

Abstract
Purpose
Patients with severe asthma are eligible for asthma-specific biologics as add-on therapies, such as mepolizumab and omalizumab, when optimized controller therapies are unable to control their symptoms. However, few real-world data are available to describe the characteristics and associated economic burden of patients considered to be candidates for mepolizumab or omalizumab therapy.
Methods
This retrospective cohort study investigated patients with asthma (≥12 years of age) identified at the time of first mepolizumab or omalizumab administration (index date) in the MarketScan™ Commercial Database. Data were collected during the 12-month period before the index date (baseline period) for two mutually exclusive patient groups (patients prescribed mepolizumab and omalizumab, respectively). Baseline demographics, history of exacerbations, healthcare resource utilization (HCRU), and medical costs were investigated.
Results
In total, 413 and 1,834 patients who had been prescribed mepolizumab or omalizumab, respectively, were identified. During the baseline period, patients prescribed mepolizumab experienced more exacerbations (81.4% vs 57.5%, P<0.001), had higher asthma-related HCRU for outpatient services (all P<0.01), and had higher total asthma-related healthcare costs (US$11,000 vs US$7,400, P<0.001) compared with patients prescribed omalizumab. Allergic rhinitis, atopic dermatitis, and chronic idiopathic urticaria were more common among patients prescribed omalizumab vs mepolizumab. In contrast, sinusitis, nasal polyps, and comorbid COPD were more common among patients prescribed mepolizumab vs omalizumab. Prescriptions of fixed-dose inhaled corticosteroids (ICSs) with long-acting β2-agonists (LABAs) and ICS/LABA/long-acting muscarinic antagonist triple therapy during the baseline period were higher among patients prescribed mepolizumab vs omalizumab (80.4% vs 56.8% and 27.1% vs 14.4%, respectively, both P<0.001).
Conclusion
In the 12 months prior to initiation of asthma-specific biologics, patients prescribed mepolizumab had a different prevalence of certain comorbidities, higher disease burden, higher HCRU, and higher healthcare costs compared with patients prescribed omalizumab.
Data availability
GSK makes available anonymized individual participant data and associated documents from interventional clinical studies which evaluate medicines, upon approval of proposals submitted to www.clinicalstudydatarequest.com. To access data for other types of GSK sponsored research, for study documents without patient-level data, and for clinical studies not listed, please submit an enquiry via the website.
Supplementary materials
Methods
MarketScan™ commercial claims and encounters database
This database contains information about privately insured individuals with fee-for-service, fully capitated, and partially capitated health plans. The plans include preferred provider organizations, point-of-service plans, indemnity plans, and health maintenance organizations.
Assignment of patients to treatment group
Assignment to treatment groups was hierarchical to ensure that each patient would be included in one treatment group. The patients administered mepolizumab during the patient identification period were selected first regardless of omalizumab use in that same time period; the remaining omalizumab patients, with no evidence of mepolizumab use during the patient identification period, were assigned to the omalizumab treatment group. After this initial assignment, patients prescribed mepolizumab with evidence of omalizumab use in the patient identification period were excluded.
Exclusion criteria
Patients were excluded if they did not have a diagnosis of asthma in the 12 months prior to, or on, the index date (ICD-9 493.xx or ICD-10 J45.xx), or if they used omalizumab during the 12 months prior to the index date. Patients were also excluded if they had a chronic idiopathic urticaria diagnosis in the absence of an asthma diagnosis in the 12 months prior to initiating omalizumab.
Asthma-related costs
Asthma-related costs were a subset of all-cause costs calculated from claims with an asthma diagnosis in any position on outpatient/emergency room claims and in the primary position on inpatient claims. Costs were calculated from paid amounts of adjudicated claims, including insurer and health plan payments, as well as patient cost-sharing in the form of co-payment, deductible, and co-insurance.
Results
Immunosuppressive therapy use in the 12-month baseline period
Overall, the number of patients receiving immunosuppressive therapies (tumor necrosis factor inhibitors, interleukin inhibitors, abatacept, alemtuzumab, belimumab, canakinumab/pf, glatiramer acetate, interferon-β-1a, interferon-β-1a/albumin human, interferon-β-1b, peginterferon-β-1a, rituximab, tofacitinib citrate, vedolizumab, natalizumab, and ocrelizumab) during the 12-month baseline period was similar (only 1.0%–1.2%).
Figure S1 Proportion of patients with all-cause HCRU during the 12-month baseline period (main analysis excluding patients with prior biologic use).
Notes: aIncludes other outpatient services, such as radiology services, laboratory tests, and outpatient infusion.
Abbreviations: ER, emergency department; HCRU, healthcare resource utilization.
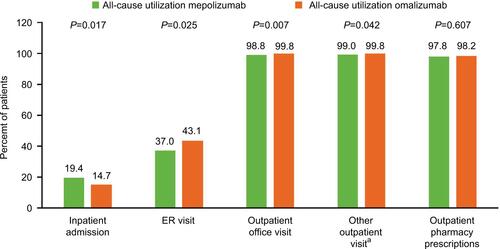
Figure S2 Proportion of patients with exacerbations during the 12-month baseline period (sensitivity analysis including patients who had received omalizumab or mepolizumab during the baseline period).
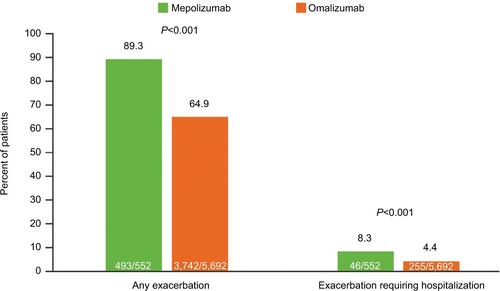
Figure S3 Proportion of patients with an asthma-related HCRU during the 12-month baseline period (sensitivity analysis including patients who had received omalizumab or mepolizumab during the baseline period).
Abbreviation: ER, emergency room; HCRU, healthcare resource utilization.
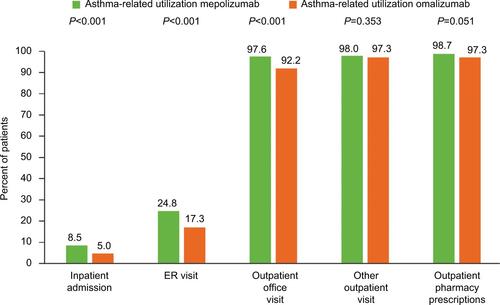
Figure S4 Asthma-related (A) and total (B) healthcare expenditure during the 12-month baseline period (sensitivity analysis including patients who had received omalizumab or mepolizumab during the baseline period).
Abbreviation: ER, emergency room.
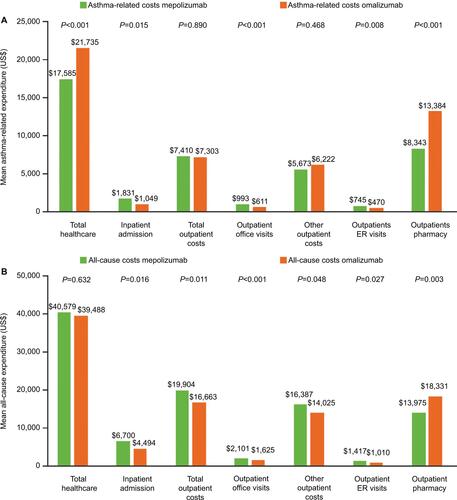
Table S1 All-cause HCRU during the 12-month baseline period (main analysis excluding patients with prior biologic use)
Table S2 Demographic characteristics at index date (sensitivity analysis including patients who had received omalizumab or mepolizumab during the baseline period)
Table S3 Clinical characteristics of patients during the 12 months prior to treatment (sensitivity analysis including patients who had had received omalizumab or mepolizumab during the baseline period)
Table S4 Asthma-related HCRU during the 12-month baseline period (sensitivity analysis including patients who had received omalizumab or mepolizumab during the baseline period)
Acknowledgments
We would like to thank Christina Larson-Chebili for her assistance during the data acquisition phase of the study and SAS programming. Editorial support (in the form of writing assistance, including development of the initial draft based on author direction, assembling tables and figures, collating and incorporating authors’ comments, grammatical editing, and referencing) was provided by Mary E Morgan, PhD, of Fishawack Indicia Ltd, UK, and was funded by GSK. This study was funded by GSK (study identifier: HO-16–16497).
Author contributions
All authors contributed to the conception and the design of the study. EP, ET, and DEI were involved in data acquisition; BH, CFB, J-PL, and HO analyzed and interpreted the data. All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
J-PL, CFB, and BH are GSK employees and hold stock/shares. HO was an employee of GSK and holds stocks/shares in GSK during the conduct of this study and is now employed by Gossamer Bio. EP, ET, and DEI are Truven Health Analytics, An IBM Watson Health Company employees. The authors report no other conflicts of interest in this work.