
Abstract
Background
The association between glioblastoma and intracranial aneurysm is rare. Treatment guidelines do not exist, and operative mortality and morbidity are significantly high. To our knowledge, no prior cases have employed endovascular therapy for the treatment of these intra-tumor intracranial aneurysms followed by tumor resection.
Case presentation
A 74-year-old male, history of a left A2 aneurysm, presented after a motor vehicle accident at low speeds. Imaging was concerning for a possible traumatic brain contusion, an aneurysmal hemorrhage given history of left A2 aneurysm, or a hemorrhage from an underlying tumor given profound edema. The patient was discussed at the brain tumor board, where the plan was to address the aneurysm followed by resection of the mass versus close monitoring with subsequent imaging. The high risk of rehemorrhage, given the real possibility of an aneurysmal hemorrhage, motivated prompt treatment of the aneurysm. The patient was taken to the angiography suite; an anterosuperiorly projecting azygous A2 aneurysm, measuring 4.5 mm × 5.5 mm with a neck width at 3.5 mm and a small daughter sac, was completely obliterated with primary coiling. The following day, he underwent a left craniotomy along a forehead skin crease for mass excision. Final pathology revealed glioblastoma. The patient recovered well from both procedures, with a baseline neurological exam. The patient subsequently underwent hypofractionated radiation and temodar.
Conclusion
To our knowledge, no prior cases have employed endovascular therapy for the treatment of these intracranial aneurysms. We emphasize that efforts to introduce less invasive elements may improve the overall outcomes in this rare patient population.
Introduction
The association between intracranial tumor and aneurysm is uncommon. Reported incidence has ranged between 0.3% and 4%.Citation1–Citation4 The subset that involves glioblastoma is rare. Cases from literature have been organized into three general categories:Citation5 1) simultaneous discovery of both pathologies,Citation1,Citation3,Citation6–Citation11 2) development of glioblastoma after the treatment of aneurysm,Citation12,Citation13 and 3) development of aneurysm after treatment of glioblastoma.Citation1,Citation5 The actual incidence of this association may be higher, since angiography is seldom completed for brain tumors.Citation5 Intracranial aneurysms may arise at a location remote to the glioblastoma in some instances,Citation5,Citation8 while in others they may be anatomically close to the tumor.Citation7,Citation10
Overall, the operative mortality for patients with a brain tumor and a cerebral aneurysm is significantly high, close to 40%.Citation2 For patients with dual pathologies, no clear guidelines exist. Past treatment strategies have varied, but have mainly emphasized a combination of aneurysm clipping and tumor debulking. To our knowledge, there have been no cases that employed a staged approach, consisting of endovascular intervention and followed by tumor excision. We report such a scenario, where the initial presentation also involved a traumatic brain injury, which further complicated the treatment strategy. Moreover, we review the literature regarding patients with dual pathologies.
Case report
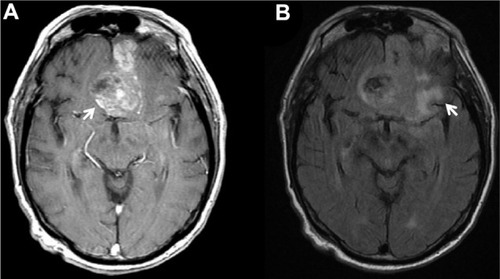
A 74-year-old male, history of a left A2 aneurysm, presented after a motor vehicle accident at low speeds. At the scene, the patient exhibited confusion. He sustained abrasions above his left eye, around his nose, and above his lip. Upon further investigation, patient had also had a syncopal episode on the prior day, where he fell and hit his head as well. Besides the confusion, he exhibited no focal neurological deficits. A computed tomography (CT) head demonstrated a 4 cm × 6 cm hyperdensity and edema with mass effect on left frontal area (). The concerns included possible traumatic brain contusion, aneurysmal hemorrhage (given history of left A2 aneurysm), or hemorrhage from an underlying tumor given profound edema. The patient was started on fosphenytoin. A CT angiography of the head demonstrated a pericallosal cerebral aneurysm (). A magnetic resonance imaging of the brain demonstrated a bifrontal, enhancing brain lesion with surrounding edema, concerning for a high-grade glioma (). Subsequently, he was started on intravenous decadron.
Figure 1 Axial CT demonstrates midline hyperdensity (arrow; A), and left frontal surrounding hypodensity (arrow; B).
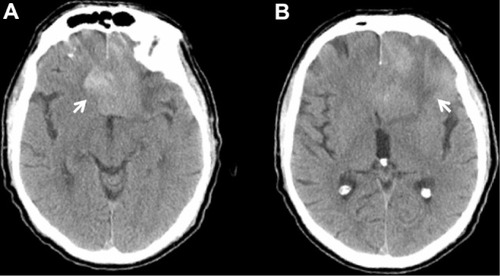
Figure 2 (A) Sagittal CT head angiography demonstrates A2 aneurysm (arrow). Diagnostic subtraction angiography (B) and (C) exhibit complete occlusion of A2 aneurysm after primary coiling (arrows).

Figure 3 (A) Axial MR T1 with contrast demonstrates heterogeneously enhancing lesion along midline and left frontal area (arrow). (B) Axial MR FLAIR demonstrates perilesional edema (arrow).
The patient was discussed at the brain tumor board, where the plan was to address the aneurysm followed by resection of the mass versus close monitoring with subsequent imaging. The high risk of rehemorrhage, given the possibility of an aneurysmal hemorrhage, motivated prompt treatment of the aneurysm. The patient was taken to the angiography suite. An anterosuperiorly projecting azygous A2 aneurysm, measuring 4.5 mm × 5.5 mm with a neck width at 3.5 mm and a small daughter sac, was completely obliterated with primary coiling (). Visualization of the external carotid arteries and internal carotid arteries bilaterally did not show any tumor blush. The following day, he underwent a left craniotomy along a forehead skin crease for mass excision. Final pathology revealed glioblastoma. The patient recovered well from both procedures, with a baseline neurological exam. The patient subsequently underwent hypofractionated radiation and temodar. The Medical College of Wisconsin does not require Institutional Review Board approval or patient consent for this case study.
Discussion
For patients with an intracranial tumor and an aneurysm, Pia et alCitation2 noted that 69% of cases exhibited initial symptoms attributed to the tumor, while 22% exhibited symptoms consistent with the aneurysm, and 6% demonstrated symptoms associated with both pathologies. Our patient presented after a traumatic brain injury, but the history of recent confusion prior to his car accident insinuates the effects from the frontal mass and surrounding edema.
The etiology of hemorrhage in our patient remains unclear. CT head was consistent with intralesional hemorrhage. Moreover, there may be a component of traumatic brain injury given his physical findings and mechanism of injury. Glioblastoma has a recognized tendency for intratumoral hemorrhage.Citation14–Citation18 However, presentation with subarachnoid hemorrhage is infrequent, with reported incidences ranging between 1.4% and 4.9%.Citation19,Citation20 Based on the ISUIA study, the A2 aneurysm in our patient has a low risk of hemorrhage, given its location along the anterior circulation and its relatively small size;Citation21 on the other hand, the presence of a daughter sac may increase the risk for hemorrhage.Citation22,Citation23 Overall, there was a significant concern that the hyperdensity represented aneurysmal hemorrhage, which prompted treatment of the existing aneurysm given risks for rehemorrhage.
The pathogenesis for intracranial aneurysm in the presence of glioblastoma has been debated. One theory involves the alteration in flow dynamics;Citation5 aneurysms may be linked to the arteries that supply glioblastomas; pathological low-resistance vessels that result in arteriovenous shunting are present in glioblastomas; an increase in flow may augment hemodynamic stress and contribute to the development of an aneurysm, not unlike the pathogenesis of aneurysms within arteriovenous malformations.Citation5,Citation10 Another notion suggests that tumor invasion of blood vessels may lead to development of an aneurysm. Glioblastoma is characterized by endothelial proliferation, necrosis, telangiectasia, and fibrosis of adjacent blood vessels.Citation6,Citation24 Andrews et alCitation6 discovered glial fibrillary acidic protein staining within the walls of aneurysm that was associated with a glioblastoma. Moreover, Aoki et alCitation7 described a dissection of the middle cerebral artery by tumor cells; similarly, Cowen et alCitation24 noted fusiform dilatation of pericallosal arteries caused by infiltration of tumor cells.
For aneurysms that develop after the treatment of glioblastoma, radiation may also play a role in pathogenesis.Citation5,Citation10,Citation25 Radiation may cause vasculopathy, characterized by endothelial damage that progresses to inflammation, thrombosis, intimal narrowing, and atherosclerosis.Citation25 These histological alterations, which predominantly influence the media and the intima, may lead to fragile points along blood vessels that are prone for aneurysmal formation.Citation25 Brachytherapy, whole brain radiation, and stereotactic radiosurgery have all been implicated with the development of intracranial aneurysms.Citation25
highlights the English literature regarding cases with simultaneous presentation of a glioblastoma and an intracranial aneurysm. Several cases involve a 1-stage approach where both are treated (Cases 6, 9, 11, 13, and 15). A few cases involved a 2-stage approach (Cases 1, 8, and 10); however, Case 10 involved a postoperative hemorrhage from a previously undiagnosed anterior communicating artery aneurysm that necessitated a second surgery while Case 8 involved a glioblastoma that was undiagnosed until pathology of the aneurysm and surrounding tissue had resulted. Details were unclear regarding a 1-stage or 2-stage approach in Cases 4 and 5. In Cases 7, 14, and 16, the pathologies were discovered at different times, and as such were treated in a “staged” fashion. Surgical treatment of the aneurysms includes clipping, muscle wrapping, resection, and vessel sacrifice. Our case involved a 2-stage approach, which entailed primary coiling of the A2 aneurysm, followed by excision of the tumor. No cases have detailed this type of approach. The operative mortality of patients with the association of a brain tumor and an intracranial aneurysm is significantly high. Besides the concern for intraoperative aneurysmal rupture, there have been instances of postoperative hemorrhage if the aneurysm was not addressed.Citation1,Citation26 Although employment of endovascular therapy entails an additional procedure, the opportunity to introduce a less invasive element may help reduce morbidity and mortality in such cases. As in our case, if there is a concern of aneurysmal rupture and subsequent risk for rehemorrhage, we recommend therapy be directed at the aneurysm first. Open surgical treatment directed at the aneurysm would lead to significant alteration of the tumor anatomy and margin and would hinder subsequent tumor resection effort. Alternatively, performing tumor resection first without securing the aneurysm would risk the rerupture of the aneurysm during the case, a source of morbidity and mortality. This report proposes a definitive treatment regimen addressing both the tumor and the aneurysm with good outcomes. This treatment regimen should be an option for patients suspected to have these dual pathologies.
Table 1 Available English literature review
Conclusion
The simultaneous presentation of a glioblastoma and an intracranial aneurysm is rare. Treatment guidelines do not exist, while operative mortality and morbidity is significantly high. To our knowledge, no prior cases have employed endovascular therapy for the treatment of these intracranial aneurysms. We emphasize that efforts to introduce less invasive elements may improve the overall outcomes in this rare patient population.
Acknowledgments
The research did not receive any funding from organizations or grants.
Disclosure
The authors report no conflicts of interest in this work.
References
- TaylorPEDelayed postoperative hemorrhage from intracranial aneurysm after craniotomy for tumorNeurology19611122523113775638
- PiaHWObradorSMartinJGAssociation of brain tumours and arterial intracranial aneurysmsActa Neurochir (Wien)1972271892044669242
- HondaMKamadaKNakataYHaradaTIwanagaHTsukamotoMThe association of cerebral aneurysm with malignant brain tumor – report of a case (author’s transl)No Shinkei Geka19808106510706256677
- OkamuraTWatanabeYKamedaHAokiHKurokawaKCoexistence of brain tumors and cerebral aneurysms – clinical considerations from eight cases (author’s transl)Neurol Med Chir (Tokyo)1981216016086167883
- YoonWSLeeKSJeunSSHongYKDe novo aneurysm after treatment of glioblastomaJ Korean Neurosurg Soc20115045745922259694
- AndrewsBTRaffelCRosegayHSubarachnoid hemorrhage from a peripheral intracranial aneurysm associated with malignant glioma: report of a caseNeurosurgery1985176456492997658
- AokiNSakaiTOikawaATakizawaTKoikeMDissection of the middle cerebral artery caused by invasion of malignant glioma presenting as acute onset of hemiplegiaActa Neurochir (Wien)19991411005100810526083
- ChengWYShenCCMinimally invasive approaches to treat simultaneous occurrence of glioblastoma multiforme and intracranial aneurysm – case reportMinim Invasive Neurosurg20044718118515343437
- GokalpHZAvmanNOzkalEGokbenBBrain tumour associated with intracranial arterial aneurysmActa Neurochir (Wien)1980532672736252754
- HashiguchiAMoriokaMIchimuraHMimataCKuratsuJGlioblastoma with an intratumoral feeding-artery aneurysmClin Neurol Neurosurg200710930230417222964
- PaolettiPRodriguez y BaenaRSangiovanniGScelsiMAssociation of a malignant glioma and an aneurysm of the middle cerebral artery. Report of a caseJ Neurosurg Sci1983272112176663355
- De ChiaraABenvenutiDMaiuriFGiamundoALavanoAAssociation of internal carotid aneurysm and temporal glioblastomaNeurochirurgia (Stuttg)19862958603713956
- LicataCPasqualinAFreschiniABaroneGDa PianRManagement of associated primary cerebral neoplasms and vascular malformations: 1. Intracranial aneurysmsActa Neurochir (Wien)19868228383751702
- KimYJLeeSKChoMKKimYJIntraventricular glioblastoma multiforme with previous history of intracerebral hemorrhage: a case reportJ Korean Neurosurg Soc20084440540819137090
- InamasuJKuramaeTNakatsukasaMGlioblastoma masquerading as a hypertensive putaminal hemorrhage: a diagnostic pitfallNeurol Med Chir (Tokyo)20094942742919779291
- LakicevicGArnautovicKMuzevicDChesneyTCerebellar glioblastoma multiforme presenting as hypertensive cerebellar hemorrhage: case reportJ Neurol Surg Rep201475e117e12125097829
- WakaiSYamakawaKManakaSTakakuraKSpontaneous intracranial hemorrhage caused by brain tumor: its incidence and clinical significanceNeurosurgery1982104374447099393
- KondziolkaDBernsteinMReschLSignificance of hemorrhage into brain tumors: clinicopathological studyJ Neurosurg1987678528573316531
- GlassBAbbottKHSubarachnoid hemorrhage consequent to intracranial tumors; review of literature and report of seven casesAMA Arch Neurol Psychiatry19557336937914360854
- LocksleyHBSahsALSandlerRReport on the cooperative study of intracranial aneurysms and subarachnoid hemorrhage. 3. Subarachnoid hemorrhage unrelated to intracranial aneurysm and A–V malformation. A study of associated diseases and prognosisJ Neurosurg196624103410565327711
- WiebersDOWhisnantJPHustonJ3rdUnruptured intracranial aneurysms: natural history, clinical outcome, and risks of surgical and endovascular treatmentLancet200336210311012867109
- MatsukawaHUemuraAFujiiMKamoMTakahashiOSumiyoshiSMorphological and clinical risk factors for the rupture of anterior communicating artery aneurysmsJ Neurosurg201311897898323240701
- UCAS Japan InvestigatorsMoritaAKirinoTThe natural course of unruptured cerebral aneurysms in a Japanese cohortN Eng J Med201236624742482
- CowenRLSiqueiraEBGeorgeEAngiographic demonstration of a glioma involving the wall of the anterior cerebral artery. Report of a caseRadiology1970975775785491743
- NanneyAD3rdEl TecleNEEl AhmadiehTYIntracranial aneurysms in previously irradiated fields: literature review and case reportWorld Neurosurg20148151151924148882
- YamadaHTaomotoKPostoperative subarachnoid hemorrhage from an intracranial aneurysm after craniotomy for astrocytoma – case reportNeurol Med Chir (Tokyo)1989298468492480546
- AliRPabaneyARobinAMarinHRosenblumMGlioblastoma and intracranial aneurysms: case report and review of literatureSurg Neurol Int201566625969791