

Abstract
Introduction
Respiratory infections have significant effects on childhood asthma. Viral respiratory infections, such as rhinovirus and respiratory syncytial virus are likely to be important in the development and exacerbation of asthma. In this study, we investigated the nasopharyngeal colonization in children with asthma to determine the prevalence of pathogens and their contribution to respiratory symptoms and airway resistance during winter.
Methods
From December 2016 to March 2017, 50 nasopharyngeal specimens were collected from 18 patients (age, 5.0±1.1 years) with asthma and 9 specimens from 9 control children (age, 4.9±1.0 years). Samples were tested for 19 viruses and 7 bacteria, using multiplex real-time PCR. Respiratory disease markers included the Global Asthma Network Questionnaire, the Common-Cold Questionnaire, the Global Initiative for Asthma assessment of asthma control, and the airway resistance at 5 Hz by forced-oscillation technique.
Results
The most commonly isolated organisms in both groups (patients and controls) were Streptococcus pneumoniae, Haemophilus influenzae, and rhinovirus. Most patients had multiple isolates (median, 3.5; range, 1–5), which changed during the study period. Types of isolates were 4 bacteria (S. pneumoniae, H. influenzae, Bordetella pertussis, and Bordetella parapertussis) and 6 viruses (rhinovirus, enterovirus, metapneumovirus, adenovirus, coronaviruses, and parainfluenza viruses). Similar isolates, including influenza A-H3 virus and bocavirus, were detected in the controls. Of the 9 patients with “wheezing disturbing sleep ≥1 per week”, 6 had rhinovirus, 2 coronaviruses, and 1 no detectable viruses. Patients with mild common cold symptoms had significantly higher airway resistance at 5 Hz z-score (P=0.025).
Conclusion
Multiple respiratory pathogens were isolated from many patients with asthma, which appeared to contribute to disease symptoms and airway resistance. Minimizing children’s exposure to respiratory pathogens might be beneficial, especially during winter.
Supplementary materials
Figure S1 Percent positive nasopharyngeal pathogens isolated from the 18 patients with asthma (A) and the 9 healthy children (B) during the studied winter periods.
Note: “x”, not detected.
Abbreviations: AdV, adenovirus; BP, Bordetella pertussis; BPP, Bordetella parapertussis; CoV coronavirus; Flu A-H3, influenza A virus-H3; hBoV, human bocavirus; hEV, human enterovirus; HI, Haemophilus influenzae; hRV, human rhinovirus; PIV1, parainfluenza virus 1; PIV3, parainfluenza virus 3; SP, Streptococcus pneumoniae.
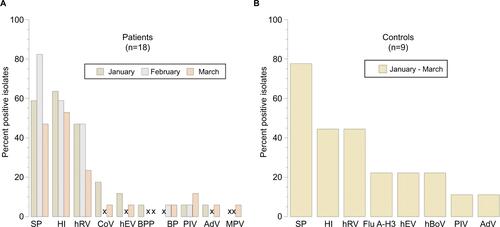
Table S1 Nasopharyngeal isolates, airway resistance (R5), “common cold” symptoms (CCQ), and GINA score in the 18 patients with asthma
Table S2 Nasopharyngeal isolates, airway resistance (R5), “common cold” symptoms (CCQ), and GINA in the 18 patients with asthma
Table S3 Responses to the Global Asthma Network Questionnaire (based on symptoms in the past 12 months) in the 18 patients with asthma
Acknowledgments
The authors are grateful to all participating children and their parents. The contribution of Mrs Sania M Al-Hamad toward data collection is greatly appreciated. The study was funded by a grant from the College of Medicine and Health Sciences, UAE University (31M252). The funding body had no role in the design of the study, collection, analysis, and interpretation of data, or in writing the manuscript.
Author contributions
ARA conceived the study, participated in its design and coordination, and drafted the manuscript. AMA, AA, and GA recruited participants and collected clinical data. JG and SMK coordinated and performed PCR experiments. HN and AKS participated in the data analysis and manuscript preparation. All authors contributed toward data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.