
Abstract
Background
Meningovascular syphilis, a distinct classification of neurosyphilis, has gained attention for its association with cerebral ischemia, particularly among individuals living with HIV. This unique manifestation of syphilis affects the meningeal and vascular structures of the central nervous system, leading to cerebrovascular complications. In this case report, we present the case of a young man diagnosed with neurosyphilis and HIV after presenting with an ischemic stroke. We discuss the challenges associated with diagnosing neurosyphilis, given its frequent atypical presentations that can mimic other diseases. Furthermore, we explore the management approach for these coexisting conditions.
Case Presentation
A right-handed male patient presented with a sudden paresis of the right upper and lower extremities, along with facial deviation to the left, and demonstrated low verbal output, limitation in constructing sentences, and conveying thoughts or ideas effectively. Upon admission, the patient’s neurological examination revealed a FOUR coma scale of 16. He exhibited motor aphasia, right facial paralysis sparing the forehead, and right upper and lower extremity spastic hemiparesis with a strength of 3 out of 5 on the Medical Research Council scale. The Plantar reflex was positive on the affected side. Brain magnetic resonance imaging revealed left middle cerebral artery infarction (cortical and lenticulostriate territory acute infarction).
Conclusion
This case highlights the need for treating physician to have a high index of suspicion towards meningovascular syphilis as a potential cause of stroke in young individuals. This is crucial, especially when there is also a concurrent HIV infection, as it requires specific treatment.
Keywords:
Background
Syphilis is caused by Treponema pallidum. When the organism invades the central nervous system (CNS), it is termed as neurosyphilis. Neurosyphilis can occur during any stage of the disease and is divided into early and late stages. If the patient has co-infection with HIV, the disease can progress rapidly. It can manifest in many different ways, with one of the most atypical presentations being stroke.Citation1 The relationship between syphilis and stroke is due to vasculitis and represents a diagnostic challenge for healthcare providers due to its rare presentation. Therefore, the diagnosis of syphilitic stroke requires a high index of suspicion.Citation2
Case
This is a case of a 38 year right-handed newly diagnosed HIV + male patient with no history of medications or hospitalizations. He presented with a sudden paresis of the right upper and lower extremities, along with facial deviation to the left and demonstrated low verbal output, limitation in constructing sentences, and conveying thoughts or ideas effectively. He otherwise had no loss of consciousness or abnormal body movements. There was no fever or history of head trauma. The patient had no prior history of hypertension, diabetes, or hyperlipidemia. He denied any high-risk sexual contact.
Upon admission, the patient’s neurological examination revealed a FOUR coma scale of 16.Citation3 He exhibited motor aphasia, right facial paralysis sparing the forehead, and right upper and lower extremity spastic hemiparesis with a strength of 3 out of 5 on the Medical Research Council scale. The plantar reflex was positive on the right, and Kerning’s sign, Brudzinski’s sign and Neck rigidity were all negative. The rest of the physical examination was within the normal range.
Diagnostic Assessment
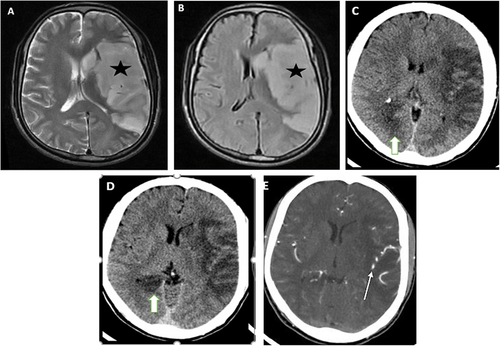
Given the acute presentation of focal neurological deficit, magnetic resonance imaging (MRI) of the brain was performed. The results revealed left middle cerebral artery infarction (fronto-temporo-parieto-insular) and lenticulostriate territory (acute infarction) ( and ). A week after his initial presentation, the patient exhibited new-onset visual disturbance and headache, promoting the decision to conduct a follow-up imaging CT scan. A new focus of hypodensity is noted involving the medial part of the right occipitotemporal lobe suggestive of right PCA territory acute infarction ( and ). The middle cerebral artery segments and its branches showed normal caliber, smooth wall, and patent lumen ().
Figure 1 (A and B) There is diffuse swelling and T2/FLAIR hyperintensity of left insular cortex, head of caudate nucleus, lentiform nucleus, lateral parts of left frontoparietal lobes and superior part of left temporal lobe (asterisk in A and B). They have marked restricted diffusion (not displayed here), which is indicative of left MCA cortical and lenticulostriatal territory acute infarction. (C and D) pre- and post-contrast CT studies done 8 days after the MRI was taken. Diffuse low attenuation is observed and a new focus of hypodensity is noted involving the medial part of occipitotemporal lobe (thick arrow in C and D) suggestive of right PCA territory acute infarction. (E) The middle cerebral artery segments and its branches showed normal caliber, smooth wall, and patent lumen (thin arrow in E).
A complete blood count (CBC) was conducted, showing a normal white blood cell count (4.8 *10^3). Further investigation of conventional cardiovascular risk factors yielded unremarkable results. Trans thoracic echocardiography did not reveal any embolic source, and routine ECG did not detect any arrhythmia. Due to the atypical stroke presentation without traditional risk factors, further investigation was pursued.
Serological testing for infectious etiologies, including syphilis and HIV (human immunodeficiency virus), was ordered. Serum RPR (Rapid plasma regain) and subsequent TPPA (Treponema Pallidum Particle Agglutination) tests were reactive; however, the titer was not reported. There was a reactive HIV antibody test, and the absolute CD4+ lymphocyte count was 451 cells/mm3. This led to the decision to perform a lumbar puncture, a lumbar puncture detected cerebrospinal fluid positive for VDRL (Venereal Disease Research Laboratory). There is no CSF pleocytosis, and all other CSF parameters were within normal limits.
Treatment and Outcome
The patient was prescribed a daily dose of 81mg aspirin and 80 mg atorvastatin, assuming that it was an ischemic stroke. In the context of the reactive syphilis and HIV serology, antimicrobial therapy of ceftriaxone 2 g intravenously (i.v.) daily for 14 days was administered, followed by benzathine penicillin intramuscularly (i.m.) at a dose of 2.4 million International Units once a week for an additional three weeks. Dolutegravir based regimen (DTG/3TC/TDF) Antiretroviral treatment was also intiated, and later, the patient was discharged for rehabilitation.
Currently, he is under long-term follow-up for HIV and neurosyphilis. The patient was regularly followed up in the outpatient clinic. A recent follow-up showed partial recovery from aphasia, and he has regained the ability to walk. The CD4 cell count remains stable.
Discussion and Conclusion
Syphilis is a sexually transmitted infection caused by the spirochete Treponema pallidum. For over 500 years, it has been a significant contributor to neurological damage. In recent years, the incidence of syphilis has been rising in correlation with the human immunodeficiency virus (HIV) epidemic.Citation4
The term neurosyphilis is used to characterize the direct invasion of T. pallidum’s in to neurological system. It has long been believed that neurosyphilis is a late symptom of syphilis; however, studies have shown that it can occur during any stage of the disease. Different degrees of central neurological involvement can be categorized as either affecting the meninges, blood vessels, or the brain tissue itself. The bacterium T. pallidum can potentially invade each of these locations directly.Citation1,Citation4
Between 0.3% and 2.4% of all syphilis patients develop meningovascular syphilis.Citation4 It appears to occur more often in relation to HIV, and several research studies indicate that the co-occurrence results in an accelerated advancement of a more severe type of neurosyphilis.Citation2 However, there have also been numerous instances of syphilitic vasculitis (SV) in young, immunocompetent stroke patients.Citation5,Citation6
The meningovascular complications of syphilis occur due to a condition called focal syphilitic endarteritis. This condition is characterized by inflammation and fibrous changes in the outer layer of blood vessels, as well as the growth of fibroblasts in the inner layer and weakening of the middle layer. As a result, it leads to the formation of blood clots and reduced blood supply to the brain, causing ischemic infarction or tissue damage due to a lack of oxygen.Citation1
In 3% of all syphilis patients and 10% of neurosyphilis patients, the first symptom is a strokeCitation1 there have been multiple instances documented in medical literature where neurosyphilis has been observed to manifest as a stroke or a syndrome resembling a stroke.Citation6
In a case similar to ours, there was a case report that described a young man who initially presented with an ischemic stroke and was later diagnosed with both HIV and neurosyphilis.Citation4 Similarly, another case report described a patient with a comparable set of symptoms and clinical presentation with a significant presence of high-risk sexual behavior. Magnetic resonance imaging later revealed an area of subacute pons ischemia.Citation7 Additionally, there have been reports of several brainstem disorders linked to neurosyphilis. Additionally, a solitary case has been recorded involving an occlusion of a cerebral aneurysm in the posterior communicating artery due to syphilitic vasculopathy.Citation8
The extent and site of the infarction correlate with the type of neurological impairments. Although the anterior circulation is more frequently affected, meningovascular syphilis can also affect the posterior circulation.Citation6 MRI with high-resolution vessel wall imaging (HR-VWI) can be useful for diagnosing stroke and depicting vessel wall inflammation associated with infectious vasculitis, in cases of neurosyphilis vasculitis manifesting as ischemic stroke.Citation9 Besides, HR VWI can detect vasculitis even in cases with a normal time of flight angiography (TOF) MRI, allowing treatment before an ischemic parenchymal lesion occurs.Citation10–12 Both CT and MRI can identify cerebral infarctions as tiny deep focal lesions. Cerebral infarctions in meningovascular syphilis, in contrast to atherosclerotic cerebrovascular disease, are usually highly distinct due to the involvement of a single artery.Citation9 In the analysis of 14 new cases of meningovascular syphilis, 71% of the patients had cerebral infarction, which was present in two patients in multiple territories and in a deep region in 28% of all patients.Citation2
CSF abnormalities occurring in neurosyphilis include pleocytosis (45 WBC per high-power field), low glucose (<2/3 serum glucose), and elevated protein (445 mg/dl). In up to 4% of patients with symptomatic neurosyphilis, CSF protein, glucose, and WBC count may be entirely normal, especially in advanced stages of the disease.Citation6 In the case presented here, the patient’s CSF showed no pleocytosis.
In advanced stages of the disease, such as tabes dorsalis, MRI demonstrates the signs of tabes dorsalis, especially in the thoracic segment as longitudinal T2-WI hyperintensities along the fascicles gracile and cuneiform, evolving to intense cord atrophy in late phases. Differential diagnosis of this condition to be considered are HIV and HTLV infections, deficiency of B12 vitamin (subacute combined degeneration of the cord).Citation13
When interpreting CSF results in HIV-positive and syphilis-positive individuals, care must be taken. Patients with HIV may exhibit a variety of CSF abnormalities, including an increase in CSF protein, WBC count (mostly lymphocytes), and immunoglobulin (both of intrathecal and extrathecal origin). Some have proposed a higher cutoff rate for CSF WBCs in the diagnosis of neurosyphilis, with 20 cells/mL being used in one study, as patients with HIV have been observed to have elevated WBC counts in their CSF attributable to HIV infection alone.Citation4 In the absence of significant blood contamination of the CSF sample, a positive CSF VDRL or RPR test is regarded as indicative of neurosyphilis. The CSF VDRL test is extremely specific, even in situations when serum VDRL or RPR titers are high (up to 1:256). The results will yield a false-positive outcome only if there is sufficient blood contamination that affects the CSF.Citation1
The suggested treatment for patients with neurosyphilis or ocular syphilis consists of administering aqueous crystalline penicillin G at a daily dose of 18–24 million units. This can be given either through continuous infusion or in divided doses, and the treatment duration typically spans 10–14 days. Alternatively, intramuscular (IM) procaine penicillin G with oral probenecid can be used.Citation11 Ceftriaxone taken intramuscularly (IM) or intravenously (IV) is a suitable alternative therapy. According to the rates of complete clinical response at one month and serological response at six months, ceftriaxone was shown to be just as effective as the gold standard, benzylpenicillin, for the treatment of neurosyphilis.Citation14
Although parenteral penicillin G is generally recommended by treatment guidelines, our patient was treated with ceftriaxone IV as an alternative therapy due to the scarce availability of penicillin medications. Following that, the treatment was continued for an additional three weeks with benzathine penicillin G IM. Such therapy led to a near complete reversal of stenosed major intracranial arteries, which was evident on a late follow-up MRA done months after antimicrobial treatment.Citation5
Treatment for neurosyphilis is considered successful in patients when neurological symptoms improve, disappear, or stabilize, and CSF abnormalities return to normal. The CDC recommends patients to have another lumbar puncture every six months until the CSF WBC count returns to normal. Retreatment should be considered if the cell count has not dropped after six months or if the CSF cell count or protein is not normal after two years.Citation15
Additionally, there are no differences in the treatment of neurosyphilis between HIV-positive and non-HIV patients.Citation6 However, it is important to note that HIV-positive patients with symptomatic neurosyphilis may have a higher likelihood of not responding to treatment, as determined by clinical and serological criteria. They may also face challenges in normalizing CSF abnormalities, even with adequate neurosyphilis treatment. As a result, routine follow-up with additional CSF testing is recommended for HIV-infected patients.
Conclusion
Syphilis and stroke can have more severe consequences in individuals who are HIV-positive due to the combined effects of weakened immune systems, accelerated disease progression, and increased inflammation. Regular medical care, adherence to antiretroviral therapy, and safe sexual practices are essential for preventing and managing both conditions and reducing the associated risks. Furthermore, this case highlights the importance of having a high index of suspicion for neurovascular syphilis in younger individuals who present with a diagnosis of cerebrovascular disease.
Abbreviations
CBC, Complete Blood Count; CSF, cerebro-spinous fluid; LP, Lumbar puncture; MRI, Magnetic resonance imaging; MRV, Magnetic resonance venography; RVI, Retroviral Infection.
Ethics Approval and Consent to Participate
Authors’ institution does not require ethical approval for publication of a single case report.
Consent to Participate
Written informed consent has been provided by the patient to have the case details and any accompanying images published.
Disclosure
The authors declare that there are no competing interests in this work.
Acknowledgment
The authors express their gratitude to the patient and the department of internal medicine of Hawassa Referral Hospital. This paper has been uploaded to Research square preprints as a preprint. https://www.researchsquare.com/article/rs-3349472/v1.
Data Sharing Statement
All data sets on which the conclusions of the case report based are available from the corresponding author on reasonable request.
Additional information
Funding
References
- Abkur TM, Ahmed GS, Alfaki NO, O’Connor M. Neurosyphilis presenting with a stroke-like syndrome. Case Rep. 2015;2015:bcr2014206988.
- Aziouaz F, Mabrouki FZ, Chraa M, et al. Analysis of fourteen new cases of meningovascular syphilis: renewed interest in an old problem. Cureus. 2021;13(8). doi:10.7759/cureus.16951
- Almojuela A, Hasen M, Zeiler F. The Full Outline of UnResponsiveness (FOUR) Score and its use in outcome prediction: a scoping systematic review of the adult literature. Neurocrit Care. 2019;31(1):162–175. doi:10.1007/s12028-018-0630-9
- Ho EL, Spudich SS. Neurosyphilis and the impact of HIV infection. Sexual Health. 2015;12(2):148–154. doi:10.1071/SH14195
- Batinić D, Antulov R, Klupka‐Sarić I, et al. Cerebral infarction as initial manifestation of meningovascular neurosyphilis in an immunocompetent patient–A case report with long term follow‐up. Clin Case Rep. 2023;11(3):e7021. doi:10.1002/ccr3.7021
- Chahine LM, Khoriaty RN, Tomford WJ, Hussain MS. The changing face of neurosyphilis. Int J Stroke. 2011;6(2):136–143. doi:10.1111/j.1747-4949.2010.00568.x
- Barragán EP, Hernández EU, Orozco BP, González MS. Meningovascular neurosyphilis with basilar artery thrombosis in HIV patient. J Infect Public Health. 2018;11(3):439–441. doi:10.1016/j.jiph.2017.09.009
- Holland BA, Perrett LV, Mills CM. Meningovascular syphilis: CT and MR findings. Radiology. 1986;158(2):439–442. doi:10.1148/radiology.158.2.3941870
- Feitoza L, Stucchi RSB, Reis F. Neurosyphilis vasculitis manifesting as ischemic stroke. Revista da Sociedade Brasileira de Medicina Tropical. 2020;53:e20190546. doi:10.1590/0037-8682-0546-2019
- Pinho M, Hall J, Cross J, Shang T, Madhuranthakam A, Moore W. Intracranial vessel wall MRI in Clinical practice: technical considerations, current and emerging applications, and clinical pearls and pitfalls. Neurographics. 2018;8(2):97–118. doi:10.3174/ng.9170237
- Mandell D, Mossa-Basha M, Qiao Y, et al. Intracranial vessel wall MRI: principles and expert consensus recommendations of the American Society of Neuroradiology. Am J Neuroradiol. 2017;38(2):218–229. doi:10.3174/ajnr.A4893
- de Oliveira Narvaez E, de Carvalho Ramos M, Do Amaral LLF, Reis F. Neurosyphilis and high-resolution vessel wall imaging: a powerful tool to detect vasculitis and neuritis. Neurol India. 2022;70(1):160–161. doi:10.4103/0028-3886.338673
- Portela L, Cardoso TM, Reis F. Muscular and brain cysticercosis. Revista da Sociedade Brasileira de Medicina Tropical. 2023;56:e0439–2023. doi:10.1590/0037-8682-0439-2023
- Bettuzzi T, Jourdes A, Robineau O, et al. Ceftriaxone compared with benzylpenicillin in the treatment of neurosyphilis in France: a retrospective multicentre study. Lancet Infect Dis. 2021;21(10):1441–1447. doi:10.1016/S1473-3099(20)30857-4
- Workowski KA, Bachmann LH, Chan PA. Sexually transmitted infections treatment guidelines, 2021. MMWR Recommendations Rep. 2021;70(4):1–187. doi:10.15585/mmwr.rr7004a1