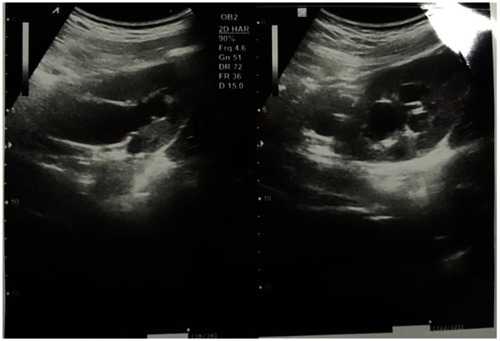
Figure 2 Transvaginal sonography findings show the balloon catheter was as high as the maternal umbilicus.
Laboratory testing revealed hemoglobin 7.9 g/dL, proteinuria (+2), and leukocyturia. The initial purpose for laparotomy in this case report is for exploration and to take down the adhesion, then remove the pregnancy and hysterectomy as the last option. Informed consent was obtained to be perfomed exploration laparotomy with the further procedure for removing the pregnancy and hysterectomy if indicated.
During laparotomy, the bladder was seen attracted upwards as high as the umbilicus. A urology specialist was also involved in this case. Thus, the separation of the bladder from the uterus was performed, and barrel-shaped cervix with posterior hyper-retroflected fundus filling the Pouch of Douglas was found. A whole part of the uterine body was seen well above the location of the fetus during laparotomy.
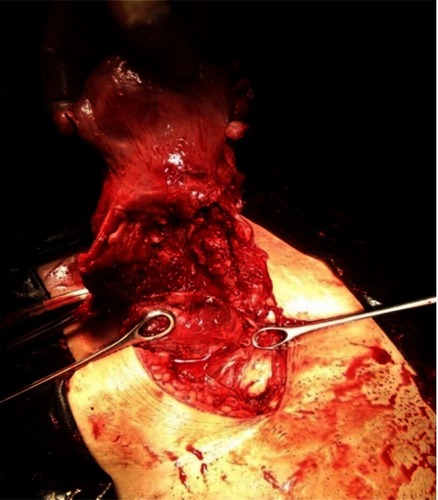
Hysterotomy incision was performed, then we remove the pregnancy (fetus and placenta) (see and ). We tried to preserve the uterus. We performed hypogastric (Internal Iliac) artery ligation prior to hysterectomy. But massive bleeding continued after the ligation procedure, therefore we performed the hysterectomy (see ).
Figure 3 The fetus after removal from the cervix.

Figure 4 The removal of the placenta from the cervix.

Figure 5 The uterus after the fetus and placenta had been removed.
Bilateral hydroureter was found due to the extremely attracted bladder, which made the lower ureter kinking near to the entry site of the ureter to the bladder. The patient received two units of packed red blood cells (RBCs) during the operation.
The postoperative period passed smoothly because the Foley’s catheter was deflated gradually after one day, and there was no vaginal bleeding. The patient was discharged five days after the intervention.
Discussion
Cervical ectopic pregnancy is one of the rarest forms of non-tubal ectopic pregnancy, and it can be defined as implantation of the blastocyst in the endocervix below the internal ostium. It accounts for less than 1% of all ectopic pregnancies, and one in 1,000–95,000 pregnancies.Citation1–Citation5 The exact etiology of cervical pregnancy is unknown.Citation5 Although cervical ectopic pregnancy is rare, there are some associated risk factors, such as previous endometrium curettage, In Vitro Fertilization-Embryo Transfer (IVF-ET), intrauterine adhesion, and previous uterine surgery such as cesarean section.Citation8 In this case, she had a history of cesarean section two times. The most common symptom of cervical pregnancy is painless vaginal bleeding (91%). However, inguinal pain is also common in this condition (26%). A classic triage of ectopic pregnancy is impaired abdominal pain, amenorrhea, and vaginal bleeding, and it is only found in about 50% of patients coming with complaints of ectopic pregnancies impaired in the cervix.Citation13,Citation14 The difficulty and pain in micturition, recurrent painless vaginal bleeding, and lower abdominal pain symptoms were found in the patient.
The methods used to diagnose cervical ectopic pregnancy have changed over time. In the past, cervical ectopic pregnancy was diagnosed intra-operatively in the presence of extensive hemorrhage at the time of uterine curettage. The advent of transvaginal ultrasound has greatly enhanced diagnostic options. However, as our case reported, sometimes even transvaginal ultrasound is insufficient to make the diagnosis.Citation14,Citation15
In our cases, we initially made a false diagnosis as adhesion of the bladder to the fundus of the uterus in 21–22 weeks of an intrauterine pregnancy with an abdominal ultrasound. The cervical pregnancy was diagnosed after laparotomy as the bladder was found to be extremely attracted, the pregnant uterus was as high as the maternal umbilicus, and the fundus of the uterus was acutely hyper-retroflected posteriorly filling the pouch of Douglas. It was also found that bilateral hydroureter with the lower part of the ureter near the entry site to the bladder was kinked. It might block the urinary tract from ureter to bladder due to the bulky cervix which compressed the ureter, attracted the bladder neck and internal urethrae os, and changed the urethra angle direction which resulted in difficulty and pain in micturition.
General principles for the management of Cervical Pregnancy include the following goals: minimise the risk of haemorrhage, evacuate the gestational cervical product and preserve the patient’s fertility.Citation16,Citation17 Management options vary and depend on the time of diagnosis and clinical presentation. The risk of hemorrhage may be reduced by cervical cerclage, intra-cervical vasopressin injection, vaginal ligation of the cervical arteries, uterine artery ligation, internal iliac artery ligation, and angiographic embolization of the cervical, uterine, or internal iliac arteries.Citation7–Citation12 Hysterectomy was performed in this case due to uncontrolled massive bleeding. Hysterectomy is the most reliable approach to control massive bleeding in cases that are refractory to all conservative treatment options; however, hysterectomy deprives the patient’s future fertility.Citation10 This is one of a rare case report which bilateral hydronephrosis and hydroureter associated with 21–22 weeks gestational age of cervical ectopic pregnancy. Moreover, there was no previous case with a complaint of difficulty and pain in micturition associated with hydronephrosis and hydroureter.
Conclusion
This is one of a rare case report of late gestational age in a cervical ectopic pregnancy with a complaint of pain and difficulty in micturition associated with bilateral hydronephrosis and hydroureter. We acknowledge that there were previous reports regarding cervical pregnancy, but a case report with complication obstruction of the urological tract which caused hydronephrosis and hydroureter was never reported before. Hydronephrosis and hydroureter have never been reported as complications in cervical ectopic pregnancy, and both are diagnosed after a laparotomy. Hysterectomy is the most reliable approach to control massive bleeding in this case. Despite the rarity of cervical ectopic pregnancy, it contributes to significant morbidity and mortality. Therefore, every effort should be made to make a precise, early diagnosis.
Consent to publish
Both of the authors have consented to publish this case report.
Ethics, consent and permissions
In this case report, the patient had read and signed an informed consent form to have the case details and any accompanying images published. Institutional approval was not required to publish the case details.
Author contributions
Both authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this case report.
References
- Gun M, Mavrogiorgis M. Cervical ectopic pregnancy: a case report and literature review. Ultrasound Obstet Gynecol. 2002;19(3):297–301. doi:10.1046/j.1469-0705.2002.00559.x11896956
- Correia L, Simoes M, Luz R, Silva A, Barros C. Cervical ectopic pregnancy: ultrasound diagnosis and conservative management. Acta Obstet Ginecol Port. 2014;8(1):84–87.
- Youssef HM, Emam M, Zayed A. Conservative management of 14 weeks cervical ectopic pregnancy: case report. Middle East Fertil Soc J. 2016;21:281–284. doi:10.1016/j.mefs.2016.05.004
- Moustafa H, Rizk B, Brooks N, Steffler B, Baker S, Puscheck E. Cervical pregnancy In: Rizk B, editor. Ultrasound in Reproductive Medicine and Infertility. Cambridge: Cambridge University Press; 2010 276–282. [chapter 33].
- Amato P. Gregg V. Pearls of Excellence Diagnosis and Management of Cervical Ectopic Pregnancy. The Foundation for Excellence in Women’ Health, Inc 1 2014.
- Kirk E, Condous G, Haider Z, Syed A, Ojha H, Bourne T. The conservative management of cervical ectopic pregnancies. Ultrasound Obstet Gynecol. 2006;27:430–437. doi:10.1002/uog.269316514619
- Ishikawa H, Unno Y, Omoto A and Shozu M. Local injection of diluted vasopressin followed by suction curettage for cervical ectopic pregnancy. Eur J Obstet Gynecol Reprod Biol. 2016;207:173–177. doi:10.1016/j.ejogrb2016.11.004
- Medhi R, Patel J, Mishra A. Cervical ectopic pregnancy presented with massive life threatening haemorrhage: a case report. Int J Reprod Contracept Obstet Gynecol. 2016;6(1):298. doi:10.18203/2320-1770.ijrcog20164679
- Chrisi C, Stratoudakis G, Zygouris D, Kastrinakis K, Daskalakis G, Panagopoulos P. Cervical pregnancy: a case report. Obstet Gynecol Int J. 2015;14(1):27–29.
- Rizk B, Holliday CP, Owens S, Abuzeid M. Cervical and cesarean scar ectopic pregnancies: diagnosis and management. Middle East Fertil Soc J. 2013;18:67–73. doi:10.1016/j.mefs.2013.01.011
- Chauhan N, Goyal P, Lal A, Chhatwal J, Shamim S. Cervical ectopic pregnancy: ultrasound diagnosis and conservative management. Int J Reprod Contracept Obstet Gynecol. 2016;3613–3615. doi:10.18203/2320-1770.
- Šijanović S, Vidosavljević D, Topolovec Z, Milostić-Srb A, Mrčela M. Management of cervical ectopic pregnancy after unsuccesful methotrexate treatment. Iran J Reprod Med. 2014;12(4):285–288.24976825
- Perkins K, Boulet S, Kissin D, Jamieson D. Risk of ectopic pregnancy associated with assisted reproductive technology in the United States, 2001–2011. Obstetrics Gynecology. 2015;125(1):70–78. doi:10.1097/AOG.000000000000058425560107
- Singh S. Diagnosis and management of cervical ectopic pregnancy. J Hum Reprod Sci. 2013;6(4):273. doi:10.4103/0974-1208.12631224672169
- Tariq A, O’Rourke M, Carstens SJ, Totten VY. Intra-abdominal rupture of a live cervical pregnancy with placenta accreta but without vaginal bleeding. Clin Pract Cases Emerg Med. 2018;2(2):116–120. doi:10.5811/cpcem.2017.10.3202929849260
- Bianchi P, Salvatori MM, Torcia F, Cozza G, Mossa B. Cervical pregnancy. Fertil Steril. 2011;95:2123e3–2123e4. doi:10.1016/j.fertnstert.2011.01.016
- Turgal M, Aydin E, Kender N, Tuncer ZS. Cervical ripening balloon: a successful treatment for massive bleeding in cervical pregnancy. J Obstet Gynaecol. 2016;36(4):531–532. doi:10.3109/01443615.2015.111650227013222