
Abstract
Background
Parenteral nutrition (PN) therapy is a complex and critical therapy that requires special clinical knowledge, skills, and practice experience to avoid errors in prescribing, compounding, and clinical management of patients. Pharmacists with adequate clinical training and expertise in PN therapy can have pivotal role in the care of patients receiving PN therapy.
Objective
The aim of this systematic review was to describe and evaluate the different roles of pharmacists and their provided services related to PN therapy.
Materials and methods
A comprehensive systematic literature review on the topic was conducted via PubMed database using several keywords related to the topic (from 1975 to 2017). Additional resources included the standards of practice and clinical guidelines from recognized organizations such as the American Society for Parenteral and Enteral Nutrition (ASPEN) and the American Society of Health-System Pharmacists (ASHP).
Results
Pharmacists have diverse roles in relation to PN therapy including the following: the assessment of patients’ nutritional needs; the design, compounding, dispensing, and quality management of PN formulations; monitoring patients’ response to PN therapy; supervision of home parenteral nutrition (HPN) programs; education of patients, caregivers, and other health care professionals on nutrition support and conducting PN-related research and quality improvement activities. These services seem to be variable across clinical settings and among different countries depending on the practice environment and pharmacists’ clinical practice in these settings. However, each of these practice domains helps to support the delivery of safe and effective PN therapy to patients.
Conclusion
Pharmacists have been actively participating in providing PN-related services to patients. To fulfill the requirements of their essential role in this area of practice, pharmacists need adequate educational preparation and clinical training on nutrition support. Empowerment of pharmacists to assume a stronger leadership role in this dimension of pharmacy practice will enhance the quality of care provided to patients receiving PN therapy and improve PN services.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Introduction
Parenteral nutrition (PN) therapy involves the intravenous administration of nutritionally sufficient and balanced formulations to supply essential nutrients to patients who are unable to tolerate oral or enteral feeding due to dysfunctional or inaccessible gastrointestinal (GI) tract. Over the years, PN has become an important primary and adjunctive therapy in various clinical conditions and disease states for both the acutely ill hospitalized patients and in the long-term setting for selected patients in the home.Citation1,Citation2 For example, PN formulations can serve as a life-sustaining option for premature infants and critically ill hospitalized patients and for patients who have permanent loss of the GI tract such as those with fistulas or short bowel syndrome.Citation3,Citation4
When all the daily nutritional requirements are exclusively supplied to the patient by PN formulations, the therapy is called total parenteral nutrition (TPN). In terms of their composition, PN formulations can either be of standard composition or tailored to the patient’s individual needs. Although standard PN formulations have been increasingly supplied by industry in some countries,Citation5,Citation6 PN formulations are still compounded in-house by pharmacy staff within the hospital pharmacies to cover patients’ needs in many countries.Citation7
The PN formulations are complex admixtures that consist of multiple components, including both macronutrients (amino acids, dextrose, and intravenous fat emulsions [IVFEs]) and micronutrients (electrolytes, vitamins, and trace elements). In view of the complexity of their composition and direct administration into the blood stream, these formulations must be sterile and contain stable and compatible components to ensure the safety of patients receiving PN therapy.Citation1,Citation8,Citation9 An incompatible, unstable, or contaminated intravenous infusion may result in harm to patients, including serious morbidity and even mortality.Citation10 Therefore, PN formulations must be compounded under strict aseptic techniques according to validated pharmaceutical compounding procedures.Citation1,Citation11,Citation12
Although being lifesaving for many patients, PN therapy is a high-risk feeding modality that can be associated with some complications.Citation4,Citation13,Citation14 In the initial stages of PN therapy, electrolyte imbalance is usually the most common acute PN-related complication.Citation13 In the long-term PN therapy, line complications such as line sepsis and occlusion, pulmonary embolism, and metabolic complications such as glucose intolerance, cholestatic liver disease, and micronutrients deficiencies/toxicity may occur.Citation13 Another potential complication of PN therapy is the refeeding syndrome which results from feeding after a period of prolonged starvation.Citation15 This can result in serious biochemical disturbance including a dramatic fall in phosphate levels with subsequent symptoms and signs of deterioration that may lead to death if not recognized and managed properly.Citation13,Citation15 In addition to these potential complications, supporting patients’ survival through the venous administration of nutrients is an expensive form of nutrition support.Citation4
Pharmacists have unique constellation of competencies, including clinical knowledge and skills which place them in an ideal position to contribute to the delivery of nutrition support therapy to patients. Indeed, the professional roles of pharmacists have been evolving from the traditional compounding and dispensing of medications to the modern delivery of direct patient care within multidisciplinary health care teams. Pharmaceutical care (PC) is a practice philosophy, in which the pharmacist responsibly provides medication therapy to patients to achieve definite outcomes that improve their quality of life.Citation16,Citation17 There is cumulative evidence to support the positive impact of PC on patient careCitation17 and health care costs.Citation18,Citation19
To adequately provide PC services, pharmacists must collaborate with other health care professionals and the patient in the design, implementation, and monitoring of a therapeutic plan to optimize patient’s clinical outcomes.Citation17,Citation19 Therefore, the effective execution of PC practice would require good collaboration between pharmacists and the other members of the health care team to optimize patients’ therapeutic outcomes. Likewise, PN therapy is optimally provided to patients as a multidisciplinary service in which the pharmacist collaborates with other health care professionals to optimize a patient’s nutrition care plan.Citation20,Citation21 Nutrition support team (NST) is an interdisciplinary team often composed of physicians, dieticians, pharmacists, and nurses who have specialty training in nutrition support with the responsibility to manage PN therapy following carefully designed protocols.Citation14,Citation22 Pharmacist provision of patient-oriented PC services to patients receiving PN therapy has been shown to improve the clinical outcomes of patients.Citation23,Citation24 Therefore, PN therapy presents an ideal avenue for the pharmacist to contribute as an active member of a multidisciplinary health care team in the provision of safe and effective nutritional and medical therapy to patients.
Development of nutrition support in clinical pharmacy
Most of the developmental milestones in pharmacy nutrition support were achieved in the USA. In 1968, Dudrick et alCitation25 from the Hospital of University of Pennsylvania managed to nourish beagle puppies into full grown dogs by infusing nutrients through central venous access. Shortly after that, the therapy was initiated in infants with debilitating diseases or GI deformities, and then it was administered to adults. Stanely Serlick was the pioneer in pharmacy nutrition support as he managed to prepare sterile, stable, and compatible mixtures of nutrients that could be infused intravenously.Citation26 By the early 1970s, commercial PN products were available and physicians were using the therapy in managing patients who required PN throughout the USA.Citation27 As a result, there was a growing need to initiate a sophisticated system for ordering, preparing, and administering PN therapy with an increased attention to the development of measures to avoid PN metabolic and catheter-related complications.Citation26 Since that early time, the interdisciplinary NSTs emerged as the preferred mode for the safe delivery of PN therapy and the pharmacists began to develop their knowledge and expertise in nutrition support.Citation26,Citation28 Their roles have been expanding beyond the preparation of the sterile, stable, and compatible PN admixtures to the clinical management of PN patients, as well as to PN-related research activities and safety improvement.Citation26 In 1978, the American Society for Parenteral and Enteral Nutrition (ASPEN), which represents an interdisciplinary society of physicians, nurses, dieticians, pharmacists, and nonclinical researchers, was established with a mission to optimize nutrition support of patients during hospitalization and throughout recovery.Citation26
The following two decades witnessed several advancements in PN therapy, such as the development of home parenteral nutrition (HPN) programs, improved quality of manufacturing macronutrients including amino acids and IVFE, advances in disposable administration devices, and introduction of automated compounding machines which enhanced the safety and precision of PN admixture compounding.Citation2,Citation26 Prior to that landmark achievement, the historical method of compounding these multicomponent admixtures was to manually use gravity-driven transfers for large volume additives, such as amino acids, dextrose, lipids, and sterile water, and to add small volume additives, such as electrolytes, trace minerals, multivitamins, and drugs using syringes.Citation29 The manual method used to be labor intensive and required multiple manipulations of infusion containers, sets, syringes, and needles which can lead to poor accuracy of the compounding process and possible contamination of the final admixture.Citation29 The evolution of automated compounding technology for PN admixture compounding with the aid of fluid pump technology and software that controls the compounder pump has led to potentially improved compounding accuracy and PN safety.Citation26,Citation29 It also reduced the time required to compound PN formulas and simplified the process of tailoring their composition to suit individual patient’s needs.Citation26
In an attempt to achieve the best PN outcomes, there has also been increasing clinical research related to the proper use of PN in different clinical conditions and the management of PN-related complications.Citation26 As the pharmacists’ role in nutrition support evolved, ASPEN published standards for nutrition support pharmacists (NSPs) in 1987.Citation30 These standards were defined by ASPEN as a “benchmark representing a range of performance of competent care that should be provided to assure safe and efficacious nutrition care”.Citation31 A year later, the Board of Pharmaceutical Specialties (BPSs) recognized NSPs as specialists.Citation32 Collaborative efforts by ASPEN, the American Society of Health-System Pharmacists (ASHPs), and other organizations came to fruition with the development of Nutrition Care Standards by the Joint Commission on Accreditation of Health Care Organizations (JCAHO).Citation33 These standards mandated the implementation of interdisciplinary nutrition care process and started to be surveyed in 1995.Citation33 Since PN is considered as a high-alert medication, ASPEN in partnership with ASHP created a task force to develop safe practices for PN which were first published in 1998 and revised in 2004.Citation1,Citation34 These clinical guidelines include consensus recommendations to support safe practices related to PN ordering, labeling, compounding, administration, and quality control.
Roles of NSPs
In many developed countries, especially in North America and Europe, nutrition support pharmacy has been growing as a specialty in clinical pharmacy practice. The NSPs are trained and competent to provide several beneficial services related to PN therapy. Depending on their practice environment, their scope of practice may include, but it is not limited to the following: providing direct patient care to patients; consultations with other health care professionals including those in entrepreneurial/industry; supervision of the compounding and dispensing of PN formulations; education of patients, caregivers, students, postgraduate trainees, colleagues, and the public; and contribution to research activities and quality improvement related to nutrition support.Citation21 Moreover, they can have administrative functions such as the management of nutrition support services in their institutions including development, documentation, implementation, and periodic review of organizational policies, procedures, and protocols related to nutrition support and the selection and review of suitable and cost-effective nutrition support formulary.Citation21
Materials and methods
This systematic review outlines the various services that pharmacists can provide in relation to the delivery of PN therapy. A comprehensive literature review on the topic was conducted using different combinations of keywords including the following: parenteral nutrition, total parenteral nutrition, nutrition support, nutrition support pharmacist, clinical pharmacy practice, clinical pharmacist, pharmacist, intensive care unit (ICU), adults, and neonates. References were resourced in the literature indexed in PubMed database during the period from 1975 to 2017 and were accessed via the Health Sciences Center Library at Kuwait University.
The references used in this review were articles describing pharmacists’ role in PN therapy including clinical studies, review articles, and position statements related to pharmacists’ role in PN from recognized organizations such as ASPEN and ASHP. References were included in the final review only if the article focused on an area of pharmacy practice related to PN therapy, and/or the article reported pharmacists’ involvement in PN therapy and/or an intervention or assessment of PN-related services by pharmacists or comparison between services. Results were mainly full articles published in English. Due to the paucity in the literature describing pharmacists’ role in PN therapy, the abstracts of some studies published in other languages were also evaluated for evidence.
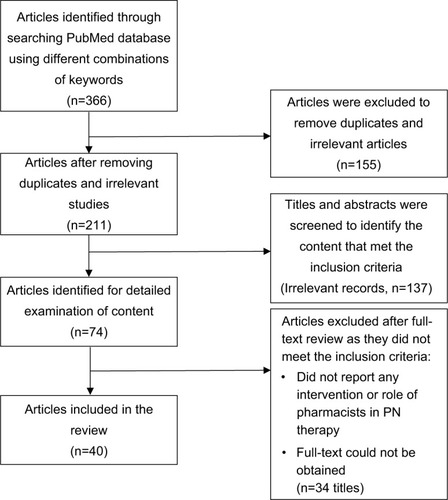
The review process initially identified all article titles and abstracts related to the topic which were reviewed to exclude duplicates and irrelevant articles. The titles and abstracts were then examined to determine the relevant articles that would be suitable for detailed examination. The next review cycle involved evaluating the remaining full articles to identify the content that met the inclusion criteria and exclude irrelevant articles. The articles were excluded from the final review if they were not reporting any intervention or involvement of the pharmacist in PN therapy or the full text could not be obtained. These articles were evaluated for content and subsequently classified according to the type of service provided by pharmacists in relation to PN therapy and the scope of pharmacists’ practice for that service. outlines the flowchart of the study selection process.
Figure 1 Flowchart of the study selection process.
Results
Pharmacists have diverse roles in relation to PN therapy including the assessment of patients’ nutritional needs; the design, compounding, dispensing, and quality management of PN formulations; developing and implementing of an individualized nutrition care plan and monitoring patients’ response to PN therapy. Other areas of pharmacists’ practice in relation to PN include supervision of HPN programs; education of patients, caregivers, and other health care professionals on nutrition support; and conducting PN-related research and quality improvement activities. Each of these practice domains helps to support the delivery of safe and effective PN therapy to patients. illustrates the different roles of pharmacists in relation to PN therapy. summarizes the key findings of the relevant studies that were included in this review.
Figure 2 Pharmacists’ different roles in relation to PN therapy.
Table 1 Identified studies describing pharmacists’ involvement and/or interventions in relation to PN therapy
Pharmacists’ role in nutrition assessment and PN prescribing
The PN formulations must meet the nutritional requirements of the patient according to patient age, energy expenditure, and clinical status to ensure that the appropriate nutrients are provided to patient and to avoid under- or overnutrition.Citation1 The ASPEN’s standards of practice for NSPs state that the NSP providing direct patient care should participate in nutrition assessment of patients in collaboration with other health care professionals to identify patients who are at risk for malnutrition.Citation21 The assessment is based on retrieving patient history through patient/caregiver interview, reviewing the patient’s medical record and evaluating nutrition-focused physical and biochemical assessment parameters.Citation21,Citation35 The NSP shall participate in the routine assessment of the patient’s energy, protein, fluid, vitamin, mineral, and electrolyte requirements according to age, clinical conditions, and medical therapy and in the assessment of patients’ candidacy for nutrient support.Citation21,Citation35 The NSP should participate in assessing the educational needs of patients, caregivers, health care professionals, and others regarding nutrition support therapy.Citation21
The literature search revealed variable levels of pharmacists’ involvement in nutrition assessment and PN prescribing processes. However, the leading role of pharmacists in PN prescribing was described as early as the late 1970s.Citation36 Green-lawCitation36 reported that the physician requested a consultation with the pharmacist to initiate PN therapy in a TPN program applied in a private nonteaching institution. The pharmacist was responsible for conducting the needed physical and nutrition assessment of the patient and writing all the TPN-related orders, with a resulting increase in the utilization of PN therapy and the physicians relying on pharmacists for this service.Citation36
To prepare pharmacists for this role, adequate training was necessary, and a number of studies reported training of pharmacists on PN prescribing. For example, FaberCitation37 described the development and implementation of an education and training program at a community hospital to enable staff pharmacists to become involved in the pharmacy-based TPN service and to write TPN orders and conduct TPN rounds. McDermott et alCitation38 reported that training efforts were made to increase pharmacists’ involvement in nutrition support and physician prescribing at their institution. The increased involvement of pharmacists in the prescribing process resulted in more appropriate PN therapy, earlier shift from PN to enteral nutrition, acknowledging pharmacists as resources for physicians, and improved job satisfaction for pharmacists.Citation38 In another study, Broyles et alCitation39 reported the positive impact of pharmacists’ interventions on improving fluid balance in fluid-restricted ICU patients receiving PN. There is also available evidence to support pharmacists’ participation in nutrition consultations with physicians in different settings.Citation40,Citation41
Ragab et alCitation3 conducted a literature review on pharmacist’s role as a prescriber for PN therapy as related to pharmacy practice. Their review revealed that the practice of pharmacist writing neonatal PN orders already exists, but seems to be limited compared to pharmacists’ role in writing adult PN orders which is more established in many countries.Citation3 Nevertheless, they concluded that there is sufficient evidence to support pharmacists’ competencies in this area of practice.Citation3
As part of the process of revision of ASPEN’s safe practices for PN guidelines, Seres et alCitation42 conducted a web-based survey among ASPEN members to gain insight into PN practices including the processes for writing PN orders. Their findings showed that in general physicians (78%) were responsible for writing PN orders, but the dietitians and pharmacists were heavily involved in the order-writing process either as individuals or as members of a nutrition support service.Citation42 Moreover, pharmacy staff were allowed to adjust certain electrolyte additives such as acetate or chloride in 62% of respondents’ organizations.Citation42 In another web-based survey of PN practices in the USA by Boullata et al,Citation43 28.3% of respondents reported that a pharmacist was prescribing PN at their settings. Similarly, Yang et alCitation44 reported pharmacists’ involvement in confirming and adjusting the daily caloric content in the PN and enteral feeding orders of very low birth weight neonates receiving PN therapy. In another study, the specialty practice pharmacist was responsible for supervising the PN system throughout the entire health care system, while the unit-based pharmacist was responsible for the initiation and daily management of PN together with the primary service physicians.Citation45 Pharmacists delivered nutrition support services have been proven to result in appropriate PN prescribing and a decline in the non-indicated use of PN.Citation38,Citation46
Pharmacists’ role in developing and implementing the nutrition care plan
The ASPEN’s standards of practice for NSPs state that the NSP shall participate in developing a customized nutrition care plan for the patient in collaboration with other health care professionals.Citation21,Citation35 This plan shall be based on the patient’s nutrition assessment, disease states, clinical conditions, and nutritional risk factors and shall include evidence-based literature.Citation21 While developing this plan, the NSP shall review patient medications to determine their impact on the nutrition care plan and nutrient requirements.Citation21 Other responsibilities of the NSP include the documentation of the nutrition care plan in the medical record, recommending the preferred route of administration of nutrition support therapy, recommending a patient-specific feeding formulation, rate of administration, and mode of administration based on the patient’s clinical information.Citation21,Citation35 Moreover, the NSP should recommend suitable medical therapy adjuncts to nutrition support therapy if needed.Citation21 The NSP shall contribute to the implementation of the nutrition care plan to enhance appropriateness, safety, accuracy, resources’ efficiency and the delivery of fiscally responsible care.Citation21,Citation35 The NSP should recommend the necessary equipment and supplies and recommend strategies for the prevention, detection, and management of complications related to the feeding formulation(s) and feeding access device(s). The NSP shall also provide strategies for the prevention, detection, and management of interactions between drugs, dietary supplements and nutrients, and strategies to avoid the incompatibility or instability of the feeding formulations.Citation21,Citation35 The NSP should communicate the individualized nutrition care plan with other health care professionals within and outside the institution to promote continuity of care.Citation21,Citation35 One of the chief responsibilities of NSP is to provide appropriate education for the patients and caregivers regarding the nutrition care plan, for which they should develop written educational materials appropriate for the educational needs of the intended audience.Citation21
As there has been a transition in pharmacy practice toward the provision of direct patient care services, the evidence on pharmacists’ participation in the development and management of nutrition care plans has been emerging in the literature. Gales and RileyCitation47 reported a multidisciplinary consult-based NST including a pharmacist with direct interventions in the nutrition care plan in a large private tertiary care institution. The collaborative care provided by the NST resulted in more adequate nutrition care for patients and less metabolic complications compared to TPN therapy solely guided by a physician.Citation47 Another study showed that pharmacist-led nutrition support service resulted in a decline in the incidence of metabolic and electrolyte abnormalities in the patients receiving PN.Citation46 A clinical pharmacist-based nutrition support service has also been found to improve the nutritional status and clinical outcomes of patients undergoing hematopoietic stem cell transplantation.Citation48 Accordingly, Mirtallo and SacksCitation49 proposed a paradigm move in pharmacy nutrition support practice to extend pharmacists’ role beyond PN and drug–nutrient interactions to become partners in the interdisciplinary approach to the implementation and monitoring of nutrition care plans.
A number of studies highlighted the specialized expertise of pharmacists in managing the medication-related changes associated with PN therapy. Giancarelli and Davanos documented several pharmacists delivered medication-related interventions in patients receiving PN therapy with a high overall acceptance rate by physicians. Some reports in the literature describe pharmacists’ role in the prevention, identification, and resolution of medication-related problems and PN complications in these patients with improved patient outcomes.Citation23,Citation24,Citation50 These studies collectively provide evidence on the unique qualifications and perspectives of the pharmacists and potential areas in which pharmacists can educate the health care team and ensure proper medication use in this patient population.Citation46,Citation50
Pharmacists’ role in compounding PN formulations
In many developed countries, the safe practices for compounding and labeling PN admixtures have been well established.Citation1,Citation34 This is evident by the development of standards and practice guidelines that adequately govern these processes. The ASPEN’s standards of practice for NSPs state that NSP shall participate in the development, implementation, and adherence to policies and procedures related to the PN order verification process, PN order review process, and compounding safe and effective PN admixtures.Citation21,Citation35 Their duties shall also include participation in developing, implementing, and adhering to procedures for the detection and prevention of compatibility or stability problems associated with PN admixture during the compounding process.Citation21 Obviously, pharmacists possess unique knowledge and skills in compatibility and stability as related to the PN formulations (e.g., calcium phosphate solubility, total nutrient admixture stability, and co-infusion of other medications with PN).Citation51 In addition, NSP shall participate in developing, implementing, and adhering to quality control procedures related to compounding PN admixtures and policies and procedures related to labeling, delivery, and storage of PN admixtures prior to administration.Citation21
The NSP should participate in training other pharmacists who verify and review PN orders and shall be involved in developing a competency-based educational curriculum for compounding PN admixtures and performing PN-related calculations. This includes training and monitoring pharmacy personnel regarding compounding PN admixtures and assessing their ability to perform the necessary calculations.Citation21
The ASHP issued guidelines for the safe use of automated compounding devices for the preparation of PN admixtures and for quality assurance for pharmacy-prepared sterile products.Citation11,Citation29 The guidelines state that pharmacists are specifically trained and legally responsible for performing extemporaneously compounding parenteral formulations, including PN admixtures.Citation29 The ASHP guidelines indicate that PN admixture compounding should be performed under the direct supervision of a pharmacist and in the appropriate environment.Citation11 The guidelines also stress on the need for specific training of pharmacists, as well as other pharmacy personnel in the operation, maintenance, and quality assur ance of the automated compounders and on performing periodic competency assessment on these responsibilities.Citation29
Preparation of PN solutions has been reported as only one component of pharmacists’ role on the nutrition team and the pharmacists’ clinical responsibilities in managing and monitoring patients receiving PN have long been well established in developed countries.Citation52 A cross-sectional study describing hospital pharmacists’ PN practices in Switzerland, France, and Belgium demonstrated the unique role of pharmacists in compounding PN formulas in hospital pharmacies as well as their participation in NST services.Citation53 On the other hand, pharmacists’ role in PN therapy in many developing countries seems to be still limited to compounding PN admixtures. For example, Batani et alCitation54 explored TPN practices in Universiti Sains Malaysia Hospital, Malaysia, and reported that pharmacists were merely responsible for compounding PN formulations and for the logistical aspects and integrity of the PN product lines. They identified high response rate of TPN-associated complications, especially in the electrolyte complications with a rate (56.5%) that seems to be higher compared to that reported in developed countries.Citation3 Since pharmacists were only responsible for PN compounding in that study, this highlights the value of pharmacist monitoring of patients’ response to PN therapy to reduce the incidence of the metabolic and electrolyte complications as have been demonstrated in studies conducted in many developed countries.Citation3,Citation46,Citation47 Likewise, Katoue et alCitation7 explored TPN practices at hospital pharmacies in Kuwait. They reported that pharmacists were mainly performing technical roles such as PN order verification, PN compounding, and maintaining PN necessary supplies with limited clinical roles in providing direct patient care services.Citation7,Citation55 The pharmacists attributed their limited involvement in providing PC services to several professional and organizational barriers.Citation55
Pharmacists’ role in monitoring patients on PN therapy
PN is a highly complex, therapeutic intervention, and patients receiving this therapy must be under close monitoring to avoid PN-related complications.Citation13,Citation14 It is important and specific to the role of the pharmacist to monitor the patient’s metabolic profile during PN therapy to early detect any feeding-related complications and prevent them from progressing to clinically significant disorders.Citation2 The ASPEN’s standards of practice for NSPs state that the NSP shall monitor patients receiving nutrition support through reports or patient visits, as appropriate in collaboration with other health care professionals.Citation21,Citation35 The NSP shall determine the appropriate monitoring parameters consistent with the patient’s nutrition care plan to optimize therapy and achieve best outcomes.Citation21 The NSP should routinely reassess the appropriateness of nutrition support therapy (e.g., feeding formulation, route of delivery, and delivery method) and evaluate the efficacy and safety of nutrition support therapy by using relevant monitoring parameters.Citation21,Citation35 Patient monitoring must also include careful review of the patients’ concurrent medications to avoid significant drug-induced metabolic disorders.Citation2 Monitoring the levels of vitamins and trace elements in patients requiring specialized nutrition support is important and represents another area that can highlight the unique skills of pharmacists with additional nutrition support training.Citation13,Citation46
Undoubtedly, patients receiving long-term PN can greatly benefit from the experience and help of NSTs, so that the complications can be detected and managed promptly.Citation13 Dodds et alCitation14 performed retrospective analysis of a previously maintained NST database to identify the frequency of metabolic occurrences in hospitalized patients receiving TPN and managed by an NST. Their data showed that only 13 symptomatic events occurred in 11 patients in 2747 courses of TPN over 7 years (0.47%).Citation14 Early recognition and prompt management of each of these events avoided long-term complications and patients’ death.Citation14 This supports the positive impact of nutrition support service on avoiding serious metabolic complications in hospitalized patients receiving TPN.
Pharmacists’ participation in monitoring patients receiving PN therapy has long been proven to reduce costs and improve patients’ clinical outcomesCitation38,Citation56,Citation57 and to prevent and resolve complications.Citation36 Mutchie et alCitation56 compared the outcomes of patients who received standard TPN solutions without pharmacist monitoring to the outcomes of patients whose TPN therapy was individualized and monitored by a pharmacist. Their findings revealed that pharmacist monitoring of patients receiving PN therapy resulted in improved patients’ clinical responses to TPN and reduced TPN-related costs.Citation56 Similarly, Dice et alCitation57 demonstrated that pharmacist monitoring of an individualized TPN in neonates resulted in a greater amount of nutrients to be provided and mean daily weight gain and was more cost-effective compared to the use of standardized TPN solutions without pharmacist monitoring. A report by Muller et alCitation52 highlights the primary role of the pharmacist in monitoring the laboratory results of cancer patients receiving PN therapy and monitoring the medications that patients receive along with PN therapy. They recommended careful monitoring of the clinical status of these patients since medications and other treatment modalities can markedly influence the nutritional status and electrolyte balance in this patient population.Citation52
Pharmacists’ role in HPN programs
Following the establishment, recognition, and reimbursement of PN therapy for hospitalized patients, consideration for payment for patients receiving therapy at home was sought and financially supported in the USA.Citation26 This lead to the development of HPN programs supported by advancements in home infusion therapy industry.Citation26 This has been found to be a useful alternative to improve nutrition in many patients especially those with short bowel syndrome, promote rehabilitation at home, and decrease long-term expenses compared to in-hospital PN therapy.Citation58,Citation59
To adequately provide HPN to patients and to guarantee the quality of service being provided, ASPEN published standards of practice for home nutrition support and ASHP published guidelines on the pharmacists’ role in home care.Citation60,Citation61 This was followed by home care accreditation program by the JCAHO which was the first to use pharmacists as surveyors, educators, and consultants.Citation26 The JCAHO’s home care standards advocated the clinical management of patients by pharmacists.
Several reports in the literature document pharmacists’ involvement in the care of patients receiving HPN therapy. Gaffron et alCitation58 described the organization and operation of HPN program at their hospital, in which the care was coordinated by a multidisciplinary team with a central role of the pharmacist in delivering this service to patients. Pharmacists were involved in patients’ education, provision of in-service training to nurses and house officers, coordination of patients’ transition to home care, testing and evaluating the equipment, development of a training manual, and editing a quarterly newsletter to patients on HPN.Citation58 Similarly, Lees et alCitation59 described pharmacists’ participation in patients training on HPN as part of a multidisciplinary team. Karnack et alCitation62 conducted a national survey in the USA to investigate pharmacists’ role in HPN programs and documented their involvement in the preparation of PN solutions, patient education, and monitoring patients’ laboratory results in collaboration with physicians. There has also been some published literature describing pharmacists’ fundamental role in the care of patients receiving HPN from several countries including Kuwait, Japan, and Poland.Citation55,Citation63,Citation64
Role of pharmacists as members in NSTs
The leadership role of pharmacists in NSTs is well established.Citation36,Citation46 There is considerable evidence to demonstrate the unique perspectives of pharmacists on NSTs and their valuable contribution to the delivery of effective and safe PN therapy.Citation14,Citation36,Citation46 It has been evident that the care provided to patients by multidisciplinary NSTs involving pharmacists results in fewer metabolic and catheter-related complications compared to the care provided by a single physician.Citation28,Citation47,Citation49 Several studies described pharmacists’ involvement in patient education and training on HPN programs as part of multidisciplinary NSTs with improved quality of care and cost-effectiveness of HPN.Citation58,Citation59,Citation64
Pharmacists’ role in management, quality improvement, and research related to PN
According to the Board Certified Nutrition Support Pharmacist (BCNSP) criteria, management, quality improvement, education, and research related to PN therapy were included responsibilities of pharmacists in addition to the pharmaceutical aspects of PN and clinical management of nutrition support patients.Citation26 The ASPEN’s standards of practice for NSPs state that the NSP should participate in the administrative management of the NST or services in collaboration with other members of the health care team.Citation21 The NSP shall also develop collaborative relationships with health care professionals, students, postgraduate trainees, patients, and caregivers and should provide them with nutrition-related education. The NSP should participate in collaborative nutrition-related research activities and shall apply their findings and the best available evidence into practice.Citation21
There have been some reports in the literature which describe some activities and initiatives by pharmacists to improve their practices and PN services. For example, in one study, the pharmacy services evaluated the quality of PN program applied in one hospital in Spain.Citation65 Harbottle et alCitation66 reported the findings of a clinical audit to evaluate PN use in Guernsey. Boitano et alCitation67 reported a quality improvement collaboration to improve the safety and effectiveness of PN at their hospital which resulted in positive impact on the quality and cost of PN services as a result of implementing a set of process improvement strategies. McDermott et alCitation68 described their experience in initiating a documentation system of clinical interventions in nutrition support with the aim to improve the workflow and quality of PN service. With regard to pharmacists’ role in the management of PN services, MartinCitation69 highlighted the important role for consultant pharmacists in nutrition management in long-term care facilities.
Pharmacist’s specialization in nutrition support and continuing professional development (CPD)
As the pharmacy profession has been developing over the years, specialization was a logical outcome of this development. Specialization allowed those pharmacists with special clinical knowledge and skills to meet more in depth or more specific patient care needs.Citation70 In 1988, the BPS recognized NSPs as specialists, thereby defining the scope of practice and the criteria for clinical competence for a pharmacist practicing in nutrition support.Citation32 This certificate is provided to those pharmacists with adequate clinical experience in this area of practice and following rigorous assessment process to evaluate their clinical competencies in the broad area of nutrition support including PN therapy to become recognized as BCNSPs.Citation71 A number of authors described and evaluated the NSP board certification process.Citation70,Citation72,Citation73
The Certified Nutrition Support Clinician® (CNSC®) credential is another certification available for physicians, dietitians, pharmacists, physician assistants, and nurses who are involved in nutrition support.Citation74 It is offered by the National Board of Nutrition Support Certification (NBNSC) which is an independent credentialing board established by ASPEN in 1984.Citation74
Several professional organizations in the field of clinical nutrition also provide education, training, and CPD programs for pharmacists practicing in nutrition support in an effort to improve their practices. The European Society of Clinical Nutrition and Metabolism (ESPEN) offers a postgraduate qualification in clinical nutrition called the Life Long Learning (LLL) Program in Clinical Nutrition and Metabolism for medical doctors and other health care specialists.Citation75 In this program, participants attend training online and at live courses, using several modern training methodologies and resources to provide them with adequate clinical experience in the field of nutrition support.Citation75 Similarly, ASPEN provides wealth of educational resources and learning opportunities for pharmacists on topics related to clinical nutrition including webinars series, online courses, self-study programs, and conferences.Citation76 In addition, some reports in the literature describe individual institutional efforts to conduct staff development programs for the education and training of pharmacists on PN support.Citation37,Citation38
Discussion
The literature presented in this review provides evidence to support pharmacists’ different roles and provided services in relation to PN therapy. These services include the nutrition assessment of patients and PN prescribing; developing and implementing the nutrition care plans; compounding and quality management of PN formulations and monitoring patients on PN therapy. Other areas of pharmacists’ practice included supervision of HPN programs; participation as members of NSTs; management of PN services and conducting PN-related research and quality improvement activities. Each of these practice domains helps to support the delivery of safe and effective PN therapy to patients. Nevertheless, it seems that the extent of pharmacists’ involvement in providing these services is variable across clinical settings and among different countries depending on the practice environment and pharmacists’ clinical practice in these settings. The clinical roles of pharmacists in providing direct patient care to patients requiring PN therapy are well established and documented in developed countries.Citation23,Citation24,Citation46,Citation47,Citation52 Pharmacists practicing in nutrition support in these countries often collaborate with the other members of NST in the assessment of patient’s nutritional needs, development and implementation of an individualized nutrition care plan for the patient, and monitoring patient’s response to PN therapy. On the other hand, pharmacists’ roles in many developing countries are still limited to performing technical tasks such as the compounding, dispensing, and quality control of PN formulations with limited role in providing direct patient care services.Citation7,Citation54,Citation55
The participation of pharmacists in the provision of TPN services has been described in the literature since the late 1970s and early 1980s.Citation36,Citation52,Citation56,Citation57 As there has been a paradigm shift of pharmacy practice from the provision of product-oriented services to the delivery of direct patient care, pharmacists’ practices related to PN therapy have been undergoing similar change as well. Pharmacists have been expanding their role beyond the preparation of PN admixtures to the clinical management of patients while practicing either as individuals or as part of NST services, therefore, emphasizing the philosophy of PC practice. The pharmacists can have clinical responsibilities which are of paramount importance such as following patient laboratory results and monitoring the impact of adjective medications on the nutrition care plan and nutrient requirements.Citation21,Citation52 Many patients receiving PN therapy are critically ill hospitalized patients, and they would be receiving multiple medications along with PN therapy. Being drug experts, pharmacists can have an essential role in the proper selection and monitoring of these mediations to guarantee optimal usage and avoid any interactions or incompatibility issues between these medications and PN therapy.Citation21,Citation46 Indeed, pharmacists have been shown to contribute effectively to the prevention, detection, and resolution of drug-related problems in patients receiving PN therapy with improved patients’ clinical outcomes.Citation23,Citation24,Citation50 In some vulnerable patient populations such as cancer patients, medications and other treatment modalities (e.g., chemotherapy and radiotherapy) can markedly alter nutritional status and electrolyte balance, which highlights the important function of the pharmacist in following these patients.Citation52 Pharmacist monitoring of neonates receiving PN therapy has also been found valuable for improving their clinical outcomes.Citation57 Overall, the participation of pharmacists in providing direct patient care services to patients receiving PN therapy has been shown to improve patients’ nutritional status and clinical outcomes; to prevent and resolve PN-related complications and to save health care costs.Citation48,Citation56,Citation57
Notably, most of the articles describing pharmacists’ interventions and roles in PN support were retrieved from the USA literature. This highlights a need to conduct more clinical studies evaluating pharmacists’ contributions to this area of practice in other countries, especially in developing countries where pharmacists are striving to establish clinical pharmacy services. The bulk of evidence on the benefits of NSTs on patient care has also been driven mainly from studies conducted in the USA.Citation14,Citation28,Citation46,Citation47 In view of the considerable evidence supporting their positive impact on nutrition support patients,Citation14,Citation28,Citation47 the development of NSTs would be vital to enhance the effectiveness and safety of PN support services. This highlights a need to focus on advocating team approach to the management of patients receiving PN support in other countries and conducting good quality research to evaluate their services in these settings.
Transformation of traditional roles of pharmacists in compounding and dispensing PN admixtures into the clinical management of patients receiving PN therapy obviously offers several advantages but comes with substantial challenges. Pharmacists need adequate education and clinical training on nutrition support to enable them to provide these clinical services to patients. Several credentialing bodies and professional organizations including BPS, ASPEN, and ESPEN provide several certification options and CPD opportunities for pharmacists practicing in nutrition support to guarantee their clinical competence and to demonstrate their accountability for the critical role they play in patient care.
Continual improvement of the standards of practice, development of local PN protocols and practice guidelines to support pharmacists and to serve the local needs in different countries, standardization of PN-related practices and services, and empowerment of pharmacists to assume a stronger leadership role in this dimension of pharmacy practice are among the potential avenues of improvement in this area of clinical pharmacy practice.
Conclusion
Pharmacists have been actively participating in providing PN-related services to patients in different countries. Most of the evidence evaluating pharmacists’ role in PN support has been documented primarily from developed countries, but it is also being investigated in some developing countries. Pharmacists’ provision of clinical services for the management of PN support patients has been associated with adequate nutrition care and medical therapy; improved nutritional status and clinical outcomes of patients; prevention and resolution of PN-associated complications and reduced PN support-related health care costs. More involvement of pharmacists in the provision of direct care services to these patients will result in improved patient outcomes and enhanced quality of PN services. To fulfill the requirements of that role, pharmacists need adequate educational preparation and clinical training on nutrition support. The empowerment of pharmacists to assume a stronger leadership role in this dimension of pharmacy practice will enhance the quality of care provided to patients receiving PN therapy and improve PN services.
Disclosure
The author reports no conflicts of interest in this work.
References
- MirtalloJCanadaTJohnsonDTask Force for the Revision of Safe Practices for Parenteral NutritionSafe practices for parenteral nutritionJPEN J Parenter Enteral Nutr2004286S39S7015568296
- DriscollDFHospital pharmacists and total parenteral nutrition: current status and trendsEur J Hosp Pharm Sci Pract200814164
- RagabMHAl-HindiMYAlrayeesMMNeonatal parenteral nutrition: review of the pharmacist role as a prescriberSaudi Pharm J201624442944027330373
- WorthingtonPBalintJBechtoldMWhen is parenteral nutrition appropriate?JPEN J Parenter Enteral Nutr201741332437728333597
- KochevarMGuenterPHolcombeBMaloneAMirtalloJASPEN Board of Directors and Task Force on Parenteral Nutrition StandardizationASPEN statement on parenteral nutrition standardizationJPEN J Parenter Enteral Nutr200731544144817712154
- ColombVCommercially premixed 3-chamber bags for pediatric parenteral nutrition are available for hospitalized childrenJ Nutr201314312 suppl2071S2076S24108138
- KatoueMGAl-TaweelDMatarKMKombianSBParenteral nutrition in hospital pharmaciesInt J Health Care Qual Assur201629666467427298063
- BarnettMICosslettAGDuffieldJREvansDAHallSBWilliamsDRParenteral nutrition. Pharmaceutical problems of compatibility and stabilityDrug Saf19905suppl 11011062108706
- DriscollDFStability and compatibility assessment techniques for total parenteral nutrition admixtures: setting the bar according to pharmacopeial standardsCurr Opin Clin Nutr Metab Care20058329730315809533
- LumpkinMMSafety alert: hazards of precipitation associated with parenteral nutritionAm J Hosp Pharm19945111142714287942876
- American Society of Health-System PharmacistsASHP technical assistance bulletin on quality assurance for pharmacy-prepared sterile productsAm J Hosp Pharm19935011238623988266973
- AyersPAdamsSBoullataJAmerican Society for Parenteral and Enteral NutritionA.S.P.E.N. parenteral nutrition safety consensus recommendationsJPEN J Parenter Enteral Nutr201438329633324280129
- MeadowsNMonitoring and complications of parenteral nutritionNutrition199814108068089785367
- DoddsESMurrayJDTrexlerKMGrantJPMetabolic occurrences in total parenteral nutrition patients managed by a nutrition support teamNutr Clin Pract2001167884
- WalmsleyRSRefeeding syndrome: screening, incidence, and treatment during parenteral nutritionJ Gastroenterol Hepatol201328suppl 411311724251716
- HeplerCDThe future of pharmacy: pharmaceutical careAm Pharm1990NS30102329
- HeplerCDStrandLMOpportunities and responsibilities in pharmaceutical careAm J Hosp Pharm19904735335432316538
- BerenguerBLa CasaCde la MattaMJMartin-CaleroMJPharmaceutical care: past, present and futureCurr Pharm Des200410313931394615579081
- American Society of Hospital PharmacistsASHP statement on pharmaceutical careAm J Hosp Pharm19935017201723
- HowardPPractical nutritional support: working together to make it happenProc Nutr Soc200160341541811681818
- TuckerAYbarraJBinghamAAmerican Society for Parenteral and Enteral NutritionAmerican society for parenteral and enteral nutrition (ASPEN) standards of practice for nutrition support pharmacistsNutr Clin Pract201530113914625288252
- DeLeggeMHKellyATState of nutrition support teamsNutr Clin Pract201328669169724170578
- Anoz JimenezLBorras AlmenarCCavera RodrigoEPharmaceutical procedures in patients under treatment with total parenteral nutritionFarm Hosp200428534935515504092
- Sevilla SanchezDPlaceres AlsinaMMMiana MenaMTLopez SuneECodina JaneCRibas SalaJPharmaceutical intervention with parenteral nutritionFarm Hosp201034191520144816
- DudrickSJWilmoreDWVarsHMRhoadsJELong-term total parenteral nutrition with growth, development, and positive nitrogen balanceSurgery19686411341424968812
- MirtalloJMAdvancement of nutrition support in clinical pharmacyAnn Pharmacother200741586987217456538
- FlackHLGansJASerlickSEDudrickSJThe current status of parenteral hyperalimentationAm J Hosp Pharm19712853263354999686
- NehmeAENutritional support of the hospitalized patient. The team conceptJAMA198024319190619086767864
- American Society of Health-System PharmacistsASHP guidelines on the safe use of automated compounding devices for the preparation of parenteral nutrition admixturesAm J Health Syst Pharm200057141343134810918925
- American Society for Parenteral and Enteral NutritionStandards for nutrition support pharmacistsNutr Clin Pract1993831241278289760
- TeitelbaumDGuenterPHowellWHKochevarMERothJSeidnerDLDefinition of terms, style, and conventions used in A.S.P.E.N. guidelines and standardsNutr Clin Pract200520228128516207664
- HolcombeBJThornDBStrausburgKMAnalysis of the practice of nutrition support pharmacy specialistsPharmacotherapy19951568068138602394
- DoughertyDBankheadRKushnerRMirtalloJWinklerMNutrition care given new importance in JCAHO standardsNutr Clin Pract199510126317898414
- National Advisory Group on Standards and Practice Guidelines for Parenteral NutritionSafe practices for parenteral nutrition formulationsJPEN J Parenter Enteral Nutr199822249669527961
- RollinsCDurfeeSMHolcombeBJStandards of practice for nutrition support pharmacistsNutr Clin Pract200823218919418390788
- GreenlawCWPharmacist as team leader for total parenteral nutrition therapyAm J Hosp Pharm1979365648650110145
- FaberEMProgram for training staff pharmacists in total parenteral nutritionAm J Hosp Pharm19914859809861906679
- McDermottLAAlbrechtJTGoodDHNutritional support: pharmacists’ influence on the prescribing processTop Hosp Pharm Manage1994143303910138926
- BroylesJEBrownROVeheKLNollyRJLutherRWPharmacist interventions improve fluid balance in fluid-restricted patients requiring parenteral nutritionDICP19912521191221905438
- MaclarenRDevlinJWMartinSJDastaJFRudisMIBondCACritical care pharmacy services in United States hospitalsAnn Pharmacother200640461261816569803
- PedersenCASchneiderPJScheckelhoffDJASHP national survey of pharmacy practice in hospital settings: prescribing and transcribing--2010Am J Health Syst Pharm201168866968821460173
- SeresDSacksGSPedersenCAParenteral nutrition safe practices: results of the 2003 American Society for Parenteral and Enteral Nutrition surveyJPEN J Parenter Enteral Nutr200630325926516639075
- BoullataJIGuenterPMirtalloJMA parenteral nutrition use survey with gap analysisJPEN J Parenter Enteral Nutr201337221222223112276
- YangSLeeBSParkHWEffect of high vs standard early parenteral amino acid supplementation on the growth outcomes in very low birth weight infantsJPEN J Parenter Enteral Nutr201337332733422891034
- MirtalloJMHawksworthKPayneBA nutrition support service web application to manage patients receiving parenteral nutritionNutr Clin Pract200924444745819605799
- GiancarelliADavanosEEvaluation of nutrition support pharmacist interventionsJPEN J Parenter Enteral Nutr201539447648125303948
- GalesBJRileyDGImproved total parenteral nutrition therapy management by a nutritional support teamHosp Pharm199429546947047347510134172
- MousaviMHayatshahiASarayaniAImpact of clinical pharmacist-based parenteral nutrition service for bone marrow transplantation patients: a randomized clinical trialSupport Care Cancer201321123441344823949839
- MirtalloJMSacksGSA “call to action” for an expanded pharmacist role in influencing the quality of nutrition careJPEN J Parenter Enteral Nutr201337444644723670602
- CerulliJMaloneMAssessment of drug-related problems in clinical nutrition patientsJPEN J Parenter Enteral Nutr199923421822110421391
- RollinsCJPharmacist interventions: unique perspective versus taking the lead in nutrition support when knowledge and skills overlap with other healthcare disciplinesJPEN J Parenter Enteral Nutr201539438138225303947
- MullerRJHoffmanDMMulliganRMParenteral nutrition program in a major cancer centerHosp Pharm1981162546610309346
- MaisonneuveNRagusoCAPaoloni-GiacobinoAParenteral nutrition practices in hospital pharmacies in Switzerland, France, and BelgiumNutrition200420652853515165615
- BataniRAAbdullahDCBahariMBEvaluation of the total parenteral nutrition service at Universiti Sains Malaysia HospitalE Spen Eur E J Clin Nutr Metab200726e111e115
- KatoueMGAl-TaweelDRole of the pharmacist in parenteral nutrition therapy: challenges and opportunities to implement pharmaceutical care in KuwaitPharm Pract (Granada)201614268027382419
- MutchieKDSmithKAMacKayMWMarshCJulusonDPharmacist monitoring of parenteral nutrition: clinical and cost effectivenessAm J Hosp Pharm1979366785787111548
- DiceJEBurckartGJWooJTHelmsRAStandardized versus pharmacist-monitored individualized parenteral nutrition in low-birth-weight infantsAm J Hosp Pharm19813810148714896794364
- GaffronREFlemingCRBerknerSMcCallumDSchwartauNMcGillDBOrganization and operation of a home parenteral nutrition program with emphasis on the pharmacist’s roleMayo Clin Proc198055294986766522
- LeesCDSteigerEHooleyRAHome parenteral nutritionSurg Clin North Am19816136216336789476
- DurfeeSMAdamsSCArthurEA.S.P.E.N. Standards for nutrition support: home and alternate site careNutr Clin Pract201429454255524964788
- American Society of Health-System PharmacistsASHP guidelines on the pharmacist’s role in home careAm J Health Syst Pharm200057131252125710902068
- KarnackCMGallinaJNJeffreyLPPharmacist involvement in home parenteral nutrition programsAm J Hosp Pharm19813822152176782872
- TomitaIIshiiSYonezawaMItoTHiraiAMizunoKRole of national insurance pharmacies in community complete home care networks--home TPN and home care supported by local national insurance pharmaciesGan To Kagaku Ryoho200027suppl 3S683S686
- PietkaMWatrobska-SwietlikowskaDSzczepanekKSzybinskiPSznitowskaMKlekSNutritional support teams: the cooperation among physicians and pharmacists helps improve cost-effectiveness of home parenteral nutrition (HPN)Nutr Hosp201431125125925561117
- Hernandez de la Figuera y GomezTJimenez TorresNVRonchera OmsCLOrdovas BainesJPThe participation of pharmacy services in evaluating parenteral nutrition programsNutr Hosp1989431491532485365
- HarbottleLBracheEClarkeJAudit of parenteral nutrition use in GuernseyInt J Pharm Pract200917529329820214271
- BoitanoMBojakSMcCloskeySMcCaulDSMcDonoughMImproving the safety and effectiveness of parenteral nutrition: results of a quality improvement collaborationNutr Clin Pract201025666367121139133
- McDermottLAAlbrechtJTGoodDHStanfordGGDocumentation of clinical interventions in nutritional supportTop Hosp Pharm Manage1993132324510128813
- MartinCMThe consultant pharmacist’s expanded role in nutrition managementConsult Pharm200924641442119555152
- StrausburgKMNutrition support pharmacist board certification processHosp Pharm199530319219619920020710140763
- Board of Pharmacy Specilities [webpage on the Internet]Nutrition Support Pharmacy Available from: https://www.bpsweb.org/bps-specialties/nutrition-support-pharmacy/#1517761118361-6c02bae3-f5a015177800157771517854077689Accessed April 27, 2018
- EbiasahRPSchneiderPJPedersenCAMirtalloJMEvaluation of board certification in nutrition support pharmacyJPEN J Parenter Enteral Nutr200226423924712090689
- DurfeeSMPharmacist specialty certificationJPEN J Parenter Enteral Nutr2012362 suppl51S52S22275326
- The National Board of Nutrition Support Certification (NBNSC) [webpage on the Internet]National Board of Nutrition Support Certification:multiple disciplines; a single standard of excellence Available from: http://www.nutritioncare.org/NBNSC/Certification/Certification_Main_Page/Accessed April 25, 2018
- The European Society of Clinical Nutrition and Metabolism [webpage on the Internet]The Life Long Learning (LLL) Programme in Clinical Nutrition and Metabolism Available from: http://www.espen.org/education/lll-programmeAccessed December 15, 2017
- American Society for Parenteral and Enteral Nutrition (ASPEN) [web-page on the Internet]Continuing Education With ASPEN Available from: https://www.nutritioncare.org/continuing-education/Accessed March 20, 2018