
Abstract
Solid pseudopapillary neoplasm (SPN) is a rare tumor of the pancreas that tends to grow silently in patients at a young age, to a large size and mass. We report here a case of a small-sized SPN detected incidentally in a 12-year-old girl following a traffic accident. The tumor was 3.5 cm in maximal diameter and was found to have hemorrhagic necrosis without a solid component. Laparoscopic spleen-preserving distal pancreatectomy was performed which cured the patient. SPN is generally accepted to be a low grade malignant tumor, but its clinical behavior is sometimes unpredictable. Tumor size and the proportion of solid portion of the tumor have both recently been identified as predictors of malignancy. Although the initial presentation in this case was that of the traffic accident, the subsequent detection of a small, totally cystic SPN, and then the complete eradication of the lesion, led to a favorable outcome for the patient. Long-term monitoring should prevent any chance of recurrence.
Introduction
Solid pseudopapillary neoplasm (SPN) is a low grade malignant neoplasm of the pancreas typically occurring in younger women. Patients with SPN are often clinically asymptomatic and the tumors are not detected by standard imaging modalities until they are large enough to cause symptoms.Citation1,Citation2 We report herein a case of a small SPN detected incidentally after a traffic accident, which nevertheless eventually resulted in a favorable outcome for the patient.
Case report
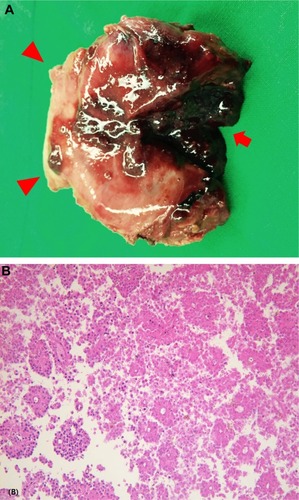
The case review was conducted according to all guidelines outlined in the Declaration of Helsinki. As this study involved no interventional experimentation whatsoever and is a retrospective review of a case, written consent from the patient was not required. A 12-year-old girl presented to the emergency department shortly after a traffic accident with upper abdominal pain. She had been in the passenger seat of the car, wearing a seat belt. She had no associated symptoms such as nausea or vomiting. Her past medical history was unremarkable. On physical examination, the patient had an acutely-ill-looking appearance but her vital signs were within normal ranges. Her abdomen was flat and slightly tender in the upper abdominal region but without signs of peritonitis. There were no identifiable external wounds on her abdomen. On laboratory examination, the white blood cell count was 12,100 cells/uL (normal, 4,000–10,000 cells/uL) with 88% segmented neutrophils, and hemoglobin was 11.6 g/dL (normal, 13.3–16.5 g/dL). Liver function tests were normal. Serum amylase and lipase were 86 U/L (normal, 30–118 U/L) and 33 U/L (normal, 12–53 U/L), respectively. Abdominal computed tomography (CT) scan revealed neither free gas nor blood in her abdomen, but a 4 cm mass was detected in the tail of the pancreas, and the patient was hospitalized for further evaluation of the pancreatic mass. The mass had an enhancing thin wall, and the internal texture was homogeneously cystic without enhancing solid components (). CEA and CA-125 checked after admission were 1.2 ng/mL (normal, 0–5 ng/mL) and 10.9 U/mL (normal, 0–35 U/mL), respectively. On day 2 of hospital admission, the patient underwent a laparoscopic spleen-preserving distal pancreatectomy to rule out malignancy. The tumor was found to be grossly 3.5 cm in maximal diameter, with a fibrous capsule with extensive hemorrhagic necrosis internally (). Pathological examination confirmed the diagnosis of SPN by demonstrating the characteristic pseudopapillae in which residual tumor cells appear to rosette around the vascular cores (). The resection margin was free of tumor cells. The postoperative course was uneventful and the patient was discharged 7 days after the operation. Currently, 6 months postoperative, the patient is well without radiological evidences of disease recurrence.
Figure 1 CT scan of mass in the pancreatic tail region with a homogeneously cystic component with enhancing thin wall (arrows).
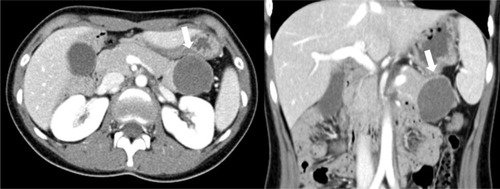
Figure 2 Surgical specimen and microphotograph.
Discussion
SPN is an uncommon pancreatic epithelial tumor that usually occurs in women in the second to fourth decades of life, usually presenting with a tumor size large enough to affect adjacent organs and provoke symptoms such as discomfort and vague abdominal pain.Citation3 In an adult study, the author noted that the mean diameter of the SPN was 10 cm and that the large size could be used as a diagnostic tool for detecting SPNs.Citation4 In a recent pediatric series, the median maximum tumor diameter was 5.5 cm, ranging from 1.8 to 15 cm.Citation5 The patient in this case had no abdominal symptoms before the accident and because the tumor was too small to cause mass-related symptoms, the eventual diagnosis of SPN in this patient would otherwise have been considerably delayed.
SPN is a low grade malignant neoplasm with an excellent long-term outcome after complete surgical excision. Hwang et al found that malignant SPNs tend to be larger than benign tumors (median 10 cm vs median 5 cm) with a greater proportion of solid components (median 88.5% vs 41.5%) at presentation.Citation5 However, it remains contentious as to whether SPNs show malignant transformation as they grow larger or whether those SPNs with innate malignant potential tend to grow more solid and larger. Moreover, there have been exceptional cases showing unpredictable behavior; some patients have shown long-term survival with residual SPN,Citation6,Citation7 while in others aggressive SPN has proved ultimately fatal.Citation8,Citation9 Therefore, to our knowledge, the benign nature shown by most SPNs does not justify or excuse late detection or treatment delay. The patient described here had a small SPN that had no malignant foci and given that long-term monitoring is mandatory for this low grade malignant tumor, the seemingly unfortunate accident experienced by the patient paradoxically resulted in a positive outcome for her.
Treatment of choice for SPN is complete surgical excision, with the actual surgical procedure dependent on the location of the tumor. SPNs can occur throughout the pancreas, but are typically found more frequently in the body or tail regionCitation10 and can be managed by distal pancreatectomy. In children, compared to the adults, less destructive surgery has been advocated and tumor enucleation had been tried in a 16-year-old girl who had SPN in both the head and tail of the pancreas.Citation11 However, contrary to the case reported by Juric et al,Citation11 the patient described here had a single mass at the most distal part of the pancreas and, moreover, concerns on the potential malignant foci led us to consider distal pan-createctomy rather than simple enucleation. With advances in surgical techniques, laparoscopic distal pancreatectomy has proven to be as safe and effective as conventional open surgery.Citation12 As SPNs frequently occur in younger women who are sensitive to cosmetic appearances, minimally invasive surgery could be an excellent alternative in such cases, provided complete tumor removal is guaranteed. Due to the possible occurrence of occult postsplenectomy infection, whether splenectomy is performed should also be considered in the management of SPN of the tail region of the pancreas in pediatric patients. In this case, spleen-preserving laparoscopic distal pancreatectomy successfully treated the patient by excising the tumor while preserving the spleen.
In summary, we successfully treated pancreatic tail SPN in a 12-year-old girl. Owing to the abdominal trauma presentation, the tumor was detected incidentally at an early stage of tumor growth. Laparoscopic spleen-preserving distal pancreatectomy produced the best results both from an oncologic as well as cosmetic aspect. Considering that malignancy is related to the tumor size and the proportion of the solid portion, prognosis of this patient appears promising, but long-term follow-up should be provided.
Disclosure
The authors report no conflicts of interest in this work.
References
- CantisaniVMorteleKJLevyAMR imaging features of solid pseudopapillary tumor of the pancreas in adult and pediatric patientsAJR Am J Roentgenol2003181239540112876017
- ChoiJYKimMJKimJHSolid pseudopapillary tumor of the pancreas: typical and atypical manifestationsAJR Am J Roentgenol20061872W178W18616861508
- JiangLCuiLWangJChenWMiaoLJiaJSolid pseudopapillary tumors of the pancreas: findings from routine screening sonographic examination and the value of contrast-enhanced ultrasoundJ Clin Ultrasound201543527728225502923
- ChoiBIKimKWHanMCKimYIKimCWSolid and papillary epithelial neoplasms of the pancreas: CT findingsRadiology198816624134163336716
- HwangJKimDYKimSCNamgoongJMHongSMSolid-pseudopapillary neoplasm of the pancreas in children: can we predict malignancy?J Pediatr Surg201449121730173325487471
- ZinnerMJShurbajiMSCameronJLSolid and papillary epithelial neoplasms of the pancreasSurgery199010834754802396191
- NishiharaKNagoshiMTsuneyoshiMYamaguchiKHayashiIPapillary cystic tumors of the pancreas. Assessment of their malignant potentialCancer199371182928416730
- van den AkkerMAngeliniPTaylorGChamiRGerstleJTGuptaAMalignant pancreatic tumors in children: a single-institution seriesJ Pediatr Surg201247468168722498381
- MartinRCKlimstraDSBrennanMFConlonKCSolid-pseudopapillary tumor of the pancreas: a surgical enigma?Ann Surg Oncol200291354011833495
- ColemanKMDohertyMCBiglerSASolid-pseudopapillary tumor of the pancreasRadiographics20032361644164814615569
- JurićIPogorelićZStepanJGKuzmićIPExtremely rare presentation of Frantz’s tumour: synchronous localisation in the pancreatic head and tailScott Med J2014593e8e1225035290
- VelanovichVCase-control comparison of laparoscopic versus open distal pancreatectomyJ Gastrointest Surg2006101959816368497