
Abstract
Purpose
To evaluate clinical features of infectious keratitis at a tertiary referral center in a rural area of Korea.
Results
This was a retrospective study. Medical records of 70 patients who were diagnosed with infectious keratitis and underwent corneal culture were reviewed. Data including demographics, predisposing factors, and microbiological profiles were collected and analyzed.
Results
Age distribution showed one peak at sixth and seventh decade, and 48 patients (68.6%) were ≥50 years old. The male to female ratio was 43 (61.4%):27 (38.6%). Ocular surface disease was the most frequently found (48 cases, 68.6%). Gram-positive bacteria were most common (ten patients, 66.7%), followed by Gram-negative bacteria (three patients, 20%) and fungi (two patients, 13.3%). In this study, 34.3% of patients were treated by at least one topical antimicrobial before culture. Patients who received topical therapy before culture showed positive culture rate of 16.7%, and patients who underwent corneal culture without topical antibiotics showed positive culture rate of 23.9%. However, there was no statistically significant difference between the two groups in positive culture rate (P=0.554).
Conclusion
The proportions of the elderly and male patients were higher than the young and female patients, respectively. Gram-positive bacteria were the most common pathogens, and ocular surface disease was the most common predisposing factor.
Introduction
Infectious keratitis is potentially devastating disease that can lead to serious visual impairment.Citation1,Citation2 To prevent permanent vision loss, early identification of causative organisms and prompt initiation of adequate antibiotics are important.Citation3,Citation4 Understanding the recent characteristics of infectious keratitis including predisposing factor and microbiologic profile are essential in the treatment of the condition. Clinical features of the disease vary according to age, area of inhabitation, socioeconomic status and general condition, and may also change over time.Citation5–Citation7 Recently, for instance, infectious keratitis associated with contact lens (CL) wear in younger patients has increased with the corresponding widespread use of CL.Citation5–Citation7
Profiles of infectious keratitis have been reported worldwide, including those from Korea.Citation1,Citation3,Citation5,Citation6,Citation8–Citation12 However, to the best of our knowledge, information regarding infectious keratitis of patients residing in rural Korea has never been reported.
In this study, we investigated the clinical features of infectious keratitis including predisposing factors and microbiological profile at a tertiary referral center in rural area of Korea.
Patients and methods
This retrospective study included 70 patients who were diagnosed with infectious keratitis and underwent corneal culture at Kangwon National University Hospital from June 2007 to October 2014. Medical records were reviewed and analyzed for data including demographics, microbiologic profile, and predisposing factors. The study conformed to the tenets of the Declaration of Helsinki. Ethical approval and patient consent was not obtained because this is a retrospective study in which only review of medical records was done.
In every case, scraping on the corneal lesion with a sterile blade was performed, and culture of the corneal sample was done using blood agar plate, chocolate agar plate, Thioglycollate broth, Sabouraud’s agar, and Brain–Heart infusion broth. If there was growth on the cultures, Gram staining and potassium hydroxide mount were performed. Empirical medical therapy was started immediately after the corneal scraping. Most patients received combination of topical 10% cefazolin and 2% gentamicin as a primary antibiotics treatment, and topical levofloxacin or moxifloxacin was used in some cases. In cases with corneal ulcer greater than 3 mm in diameter or rapidly progressing inflammation, 3.1% vancomycin and 2% amikacin were chosen as a primary treatment. Antifungal agents including 0.5%–3% amphotericin or 1% voriconazole were also initiated in cases with suspicious fungal infection. After culture results were available, we changed antibiotics based on the sensitivity tests.
Positive culture rates according to previous use of antibiotics were compared using Fisher’s exact test, and P-value <0.05 was considered significant. SPSS for Windows (version 18.0, SPSS Inc., Chicago, IL, USA) was used for statistical analyses.
Results
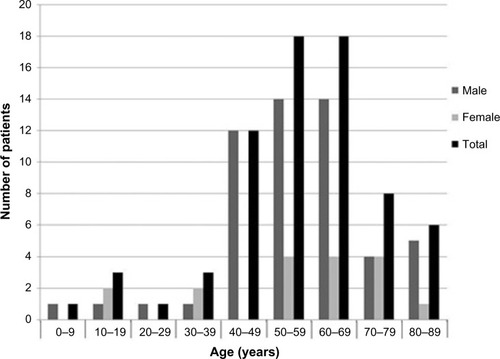
Study population comprised 53 (76%) men and 17 (24%) women. The mean age of all subjects was 56.7±17.0 years (range, 6–88 years). Forty-eight patients (69%) were ≥50 years old, whereas eight patients (11%) were <40 years old. Unimodal age distribution with a peak at fifth and sixth decades was observed. Details of age and sex distribution are shown in .
Figure 1 Distribution of the patients according to the age and sex.
Regarding predisposing factors, ocular surface disease was most frequently found (48 cases, 69%). Corneal erosion was the most common disease (36 patients), followed by recurrent corneal erosion (3 patients), herpes keratitis (3 patients), bullous keratopathy (2 patients), graft-versus-host disease (2 patients), neurotrophic ulcer (1 patient), and chemical burn (1 patient). Five patients (7%) had a history of previous ocular surgery. Two of those patients had history of cataract surgery, and one patient had history of patch graft surgery due to scleromalacia perforans. One patient had received glaucoma filtration surgery and the remaining one patient had a history of pars plana vitrectomy. Corneal trauma was noted in 15 cases (21%). Four of them had trauma with organic material and five patients had metallic foreign body in cornea. Fourteen of 15 patients with a history of corneal trauma were male patients. CL wear was reported in two cases (3%). Predisposing factors of infectious keratitis are summarized in .
Table 1 Predisposing factors for infectious keratitis
In 15 patients (21%), corneal culture revealed positive results. Twenty-four patients (34%) received treatment with topical antibiotics before referral. Positive culture rate was 17% (4 of 24 cases) in patients with prior treatment with antibiotics, and 24% (11 of 46 cases) in those who did not receive antibiotics treatment. However, no statistically significant difference was found in culture positive rate between the two groups (P=0.554, Fisher’s exact test). shows comparisons of positive culture rates according to previous use of antibiotics.
Table 2 Comparison of positive culture rates according to previous use of antibiotics
Single microorganism was isolated in 14 patients, and two organisms were identified in one patient. Gram-positive bacteria was most common (ten patients, 67%), followed by Gram-negative bacteria (three patients, 20%) and fungi (two patients, 13%). Culture results are summarized in .
Table 3 Causative organisms isolated in cultures of corneal scrapes
Discussion
In the present study, we evaluated clinical features of infectious keratitis including age and sex distribution, predisposition factors, and microbiologic profile.
The age distribution showed single peak in patients aged in their 50s and 60s, and only 11% of patients aged <40. The results are inconsistent with the recent studies that demonstrated bimodal age distribution in the young and in the elderly.Citation5–Citation7 CL-related infectious keratitis was only two cases (3%) in this study, which is in discordance with those of the previous studies in Korea that 26%–40% of infectious keratitis was associated with CL wear.Citation13,Citation14 Studies conducted in other countries also demonstrated that 30%–50% cases of infectious keratitis were associated with CL wear, and the incidence is higher in patients aged in their 20s and 30s.Citation7,Citation15 These results could be explained by the fact that Kangwon province is a rural area where proportion of elderly population is higher and only small population of youngsters reside.
In the present study, the proportion of male patients was higher than female patients, which is in agreement with the male preponderance in the elderly reported in another study.Citation16 It is conceivably due to the fact that males are more susceptible to trauma. In this study, 14 of 15 patients with infectious keratitis associated with corneal trauma were male.
The results that ocular surface disease was most common predisposing factor for infectious keratitis correspond well with the previous reports.Citation5,Citation7,Citation16,Citation17 Corneal trauma was the second common predisposing factor. Infectious keratitis after corneal trauma is common in undeveloped countries or rural areas,Citation7,Citation18,Citation19 and decreased with economic development and urbanization.Citation15,Citation19 The relatively high proportion of corneal trauma might be explained by the fact that most of the patients included in this study were the elderly residing in rural areas and live on farming, thus having an increased risk of corneal trauma and exposure to pathogens.
Positive culture rate was 21%, which is lower compared to the results of previous studies that causative microorganism was identified in 40%–68% of cases.Citation1,Citation5–Citation7,Citation9,Citation20,Citation21 Empirical antibiotics treatment, slow growth of microorganisms on culture media, other causes of keratitis including virus and improper corneal sampling might account for the low positive culture rate in this study.Citation8 Patients with prior topical therapy had lower positive culture rate compared to those who did not receive antibiotics treatment before referral, although the difference was not statistically significant. Prior studies demonstrated that empirical use of antibiotics is associated with decreased positive culture rate.Citation1,Citation6 Meanwhile, van der Meulen et alCitation6 showed the rate that culture outcomes affected modification of initial antibiotic therapy was only 4.5%, suggesting the effectiveness of empirical treatment with antibiotics. With the development of antibiotics, such as fourth-generation quinolone including moxifloxacin and gatifloxacin, the effectiveness of empirical treatment with commercially available antibiotics can be enhanced. For instance, Sharma et alCitation22 recently revealed that 0.5% moxifloxacin monotherapy is equally effective as combination therapy using fortified cefazolin and tobramycin in the treatment of moderate bacterial corneal ulcers.
In this study, Gram-positive bacteria were the most frequently identified pathogen, and Staphylococcus species was the most common Gram-positive bacteria, which is in agreement with previous reports.Citation1,Citation7,Citation20,Citation23 By contrast, several recent studies demonstrated high incidence of keratitis caused by Gram-negative bacteria, especially Pseudomonas aeruginosa.Citation5,Citation6,Citation21,Citation24 Prior studies in Korea also reported that Pseudomonas species was the most common pathogen.Citation13,Citation14 The results of the present study are in discordance with those studies, conceivably because of low proportion of CL-related keratitis.
Although this study has a limitation that only a small numbers of patients at one tertiary referral center were included, we believe that this study provides updated data of infectious keratitis in a rural area of Korea, and can be informative particularly regarding infectious keratitis in rural areas. Further studies including larger population are needed for more generalized data.
Acknowledgments
Seung-Jun Lee and Jang Hun Lee share first authorship for this paper.
Disclosure
The authors report no conflicts of interest in this work.
References
- HanSBLimTHWeeWRLeeJHKimMKCurrent characteristics of infectious keratitis at a tertiary referral center in South KoreaJpn J Ophthalmol200953554955119847616
- McLeodSDLaBreeLDTayyanipourRFlowersCWLeePPMcDonnellPJThe importance of initial management in the treatment of severe infectious corneal ulcersOphthalmology199510212194319489098300
- ProkoschVGatzioufasZThanosSStuppTMicrobiological findings and predisposing risk factors in corneal ulcersGraefes Arch Clin Exp Ophthalmol2012250336937422116498
- HallRCMcKellarMJBacterial keratitis in Christchurch, New Zealand, 1997–2001Clin Experiment Ophthalmol200432547848115498058
- GreenMApelAStapletonFRisk factors and causative organisms in microbial keratitisCornea2008271222718245962
- van der MeulenIJvan RooijJNieuwendaalCPVan CleijnenbreugelHGeerardsAJRemeijerLAge-related risk factors, culture outcomes, and prognosis in patients admitted with infectious keratitis to two Dutch tertiary referral centersCornea200827553954418520502
- BourcierTThomasFBorderieVChaumeilCLarocheLBacterial keratitis: predisposing factors, clinical and microbiological review of 300 casesBr J Ophthalmol200387783483812812878
- Chirinos-SaldanaPBautista de LucioVMHernandez-CamarenaJCClinical and microbiological profile of infectious keratitis in childrenBMC Ophthalmol2013135424131681
- FeilmeierMRSivaramanKROlivaMTabinGCGurungREtiologic diagnosis of corneal ulceration at a tertiary eye center in Kathmandu, NepalCornea201029121380138520847686
- GreenMApelAStapletonFA longitudinal study of trends in keratitis in AustraliaCornea2008271333918245964
- GuptaNVashistPTandonRGuptaSKDwivediSManiKPrevalence of corneal diseases in the rural Indian population: the Corneal Opacity Rural Epidemiological (CORE) studyBr J Ophthalmol2015214715225395684
- HenryCRFlynnHWJrMillerDForsterRKAlfonsoECInfectious keratitis progressing to endophthalmitis: a 15-year study of microbiology, associated factors, and clinical outcomesOphthalmology2012119122443244922858123
- HahnYHHahnTWTchahHWEpidemiology of infectious keratitis(II): a multi-center studyJ Korean Ophthalmol Soc2001422247265
- TchahHWKimJCHahnTWHahnYHEpidemiology of contact lens related infectious keratitis (1995.4~1997.9): multi-center StudyJ Korean Ophthalmol Soc199839714171426
- CohenEJFultonJCHoffmanCJTrends in contact lens-associated corneal ulcersCornea19961565665708899267
- KunimotoDYSharmaSGargPGopinathanUMillerDRaoGNCorneal ulceration in the elderly in Hyderabad, south IndiaBr J Ophthalmol2000841545910611100
- KeayLEdwardsKNaduvilathTMicrobial keratitis predisposing factors and morbidityOphthalmology2006113110911616360210
- ParmarPSalmanAKalavathyCMKaliamurthyJThomasPAJesudasanCAMicrobial keratitis at extremes of ageCornea200625215315816371773
- VajpayeeRBDadaTSaxenaRStudy of the first contact management profile of cases of infectious keratitis: a hospital-based studyCornea2000191525610632009
- YehDLStinnettSSAfshariNAAnalysis of bacterial cultures in infectious keratitis, 1997 to 2004Am J Ophthalmol200614261066106817157596
- MarangonFBMillerDAlfonsoECImpact of prior therapy on the recovery and frequency of corneal pathogensCornea200423215816415075885
- SharmaNGoelMBansalSEvaluation of moxifloxacin 0.5% in treatment of nonperforated bacterial corneal ulcers: a randomized controlled trialOphthalmology201312061173117823415776
- TuftSJMathesonMIn vitro antibiotic resistance in bacterial keratitis in LondonBr J Ophthalmol200084768769110873974
- TanDTLeeCPLimASCorneal ulcers in two institutions in Singapore: analysis of causative factors, organisms and antibiotic resistanceAnn Acad Med Singapore19952468238298838989