
Abstract
The basophil activation test (BAT) is an ex vivo functional assay that measures by flow cytometry the degree of basophil degranulation after stimulation with an allergen. In recent years, there has been an increased interest in the diagnostic value of the BAT as it has the potential to mimic the clinical phenotype of sIgE sensitized patients, in contrast to allergen-specific IgE levels. This diagnostic potential would be of particular interest for food allergies present early in life such as peanut, cow’s milk and eggs, which require an expensive, time-consuming and patient unfriendly oral food challenge (OFC) for diagnosis. However, routine applications of the BAT for clinical use are not yet feasible due to the lack of standardized protocols and large clinical validation studies. This review will summarize the current data regarding the application of the BAT in food allergy (FA) for cow’s milk, egg and peanut, being the most common causes of FA in children. Additionally, it will discuss the hurdles for widespread clinical use of the BAT and possible future directions for this diagnostic procedure.
Introduction
Most food allergies (FA) are diagnosed in early life, nevertheless the diagnosis can be made in older children or even adults. Currently there are fourteen foods listed as recognized food allergens in the European Union,Citation1 of which eight are responsible for approximately 95% of FA cases: cow’s milk, eggs, fish, peanuts, shellfish, soy, tree nuts and wheat.Citation2 In the US, approximately 9% of adults have a FA diagnosis;Citation3 meanwhile, in Europe it stands at about 6% among adults.Citation4 In children below the age of five the prevalence of FA ranges between 4% and 10% worldwide.Citation5,Citation6
An oral food challenge (OFC) is the current gold-standard for FA diagnosis; however this method is labor intensive, costly and implies the risk of a severe and life threatening anaphylaxis. Determination of the prevalence of food allergies is dependent on confirmation by this gold standard; however, since OFCs are not only time-consuming but carry an inherent risk they might not be acceptable to all study participants.Citation7
FA varies in etiology, allergen type and severity which contributes to a challenging diagnosis. Adding complexity to this diagnosis there is also the cross-reactivity between allergens, the concomitant presence of multiple food allergens and food intolerances.Citation8 The symptoms of a FA and a food intolerance can overlap, therefore a proper differential diagnosis is crucial since a FA triggers an immune response which can end in a life-threatening event known as anaphylaxis. The current cornerstone of FA diagnosis is the clinical history aided in most cases by specific IgE levels in blood (sIgE) and/or skin prick test (SPT). Both tests have a high sensitivity but low specificity; both detect sIgE sensitization which is not the same as a food allergy; in other words sensitization does not necessarily lead to the development of symptoms. Additionally, both assays currently lack reliable threshold values as they are dependent on factors like the type of allergen/food and study population (eg, age, other diseases). The next step for food allergy diagnosis is an OFC; particularly the double-blind placebo-controlled food challenge (DBPCFC). Because of the drawbacks of these diagnostic challenges, FA diagnosis is trending towards the development of screening tests reducing the indications for OFCs. This approach, however, requires the establishment of thresholds values for SPT and sIgE that can predict the likelihood of a clinical reaction.Citation9 The burden of a FA misdiagnosis manifests in increased anxiety and diminished quality of life for patients plus potential nutritional deficiencies due to dietary restrictions.Citation10 Furthermore, the economic cost of FA misdiagnosis to society are not insignificant with many resources being dedicated to further medical evaluation, additional testing and unnecessary prescriptions.Citation11
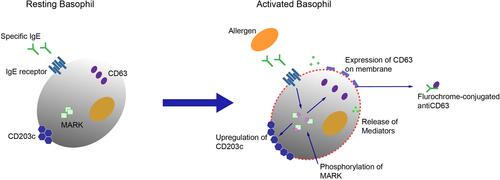
Under this scenario, the interest in the basophil activation test (BAT) has increased as a potential tool which simulates an allergic reaction ex vivo. The BAT is a flow cytometric assay that detects the functional ability of IgE to activate basophils which are stimulated due to allergen exposure (see ). However, there is still knowledge lacking regarding degranulation metrics and implementation guidelines to guarantee universality in the execution of the test and interpretation of the results.Citation12,Citation13 The BAT measures the expression of activation markers (mainly CD63 or CD203c) on the basophil cell membrane following cross-linking of IgE antibodies caused by an allergen.Citation14,Citation15 Even though basophils are scarce (they form less than 3% of peripheral white blood cells) they are easily accessible cells and their activation is quantifiable. Therefore, the BAT is a promising biomarker for the diagnosis of a food allergy and can replace the OFC.
Figure 1 Basophil activation test principle. At a resting mode, the activation marker CD203c is expressed at low levels, but upon activation it is rapidly up-regulated. In addition, when the basophil is in a resting mode the activation marker CD63 is mainly present inside the cell granules. Upon activation, after exposure to an allergen, the granules fuse with the cell membrane and CD63 is exposed on the cell surface and can be detected by labelled antibodies with subsequent flow cytometry. Therefore the expression of CD63 is closely associated with degranulation.
The BAT has been validated for different IgE-mediated food allergies and showed a high sensitivity and specificity.Citation16,Citation17 The accuracy of the BAT has been shown to be higher than tests for IgE sensitization (sIgE/SPT)Citation12,Citation17 and the BAT has been able to differentiate clinically allergic patients from those who were sensitized but tolerant, with a specificity ranging from 75% to 100% and a sensitivity between 77% to 98%.Citation12,Citation15–Citation17 This specificity and sensitivity profile has positioned the BAT as a potential tool in reducing the number of OFCsCitation12 contributing to the interest in further developing this technique for FA diagnosis.
One reason for this improved diagnostic power can be attributed to the fact that the BAT is a functional assay, therefore the results are not dependent on the amount of IgE alone but also on its characteristics such as affinity, avidity and even on antibodies of other isotypes (eg, IgG4).Citation18
Kits for performing the BAT have become more readily available for any clinical or research laboratory with a flow cytometry facility.Citation19 Nonetheless, standardization and harmonization of the BAT technique plus interpretation of results are still lacking and not yet defined. Many questions remain regarding how feasible it is to standardize the BAT and its methodology while adopting a protocol that allows for comparison of results between different centers. Simultaneously, universal threshold values should be established and data for specific allergens validated in different allergic populations whilst evaluating the cost-effectiveness of this technique. It is important to keep in mind when validating the BAT in the context of cross-reactivity syndromes that the performance of the test will be influenced by the control group, a healthy control group will likely overestimate the specificity of the test and therefore also the diagnostic accuracy of the reference test.Citation13
The BAT and Food Allergy Diagnosis
Food allergies that begin at an early age such as cow’s milk, egg and peanut, present a higher diagnostic challenge as performing an OFC in children generates significant anxiety in parents and clinical staff. Furthermore an OFC in young children can be difficult to perform (eg, willingness of the patient to eat) and interpret since the majority of the symptoms are subjective and the test is often not continued until objective symptoms are reached.Citation20,Citation21 Both milk and egg allergies start early in life and the majority becomes naturally tolerant over time whereas peanut allergy starts later in life and is usually lifelong. Therefore, in this subgroup of FA, the BAT as a tool would represent a significant diagnostic improvement in FA diagnosis in the clinical practice as it has the potential to reduce the need for an OFC.Citation22 Furthermore, most of the clinical validation data currently available for the BAT are obtained with egg, milk and peanut; therefore, these data are used to deduce and sum up the current clinical application of the BAT. Although most articles regarding the BAT focus on diagnosis there is pertinent data available regarding the role of the BAT in monitoring the effect of immunotherapy as well.Citation23
The BAT mimics the clinical phenotype of patients while other allergy tests can only detect the presence of allergen-specific IgE. Additionally, the BAT can differentiate sensitization from a true food allergy and thus segregate between allergy and tolerance, particularly in children with peanut or egg allergy.Citation24
Peanut Allergy
Peanut allergy (PA) is one of the most common food allergies worldwide accounting for 0.5% to 1.5% of the population in Western countries.Citation25 PA usually starts around 18 months of age but can begin later in life, either as stand-alone allergy or as part of the pollen-food allergy syndrome.Citation26 PA, along with tree nut allergies, is the most common cause for life threatening anaphylactic reactions. Even though only a small percentage of US children are clinically allergic to peanut (currently 1.4%), approximately 10% are sensitized to it; consequently, the proper diagnosis in this group is vital for the quality of life of the patients and their families.Citation27 In FA diagnosis, it is becoming critical to be able to identify the individual disease phenotype to provide the correct individualized treatment; thus, techniques that can separate cross-reactivity with other allergen families and pollen allergen are gaining importance.Citation28 For example; Arachis hypogea 2 (Ara h 2) specific IgE (reflecting sensitization) has been shown to be a useful predictor of clinical reactivity.Citation29 In children with suspected PA, the BAT diagnosed PA with 98% specificity and 75% sensitivity. Moreover, the BAT was the best biomarker for severity, identifying severe reactions with 97% specificity and 100% sensitivity.Citation30 Thus, the BAT outperformed the level Ara h 2 specific-IgE, level of peanut specific-IgE and IgG4/IgE ratio, only to be surpassed by the SPT.Citation30 Therefore, the BAT is capable of predicting the allergic clinical status to peanut in children and could reduce the need for OFCs.Citation12,Citation30
It has been observed that a higher proportion of activated basophils is associated with more severe reactions and a lower threshold of activation, raising the question if severity is linked to threshold. For example; in adults that suffer from severe peanut allergy similar associations have been identified using the BAT, where basophil reactivity to peanut was significantly higher in patients who had a history of severe allergy to peanuts when compared to patients who were sensitized to peanuts (p<0.001).Citation31 However, further validation is necessary before applying this result more broadly including to other food allergens and to other patient populations.Citation28
Moreover, single peanut or tree-nut allergic patients are often sensitized to other tree-nuts requiring multiple OFC for diagnosis since the main challenge with these patients is distinguishing between sensitization and allergy. The BAT has shown to be capable to discriminate between allergic and nonallergic children, to the respective nut/seed when tested against peanut, hazelnut, cashew nut, sesame, and almond.Citation32 Moreover, this study reported that the use of the BAT as a second step in the diagnostic process reduced the number of OFC by 5% to 15% after equivocal SPT and IgE to extracts and components. This notion was later reinforced by further studies showing that separately the SPT and the BAT were limited in their capacity to distinguish allergy from tolerance; however, when used in conjunction as part of the diagnostic kit their ability to identify allergic and tolerant patients improved.Citation33 Moreover, the same study also concluded that this approach could potentially reduce the need for OFCs with 78.2% in walnut/pecan cases and with 76.6% in cashew/pistachio cases.Citation33 Additionally, the BAT has been useful to differentiate between the allergenicity of different allergen extracts in hazelnut allergic patients. In 132 hazelnut allergic patients, sensitization was confirmed by SPT and sIgE against hazelnut;Citation34 following a hazelnut free diet, a DBPCFC was performed with increasing amounts of native and roasted hazelnut. The BAT was measured before and after provocation and it showed that significantly higher concentrations of the allergen extract were needed (roasted>native) to induce 50% basophil activation. Therefore, the researchers concluded that the BAT was useful in determining the reactivity of an allergen extract.Citation34
In PA patients, oral immunotherapy (OIT) can significantly shift the threshold dose of peanut that can be ingested without generating symptoms. Sustained protection during and after OIT has been reported in association with lower levels of basophil activation at 13 weeks after active OIT.Citation35 Hence, patients with a low basophil responsiveness after OIT were more likely to achieve treatment success.Citation36 Using the Ara h 2 as a predictor of clinical reactivity, the BAT could provide a functional surrogate of efficacy since studies have demonstrated that basophil sensitivity to Ara h 2 is a useful biomarker for long time efficacy of peanut OIT.Citation37 Therefore there is increasing data that the BAT provides additional value in monitoring the response to immunotherapy.Citation38
Cow’s Milk Allergy
Cow’s milk allergy (CMA) is the most common childhood allergy with a prevalence of approximately 2.5% worldwide.Citation20 The onset of this allergy is generally related to the introduction of cow’s milk based infant formula and currently it affects 1 in every 50 infants under the age of one with most of the patients outgrowing their allergy during childhood or pre-puberty.Citation39 CMA is highly variable with allergens involved in the allergic response. Previously, ß-lactoglobulin, the most abundant whey protein, was thought to be the most important allergen in CMA since it is not present in human milk and up to 76% of the patients react to this protein.Citation40 Nowadays, it is known that other proteins, including α-lactalbumin and caseins, are critically involved in the disease. Low levels of ß-lactoglobulin and casein allergen-specific (known as Bos d 8) sIgE concentrations have been described as predictive for the resolution of CMA.Citation41
The lack of specific clinical manifestations can often lead to a misdiagnosis; the current diagnostic tests include sIgE (sensitivity 87%, specificity 48%) and SPT (sensitivity 88%, specificity 68%) while the current gold standard for CMA diagnosis is the double-blind placebo-control food challenge (DBPCFC).Citation41,Citation42 The difficult diagnostic scenario has resulted in an over-diagnosis of CMA, possibly undermining breast feeding rates and leading to unnecessary elimination diets with negative nutritional impact.Citation43 For example, a meta-analysis showed that the self-reported prevalence of CMA was approximately 6%, however the prevalence fell to 0.6% when CMA was confirmed by DBPCFC.Citation41 The BAT has been described as highly efficient in confirming CMA in childrenCitation44 with a sensitivity of 89% and a specificity of 83% for cow’s milk extract,Citation45 positive predictive value of 81% and negative predictive value of 96% in detecting persistently allergic patients.Citation46 For safety and commercial reasons, milk is processed by using various treatments (heat and other physio-chemical) that can alter the allergenic potency of milk proteins. The BAT can help to distinguish between patients that can tolerate heated forms of cow’s milk from those who are not able to. Therefore, the BAT can provide important information which has implications for the prognosis of CMA patients as patients who persistently do not tolerate heated milk will have a higher chance to develop a more persistent form of CMA allergy.Citation47,Citation48
Even though most patients diagnosed with CMA will outgrow this allergy in the first years of life, the prognosis for those who do not is worse; with cow milk IgE levels reported being highly predictive for this outcome.Citation20
Therefore, in FA that are commonly outgrown with time such as CMA, the BAT can be useful in assessing the natural resolution of food allergies and in deciding when to reintroduce cow’s milk to the patient’s diet. The BAT has been described as highly effective in improving the diagnostic accuracy in CMA since it can mimic the acute degree of CMA against cow’s milk and human milk allergens as well as assist in monitoring the development of CMA;Citation49 offering the possibility that the BAT could be a reliable and cost effective diagnostic tool when clinicians suspect an IgE mediated CMA which could in turn diminish the need for DBPCFCs.Citation50
In recent years, many studies have demonstrated the efficacy of OIT for CMA ranging from 67% tolerance at 18 weeksCitation51 to 90% showing complete desensitization after 1 year.Citation52 Nevertheless, follow-up studies have found that full milk tolerance decreases dramatically over time, which suggests that protection is more difficult to maintain than previously described.Citation53 Current recommendations suggest treatment of CMA should wait until the child is 3 years old; however, recent findings suggest that OIT is a promising strategy for CMA even in young children. OIT has demonstrated to achieve full tolerance in a high percentage of children with mild side effects that can be easily managed by slowing the desensitization.Citation54 At the end of oral food allergy desensitization, a significant decrease in specific IgE levels and increase in specific IgG4 levels is described in the literature, highly possible due to a switch from a Th2 to a Th1 response;Citation55 therefore by analyzing the up-regulation of allergen-induced CD63 with flow cytometry it is possible to monitor the progression of clinical tolerance by OIT in FA. There is little information regarding the use of the BAT for monitoring the clinical tolerance induced by OIT in CMA; however, a reduction of cow’s milk protein-induced CD63 expression levels at the end of the desensitization protocol has been observed and the BAT has been described as highly sensitive and closely correlated with clinical tolerance.Citation56
Egg Allergy
Egg allergies are common IgE mediated food allergies in children with a prevalence ranging from 1.3% to 10.1%,Citation20 with most cases presenting during the first year of life. The prognosis is generally good with the majority of children outgrowing their allergy at school age. A proper diagnosis of egg allergy is crucial for several reasons, which can also be valid for other food allergies, (1) it can cause severe allergic reactions in sensitized children, (2) unnecessary avoidance due to a misdiagnosis leads to significant dietary restrictions and the possibility of nutritional deficiencies, (3) early sensitization to egg is a known marker of later sensitization to aeroallergens and the possible future development of asthma and (4) many vaccines that are administered during childhood contain egg therefore an egg allergy diagnosis is crucial to determine which vaccines are safe to administer.Citation57
Most of the allergenic proteins are found in the egg white: ovomucoid (Gal d 1), ovalbumin (Gal d 2), ovotransferrin (Gal d 3), egg white lysozyme (Gal d 4) and ovomucin; with Gal d 2 ovalbumin being the most abundant protein in egg white.Citation58 Currently the BAT for egg allergy is described with a sensitivity of 63% and a specificity of 96% for CD203c expression and a sensitivity of 77% and a specificity of 100% for CD63 expression using ovalbumin.Citation17 An important diagnostic conundrum for clinicians is the distinction between allergic and sensitized children (clinically tolerant but demonstrate a positive sIgE and/or SPT). Studies have attempted to evaluate if the BAT can play a role in addressing this diagnostic problem, which when presented requires further evaluation with an OFC. At the moment, the data suggests that most egg-sensitized but tolerant children are unable to elicit basophil activation upon allergen challenge.Citation59 Therefore, the BAT might be a handy tool to complement conventional tests in this group of patients allowing for a better differentiation between allergic and non-allergic patients.Citation45
Generally, individuals with egg allergy can tolerate cooked products that contain egg which would imply that the allergic response is dependent on epitope configuration. The ovalbumin proteins are heat labile while the ovomucoid epitopes do not seem to be affected by heating. Some heat labile allergenic proteins change their configuration during the cooking process and therefore their immunogenic potential is either blunted or minimized.Citation60 Alternatively, partially unfolded proteins could expose existing hidden epitopes and increase their allergenic activity. So, net effects are hard to predict without pre-existing knowledge or careful analysis of epitopes present in the allergens and severe allergic reactions can occur with a single bite of cooked egg (about 70mg of egg protein). Patients that are diagnosed with an egg allergy are placed on egg-free diets, but total egg avoidance is very challenging both for patients and caregivers. Therefore, new treatment strategies are being explored. Food oral immunotherapy can induce tolerance or desensitize patients that are allergic to egg and it is associated with a median success rate of over 80%.Citation61 The aim of the OIT in the treatment for a FA, as previously indicated, is to achieve tolerance to the usual or certain doses of the allergenic food to prevent reactions in case of ingestion of small quantities of said food. This is mainly attributed to several immunological responses, mainly a decrease in specific IgE, increase in specific IgG4 antibodies, formation of specific regulatory T cells and changes in the basophil response.Citation62
Research has shown that in OIT in egg allergic children produces a reduction in basophil activation after allergen stimulation; a significant decrease in percentage of CD203c+ cells (p = 0.04) and a lower percentage of CD63+ cells (p = 0.07) over time after stimulation with 0.01 µg/mL anti-ovomucoid.Citation63 This could be caused by changes in circulating levels and surface bound IgE on the basophils and in the amount of IgE receptors on the basophil surface. Therefore, using the BAT to test the safety and efficacy of a new immunotherapy such as low allergenic hydrolyzed egg is a handy tool for researchers and clinicians to circumvent expensive OFCs.
Future Directions of the Basophil Activation Test
The BAT is currently not widely used in FA diagnosis, although it possess a high diagnostic potential, it lacks validation and standardization to allow results comparisons between different laboratories and protocols that can be universally applied need to be formulated. This process should include not only the proper reference test that would be used to validate and standardize the BAT, but also the considerations of the possible drawbacks of utilizing such a reference and additionally a protocol for the allergens used and their importance in each subgroup of patients, as well as which activation markers are better suited for a specific patient population. These are among the main factors that need to be clearly established before the BAT can be universally used for clinical diagnosis or research (see ).
Table 1 Technical Considerations for Widespread Use of the BAT
BAT Validation and Standardization, the Reference Test
Standardization and validation of a new diagnostic test starts with the choice of the reference test(s). Currently, OFCs outcomes are used as the gold standard for FA diagnosis. A DBPCFC would be the best test as it removes patient and observer bias;Citation64 therefore, it should be the reference test for validation and standardization of a newer diagnostic tool such as the BAT. However, even this gold standard has limitations as 3% false-positive, 3% false-negative results and 10% dubious outcomes occur.Citation65–Citation67 In addition, there are several other points of concern like differences in dosing scheme and type of food matrices. Uniformity concerning these issues has not been obtained yet. Furthermore, reproducibility of the OFC has not been extensively tested. However, Glaumann et al found that that the threshold of the OFC showed a much higher variation and lower reproducibility than the sensitivity of the BAT (CD-sens).Citation68 Finally, although there are guidelines for the stop criteria of an OFC (ie, PractallCitation69) the question remains whether subjective symptoms are similar to objective symptoms in predicting the degree of severity and avoidance of food allergen traces. Thus, even though the OFC is the best diagnostic tool currently available, uncertainties remain about its value in clinical practice. Therefore, when validating the BAT by using the OFC, the limitations of the reference test need to be considered. This also urges us to rethink the applications of the OFC and new diagnostic tools, with their own drawbacks, in the optimization of food allergic diagnostics. Nevertheless, like the gold standard, a new diagnostic tool should be extensively validated in robustness and applicability. For the BAT it means that much research is still required concerning the source and type of allergens used, the optimal readout-parameters and the determination of reliable and safe cut-off values.
Allergen Selection
The BAT is a functional assay that evaluates the activation state of basophil cells before and after stimulation with allergens. The structure and availability of IgE-binding epitopes of the allergens in the food is influenced by food matrix composition as well as food processing steps before exposure to the patient. For food diagnostic purposes, raw allergen preparations are often used while individuals are mostly exposed to processed foods, eg in the case of soy or peanut proteins. Therefore, the use of raw extracts can compromise the diagnostic procedure and interpretation of the efficacy of tolerance induction; the BAT gives the possibility to test various allergen preparations which gives it a diagnostic advantage over other techniques, like the OFC.
The expected response in an allergic patient in a BAT test is a bell shape dose-response curve. Nonetheless the complexity of antigens and the affinity of different profiles of epitope-specific IgE can vary the shape of the dose-response curve.Citation70 Several factors have an impact on the basophil surface activation markers dose-response curve, amongst them: affinity of the antigen for the cell-bound IgE antibodies, density of the epitope-specific IgE antibodies and epitope spreading of the IgE antibody.Citation70 All of these factors determine the optimal allergen concentration for basophil activation and might vary significantly among subjects. To account for this issue it is advised to include a broad range of allergen concentrations to better evaluate the effect of the allergen in the basophil response.
Currently food allergy diagnostic tools mainly include water-soluble allergens and thus lipophilic allergens are missing. Using purified mixtures of Ara h 10/11 and Ara h 14/15 (ie peanut lipophilic oleosins) the BAT showed that the rate of peanut oleosin sensitization among peanut allergic patients was 65%.Citation71 This shows that sensitization to peanut oleosins is clinically relevant and therefore oleosins are major allergens in peanut allergy. Nevertheless, in order to evaluate the predictive value of these results they need to be compared with the outcome of the OFC and other peanut allergens with additional multicenter studies.Citation72
Peanut allergenic proteins are significantly affected by thermal processing which is caused by the interaction between the proteins and other food compounds such as sugars. An example of such interaction is the Maillard reaction, which involves the formation of neo-allergens by promoting the aggregation and formation of new epitopes. These neo-allergens may increase the severity of the allergic reaction in some individuals who are sensitized against processed and not raw allergens; therefore providing a need to include processed food in the diagnosis of FA, which normally use raw extract for PA diagnosis. Moreover, it is known that thermal processing affects the degranulation capacity differently, increasing in Ara h 1 while decreasing in Ara h 2/6;Citation73 granting the BAT an important role in the assessment of food processing on protein allergenicity. As shown by Vissers et al, it is important to include degranulation assays in addition to the commonly studied IgE reactivity to have an inside in the clinical relevance of an allergen.Citation73 The authors showed that the IgE-binding capacity of Ara h 1 roasted in the presence of sugar was decreased 9000-fold compared with native Ara h 1, while the capacity to elicit mediator release was increased. In this area, the BAT has been described as helpful to determine the effect of thermal processing on the allergenicity of peanut proteins. A study which used both IgE immunoblotting and the BAT for raw and roasted peanuts did not find a correlation between the two techniques, highlighting the fact that IgE binding studies do not predict the potential of an allergen to trigger cell degranulation. The authors explained the discrepancy between a positive immunoblotting result and a negative BAT as an occurrence due to sensitization to heat-resistant cross-reactive carbohydrate determinants, which is a main cause of positive IgE results that have no clinical significance.Citation74 Consequently, the BAT provides important additional information to the results yielding from the IgE binding techniques.
In addition to providing valuable information regarding the allergenicity of peanuts and hazelnut, the BAT has yielded meaningful information about the non-specific lipid transfer proteins that are involved in allergies to fresh and processed fruits. The BAT showed that only severe heat treatment of Mal d 3 from apple peel caused significant decrease in its allergenicity, suggesting that the sugar in fruit may contribute to the thermostability of the allergenic activity.Citation75 Hence, the BAT is a suitable diagnostic tool to assess the allergenicity of processed allergens. Nonetheless, which processed allergens should be used in the BAT to reflect the in vivo situation still needs much research.
Determination of the Degree of Basophil Activation
Activation Markers
Following allergen stimulation, human basophils exhibit different degranulation patterns releasing various mediators and expressing particular activation markers. The BAT detects phenotype changes of allergen induced basophil degranulation; for this different protocols are in place using CCR3, CD123, CRTH2, CD203c or anti-IgE to identify basophils. All these markers are expressed on the basophil membrane but secondary makers are necessary to exclude CRTH2 + T cells or CD123+ plasmacytoid dendritic cells. Additionally, it has been suggested that CD203c is the marker that reveals the purest basophil cell population when compared to other markers (CCR3+, CRTH2+/CD3−, CCR3+/CD3−, IgE+, among others) and that anti-IgE should be used when a basophil population of very high purity is needed.Citation76 For a valid interpretation of the results, the precise identification of the population of basophils is crucial.Citation15 As long as these markers are not compared in one population it is difficult to determine which markers perform best; hence studies that compare different identification and activation markers in the same population are needed.
Moreover, degranulation is detected by surface expression of CD63, which is only expressed on the inner side of the granule membrane of the resting basophil.Citation77 Since the development of the BAT, several activation markers have been studied and compared. In the mid 1990’s the CD63 activation marker was discovered and currently is the most favored activation marker because it is directly related to histamine release and it is easily accessible since it is expressed in a distinct positive population.Citation48,Citation76,Citation78 The other valuable marker is CD203c;Citation79 however, it does not form a distinct positive population and is a more general basophil marker which can be used both as an identification and as an activation marker.Citation48 CD63 and CD203c are upregulated after IgE receptor aggregation but follow partially different metabolic pathways.
Presently, there is no standardization of CD63 or CD203c detection and the determination of the positive threshold value.Citation24 Furthermore, at several allergen concentrations, some studies have shown, that CD63 and CD203c expression differed between allergic or sensitized patients.Citation76 For example, in hazelnut allergy CD203c expression showed a better discrimination capacity when compared to CD63 and therefore was more accurately able to distinguish between sensitized and allergic patients.Citation79 This could be explained by the differences in kinetics between CD63 and CD203c. While the maximal up-regulation for CD63 is between 25–30 minutes, for CD203c it is at 10–20 minutes; in this study the stimulation time used averaged 15 minutes to capture both markers.Citation79 In general, expression of CD203c reach their peak quickly and starts to decline after approximately 20 minutes and both CD63 and CD203c disappear after 4 to 5 hours of incubation.
A possible new marker is CD300, a surface receptor on basophils. This receptor was shown to increase during IgE mediated basophil degranulation but it is not necessarily elevated as a result of an allergen-mediated degranulation. The CD300 marker is correlated to enhanced degradation and its expression levels correlated with the severity of symptoms particularly in children with a severe CMA symptomatology; thereby suggesting that CD300c has a role in the clinical manifestation of CMA by decreasing the activation threshold of basophils.Citation80 An additional marker of interest is CD300a, an inhibitory receptor that is rapidly up-regulated in response to IgE/FcεRI (high affinity receptor for IgE) and inhibits anaphylactic basophil degranulation.Citation81 Furthermore, the expression of CD300a, similar to CD63, remained in a plateau for approximately 2 hours. CD300a is associated with inhibitory ITIM-mediated signaling (immunoreceptor tyrosine-based inhibitory motifs) which may hamper activation processes.Citation81 Moreover with an inhibitory net observed effect, several studies have reported a CD300a dominance over CD300c;Citation80,Citation82 thus more precise tools are needed to characterize the functional input from CD300a and CD300c.
The current data suggest that depending on the allergen and the cohort used, there might be a variability in the sensitivity and specificity of the basophil activation markers. On the other hand, as several markers can be measured, the BAT is a valuable tool for researchers as it can assess various immunological pathways providing valuable insights into immune mechanisms of allergic diseases.Citation22
Result Analysis and Interpretation
Since the analysis and interpretation of the results of the BAT can be intensive and laborious, recently a data driven programmatic approach has been proposed to analyze the flow cytometric results in a more reproducible, unbiased and productive way. By using the R Bioconductor package, flowCore, researchers were able to analyze 269 basophil activation tests from a clinical trial in a quick and efficient way, representing a net saving of 1340 minutes of labor by a skilled operator and only 2% of the basophil activation results differ significantly from manual gating.Citation83 This data-driven approach could provide a platform for the BAT data to be analyzed in a more transparent and reproducible way with better quality control and additionally providing an adequate way for data sharing among clinicians and researchers.
Commonly there are two ways to measure basophil activity; by the number of basophil that respond to a stimulus (basophil reactivity) or by the allergen concentration at which half of all reactive basophils respond (basophil sensitivity); once reactivity is confirmed it may be useful to evaluate sensitivity.Citation48 Basophil reactivity can be expressed as %CD63+ basophils at a given allergen concentration and it refers to the proportion of basophils that express CD63 compared to the negative control.Citation84 Basophil reactivity can also be expressed as the ratio of %CD63+ to allergen IgE-mediated positive control (anti-IgE or anti- FcεRI) and recently two studies reported an association between basophil reactivity and symptom severity in PA patients.Citation30,Citation84 To measure sensitivity the reactivity at 6–8 allergen concentrations is measured, then the graded response is fitted to a curve of reactivity vs allergen concentration and the eliciting concentration at which 50% of basophils (EC50) is determined.Citation70 From this parameter, CD-sens can also be determined as 1/EC50 x 100. Basophil sensitivity has been reported to be helpful in the diagnosis of food allergy.Citation12,Citation70 Both basophil reactivity and sensitivity seem to be distinct parameters of activation; nonetheless both are regulated by Syk and appear to be interdependent.Citation70
Recently, the area under the dose-response curve (AUC) is gaining interest since it is a marker of sensitivity and reactivityCitation48,Citation70 and it can be calculated in cases where responses do not fit well to a typical dose-response curve.Citation48 Furthermore, it uses several measuring points, at multiple allergen concentrations, which lowers the risk of false outcomes.
Therefore basophil reactivity and basophil sensitivity plus read-out parameter such as CD-sens, EC50 and AUC have been reported as sensitive biomarkers that reflect the clinical severity of anaphylactic reactions, the clinical thresholds for eliciting symptoms and OIT particularly in FA patients.Citation85 A result of increased basophil reactivity and sensitivity reported in thresholds of BAT parameters, can help a clinician decide whether or not to perform an oral provocation test.Citation85
Automation of the Basophil Activation Test
Presently, the BAT is regarded as a good ex vivo test that holds many diagnostic advantages in FA which include high sensitivity/specificity, low risk profile, potential to predict symptom severity and importantly the potential to discriminate between sensitized asymptomatic and truly allergic patients;Citation17,Citation86 nevertheless, as mentioned before, there are still some hurdles to fully embrace the capabilities of this test broadly in the clinical practice.
It is not only the lack of standardization that is currently a challenge, there are also issues concerning some of the procedural limitations such as the needed flow cytometry expertise, cost, technical operational and maintenance aspects, the challenging pre-processing and pre-labelling of samples and the ponderous of existing workflows. Difficulties like this mean that currently the BAT remains limited to specialized laboratories.
The BAT is performed in a limited number of laboratories as blood sampling and storage for this type of test requires special conditions to preserve cell viability and functionality (eg, sample needs to remain refrigerated) and should be used within 8 hours after obtaining the sample, although some researchers currently suggest it can be as long as 24 hours,Citation87,Citation88 since at room temperature IgE mediated reactions decrease faster.Citation59 Currently, there are several time limits mentioned in the literature so there is no real consensus and this poses a problem because presently the inclination is to obtain the sample and perform the test so quickly that it is a challenge.Citation15
In order to reduce hands-on time, efforts have been made to develop a simplified and standardized whole-blood based BAT prototype procedure to increase the automation of this test. Arif-Lusson et al proposed a whole blood based and simplified procedure for the BAT which relies on a dry antibody formulation technology that can be transposed in a 96 well plate format.Citation89 Moreover, a novel microfluidic-based immunoaffinity BAT (miBAT) has been introduced to simplify the cumbersome BAT processes and therefore makes it more accessible to clinical practice. This microfluidic device is coated with anti-CD203c and designed to capture basophils from whole blood directly which are then activated by anti-FcεRI antibody and followed by optical detection of CD63 expression.Citation90 Blood collected from allergic patients and healthy controls was analyzed with the miBAT with the expression of CD63 percentage significantly higher after allergen activation when compared to the negative control (p < 0.001) and miBAT data were comparable to flow cytometry.Citation91 This technique however still needs validation in larger patient populations to assess its performance.
In addition to the storage time of the sample, there is a lack of consensus regarding which of the existing BAT protocols should be applied to harmonize results and therefore be able to compare them between laboratories. Behrends et al recently published a simplified protocol with automation of sample preparation, measurement and data analysis plus lengthening of the time between blood collection and sample processing.Citation86 The researchers created a novel gating strategy with 3 antibodies (FcεRIα, CD203c, CD63) which was compared to their previous protocol that used 12 antibodies; the results found no differences in sensitivity and specificity between the two protocols or between the automated and the manually analysed samples, which saved 90% of labor time. Moreover, this new protocol by Behrends considerably extended the time frame for performing a BAT after blood donation to 7 days for whole blood storage at room temperature and 17 days at 4°C prior to BAT preparation and measurement. The researchers confirmed their results via a nationwide ring trial that showed a robust and applicable BAT protocol in a variety of flow cytometers.Citation86 Agyemang et al took a different approach to preserve basophil activation stability and therefore expand the use of the BAT.Citation92 Agyemang et al evaluated a novel peanut-BAT (P-BAT) as a diagnostic method of peanut allergy; in this pilot study basophils in whole blood were stimulated with six peanut concentrations (0.0001–10 mg/mL) within 3 to 4 hours of sample acquisition and activation was measured by CD63+ and CD203c+ expression via flow cytometry on days 0, 1, 3 and 5. Findings showed basophil activation at each peanut concentration with the P-BAT method on day 0, and it was sustained on days 1, 3 and 5 without further stimulation; therefore by using the P-BAT method researchers eliminated the immediate need for sample processing by a simple activating basophils in a simple way using whole blood, which can be easily performed in the first 4 hours of sample collection.Citation92
Passive BAT
Directly exposing basophils from fresh whole blood or isolated peripheral blood mononuclear cells to various allergen concentrations is a technique known as “direct BAT”.Citation14 This technique has certain limitations; for example, the recommendation that the test has to be performed within 8 to 24 hours after collection of the blood sample as basophil reactivity decreases over timeCitation88 and a key problem known as “anergy”, which means non-responding basophils to IgE receptor-mediated signaling after stimulation with one or more types of allergen or anti- FcεRI IgE receptor stimulation, a problem that presents in about 10% of the individuals.Citation15 This “basophil anergy” appears to be associated with a down-regulation of basophil Syk expression and function plus an apparent reduction in the incidence of allergic rhinitis.Citation93
Research has shown that it is possible to reproduce passive sensitization of basophils with IgE ex vivo, this technology can be applied to allergic diseases as well. In the “passive” (also called “indirect”) BAT (iBAT) isolated basophils from pooled healthy donor blood are stripped from receptor bound IgE and passively sensitized with sIgE from an allergic patient’s serum. Subsequently, these basophils can be activated by exposing them to the allergens of interest. This allows the storage of large amounts of patient serum and to determine the allergic status at once at a later point in time, solving one of the crucial performance issues with the BAT.Citation14 Moreover, by using pooled blood from several donors the risk for “basophil anergy” is reduced. This technique demands more time and is more labor intensive when compared to the direct BAT, but the advantages it presents for researchers and clinicians for exploring immunological allergy mechanisms as well as optimizing allergy diagnosis and monitoring treatment efficacy should not be overlooked.Citation14 A different approach to combat the issue of non-responding basophils was taken by Santos et al, by researching if the ability to elicit peanut-induced cell activation could be transferred by passive sensitization of LAD2 mast cells with patients plasma.Citation84 The mast cell activation test (MAT) to peanut strongly correlated with the BAT (RS = 0.808, P < 0.001) plus the MAT gave a conclusive results for participants with non-responding basophils; however, the BAT showed a greater diagnostic accuracy due to its higher sensitivity.Citation94
Additionally it is important to note that by using a passive BAT the influence of the patient basophils are not taken into account which might be an important factor. However, a study regarding peanut allergy and the use of the iBAT predicted a peanut allergy which is comparable to studies that used the direct BAT.Citation17 Nevertheless, it is unknown whether intrinsic basophil characteristics can play a minor role in some patients.
Conclusions
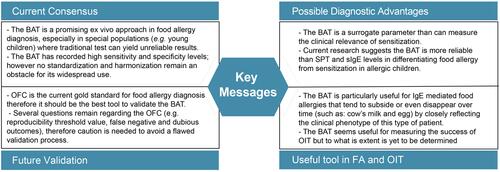
The current challenge in FA diagnosis is to develop a technique which is both accessible and reliable plus could replace the expensive, time-consuming and patient-unfriendly OFCs. The key messages from this review are summarized in . Currently, the BAT is a promising ex vivo diagnostic tool in food allergy diagnosis. Nonetheless, several methodological aspects need to be investigated before a standardized protocol is available which can be universally applied making comparisons between results of different studies justified, which are summarized in . Besides the fact that the diagnostic accuracy of the reference test, an OFC, is crucial the type of allergen used in the BAT is a main point to consider as the BAT does not reflect food processing and digestion. In addition, it is also highly necessary to standardize the basophil identification and activation markers plus procedures for detection of activation basophils. In our opinion, the way of conquering these challenges might be possible by collaboration between clinicians and laboratory technicians in multi-center studies. Furthermore, the role and applicability of current diagnostic tools, such as OFC, should be discussed in order to be able to determine the diagnostic power and place of the BAT in the current diagnostic work-up for a food allergy.
Figure 2 Summary of the key messages of the current status of applying BAT in allergy diagnostics and immunotherapy.
Disclosure
The authors report no conflicts of interest in this work.
References
- National Academies of Sciences, Engineering and Medicine; Health and Medicine Division; Food and Nutrition Board. Finding a Path to Safety in Food Allergy: Assessment of Food of the Global Burden, Causes, Prevention and Management, and Public Policy. US: National Academies Press; November 30, 2016.
- European Commission Directive. 2007/68/EC of 27TH November; 2007.
- Gupta RS, Warren CM, Smith BM, et al. Prevalence and severity of food allergies among US adults. JAMA Netw Open. 2019;2(1):e185630. doi:10.1001/jamanetworkopen.2018.5630
- Nwaru BI, Hicktein L, Panesar SS, Roberts G. Prevalence of common food allergies in Europe: a systematic review. Allergy. 2014;69:992–1007. doi:10.1111/all.12423
- Mori F, Barni S, Saretta F, et al. Epidemiology of rare allergic diseases in children. Pediatr Allergy Immunol. 2020;31(26):39–42. doi:10.1111/pai.13359
- Loh W, Tang MLK. The epidemiology of food allergy in the global context. Int J Environ Res Public Health. 2018;15:2043. doi:10.3390/ijerph15092043
- Kelleher MM, Jay N, Perkin MR, et al. An algorithm for diagnosing IgE-mediated food allergy in study participants who do not undergo food challenge. Clin Exp Allergy. 2020;50(3):330–342. doi:10.1111/cea.13577
- Foong RX, Santos AF. Biomarkers of diagnosis and resolution of food allergy. Pediatr Allergy Immunol. 2021;32:223–233.
- De Martinis M, Sirufo MM, Suppa M, Ginaldi L. New perspective in food allergy. Int J Mol Sci. 2020;21:1474. doi:10.3390/ijms21041474
- King RM, Knibb RC, Hourihane JO. Impact of peanut allergy on quality of life, stress and anxiety in the family. Allergy. 2009;64(3):461–468. doi:10.1111/j.1398-9995.2008.01843.x
- Bird JA, Crain M, Varshney P. Food allergen panel testing often results in misdiagnosis of food allergy. J Pediatr. 2015;166(1):97–100. doi:10.1016/j.jpeds.2014.07.062
- Santos AF, Douiri A, Becares N, et al. Basophil activation test discriminates between allergy and tolerance in peanut-sensitized children. J Allergy Clin Immunol. 2014;134(3):645–652. doi:10.1016/j.jaci.2014.04.039
- Ebo DG, Bridts CH, Mertens CH, Sabato V. Principles, potential, and limitations of ex vivo basophil activation by flow cytometry in allergology: a narrative review. J Allergy Clin Immunol. 2021;147(4):1143–1153. doi:10.1016/j.jaci.2020.10.027
- Hemmings O, Kwok M, McKendry R, Santos AF. Basophil activation test: old and new applications in allergy. Curr Allergy Asthma Rep. 2018;18(12):77. doi:10.1007/s11882-018-0831-5
- Anostegui IJ, Melioli G, Canonica GW, et al. IgE allergy diagnostics and other relevant test in allergy, a World Allergy Organization position paper. World Allergy Organ J. 2020;13:100080. doi:10.1016/j.waojou.2019.100080
- Patil SU, Bunyavanich S, Phil M, Berin MC. Emerging food allergy biomarkers. J Allergy Clin Immunol Pract. 2020;8(8):2516–2524. doi:10.1016/j.jaip.2020.04.054
- Santos AF, Shreffler WG. Road map for the clinical application of the basophil activation test in food allergy. Clin Exp Allergy. 2017;47:1115–1124. doi:10.1111/cea.12964
- Santos AF, James LK, Bahnson HT, et al. IgG4 inhibits peanut-induced basophil and mast cell activation in peanut-tolerant children sensitized to peanut major allergens. J Allergy Clin Immunol. 2015;135(5):1249–1256. doi:10.1016/j.jaci.2015.01.012
- Cottel N, Saf S, Bourgoin M, et al. Two different composite markers predict severity and threshold dose in peanut allergy. J Allergy Clin Immunol Pract. 2020;9(1):275–282. doi:10.1016/j.jaip.2020.09.043
- Savage J, Sicherer S, Wood R. The natural history of food allergy. J Allergy Clin Immunol Pract. 2016;4:196–203. doi:10.1016/j.jaip.2015.11.024
- Niggemann B. Pitfalls in double-blind, placebo-control oral food challenges. Allergy. 2007;62:729–732. doi:10.1111/j.1398-9995.2007.01396.x
- Santos A, Gideon L. Basophil activation test: food challenge in a test tube or specialist research tool? Clin Transl Allergy. 2016;6(1):1–9. doi:10.1186/s13601-016-0098-7
- Paranjape A, Tsai M, Mukai K, et al. Oral immunotherapy and basophil mast cell reactivity in food allergy. Front Immunol. 2020;11:602660. doi:10.3389/fimmu.2020.602660
- McGowan EC. Update on the performance and application of basophil activation test. Curr Allergy Asthma Rep. 2013;13(1):101–109. doi:10.1007/s11882-012-0324-x
- Ezendam J, van Loveren H. Parameters needed to estimate the global burden of peanut allergy. RIVM Report 340007002; 2012.
- Vereda A, van Hage M, Ashlstedt S, et al. Peanut allergy: clinical and immunological differences among patients from 3 different geographical regions. J Allergy Clin Immunol. 2011;127:603–607. doi:10.1016/j.jaci.2010.09.010
- Warren C, Lei C, Sicherer S, Scheimer R, Gupta R. Prevalence and characteristics of peanut allergy is US adults. J Allergy Clin Immunol. 2021;147(6):2263–2270.
- Duan L, Celik A, Hoang JA, et al. Basophil activation test shows high accuracy in the diagnosis of peanut and tree nut allergy: the markers of nut allergy. Allergy. 2021;76(6):1800–1812.
- Ehlers AM, den Hartog Jager CF, Knulst AC, Otten HG. Distinction between peanut allergy and tolerance by characterization of B cell receptor repertoires. Allergy. 2021;76(9):2753–2764. doi:10.1111/all.14897
- Santos AF, Du Toit G, O’Rourke CO, et al. Biomarkers of severity and threshold of allergic reactions during oral peanut challenges. J Allergy Clin Immunol. 2020;146(2):344–355. doi:10.1016/j.jaci.2020.03.035
- Rentzos G, Lundberg V, Lundqvist C, et al. Use of basophil activation test as a complementary diagnostic tool in the diagnosis of severe peanut allergy in adults. Clin Transl Allergy. 2015;5:22. doi:10.1186/s13601-015-0064-9
- Santos AF, Bergmann M, Caubet JC, et al. Basophil activation test reduces oral food challenges to nut and sesame. J Allergy Clin Immunol Pract. 2021;9(5):2016–2027. doi:10.1016/j.jaip.2020.12.039
- Elizur A, Appel MY, Nachshon L, et al. NUT Co Reactivity – ACquiring Knowledge for Elimination Recommendations (NUT CRACKER) study. Allergy. 2018;73:593–601. doi:10.1111/all.13353
- Worm M, Hompes S, Fiedler EM, Ilner AK, Zuberbier T, Vieths S. Impact of naïve, heat-processed and encapsulated hazelnuts on the allergic response. Clin Exp Allergy. 2009;39(1):159–166. doi:10.1111/j.1365-2222.2008.03143.x
- Tsai M, Mukai K, Chinthrajah RS, Nadeau KC, Galli SJ. Sustained successful peanut oral immunotherapy associated with low basophil activation and peanut-specific IgE. J Allergy Clin Immunol. 2020;145:885–896. doi:10.1016/j.jaci.2019.10.038
- Burks AW, Wood RA, Jones SM, et al. Sublingual immunotherapy for peanut allergy: long term follow up of a randomized multicentre trial. J Allergy Clin Immunol. 2015;135(5):1240–1248. doi:10.1016/j.jaci.2014.12.1917
- Patil SU, Ogunniyi AO, Calatroni A, et al. Peanut oral immunotherapy transiently expands circulating Ara h 2-specific B cells with homologous repertoire in unrelated individuals. J Allergy Clin Immunol. 2015;136(1):125–134. doi:10.1016/j.jaci.2015.03.026
- Patil SU, Steinbrecher J, Calatroni A, et al. Early decrease in basophil sensitivity to Ara h 2 precedes sustained unresponsiveness after peanut oral immunotherapy. J Allergy Clin Immunol. 2019;144(5):1310–1319. doi:10.1016/j.jaci.2019.07.028
- Schoemaker AA, Sprikkelman AB, Grimshaw KE, et al. Incidence and natural history of challenge-proven cow’s milk allergy in European children – EuroPrevall birth cohort. Allergy. 2015;70(8):963–972. doi:10.1111/all.12630
- Crittenden RG. Cow’s milk allergy: a complex disorder. J Am Coll Nutr. 2005;24 (6):582S–59S. doi:10.1080/07315724.2005.10719507
- Fiocchi A, Brozek J, Schunemann H, et al. World Allergy Organization Diagnosis and Rationale for Action against Cow’s Milk Allergy (DRACMA) guidelines. Pediatr Allergy Immunol. 2010;21(21):1–125.
- Zeng Y, Zhang J, Dong G, et al. Assessment of cow’s milk-related symptom scores in early identification of cow’s milk protein in Chinese infants. BMC Pediatr. 2019;19(1):1–7. doi:10.1186/s12887-019-1563-y
- Munblit D, Perkin MR, Palmer DJ, et al. Assessment of evidence about common infant symptoms and cow’s milk allergy. JAMA Pediatr. 2020;174(6):599–608. doi:10.1001/jamapediatrics.2020.0153
- Ciepiela O, Zwiazek J, Zawadzka-Krajewska A, Kotula M, Kulus U. Basophil activation test based on the expression of Cd203c in the diagnostic of cow milk allergy in children. Eur J Med Res. 2010;15(ii):21–26. doi:10.1186/2047-783X-15-S2-21
- Sato S, Tachimoto H, Shukuya A, et al. Basophil activation marker CD203c is useful in the diagnosis of hen’s egg and cow’s milk allergies in children. Int Arch Allergy Immunol. 2010;152(1):54–61. doi:10.1159/000312126
- Rubio A, Vivinus-Nebot M, Bourrier T, Saggio B, Albertini M, Bernard A. Benefit of the basophil activation test in deciding when to reintroduce cow’s milk in allergic children. Allergy. 2010;66(1):92–100. doi:10.1111/j.1398-9995.2010.02432.x
- Norgaard A, Bernard H, Wal JM, et al. Allergenicity of individual cow milk protein in DBPCFC-positive milk allergic adults. J Allergy Clin Immunol. 1996;97(3):237. doi:10.1016/S0091-6749(96)80436-2
- Hoffman HJ, Santos AF, Mayorga C, et al. The clinical utility of basophil activation test in diagnosis and monitoring of allergic disease. Allergy. 2015;70:1393–1405. doi:10.1111/all.12698
- Schocker F, Kull S, Schwager C, Behrends J, Jappe U. Individual sensitization pattern recognition to cow’s milk and human milk differs for various clinical manifestations of milk allergy. Nutrients. 2019;11:1331. doi:10.3390/nu11061331
- Ruinemans-Koerts J, Schmidt-Hieltjes Y, Jansen A, Savelkoul HFJ, Plasier A, van Setten P. The basophil activation test reduced the need for a food challenge test in children suspected of IgE mediated cow’s milk allergy. Clin Exp Allergy. 2018;49(3):350–356. doi:10.1111/cea.13307
- Panjo GB, Caminiti L, Ruggeri P, et al. Oral immunotherapy for cow’s milk allergy with a weekly up-dosing regimen: a randomized single-blind controlled study. Ann Allergy Asthma Immunol. 2010;24(4):376–381.
- Martorell A, De la Hoz B, Ibanez MD, et al. Oral desensitization as a useful treatment in 2 year old children with cow’s milk allergy. Clin Exp Allergy. 2011;41(9):1297–1304. doi:10.1111/j.1365-2222.2011.03749.x
- Burbank AJ, Sood P, Vickery BP, Wood RA. Oral immunotherapy for food allergy. Immunol Allergy Clin North Am. 2016;36:55–69. doi:10.1016/j.iac.2015.08.007
- Passalacqua G, Landi M, Pajno GB. Oral immunotherapy for cow’s milk allergy. Curr Opin Allergy Clin Immunol. 2012;12:271–277. doi:10.1097/ACI.0b013e3283535b93
- Nucera E, Schiavino D, D’Ambrosio C, et al. Immunological aspects of oral desensitization in food allergy. Dig Dis Sci. 2000;45:637–641. doi:10.1023/A:1005430231735
- Nucera E, Pecora V, Buonomo A, et al. Utility of basophil activation test for monitoring the acquisition of clinical tolerance after oral desensitization to cow’s milk: Pilot Study. United European Gastroenterol J. 2015;3(3):272–276. doi:10.1177/2050640615570694
- Savage JH, Matsui EC, Skirpak JM, Wood RA. The natural history of egg allergy. J Allergy Clin Immunol. 2007;120(6):1413–1417. doi:10.1016/j.jaci.2007.09.040
- Mather P, Pfleghaar JL. Egg Allergy. Stat Pearls Publications; 2020.
- Ocmant A, Mulier S, Hanssens L, et al. Basophil activation test for the diagnosis of food allergy in children. Clin Exp Allergy. 2009;39(8):1234–1245. doi:10.1111/j.1365-2222.2009.03292.x
- Berin MC, Grishin A, Masilamani M, et al. Egg-specific IgE and basophil activation but not egg-specific T-cell counts correlate with phenotypes of clinical egg allergy. J Allergy Clin Immunol. 2018;142(1):149–158. doi:10.1016/j.jaci.2018.01.044
- Ibáñez MD, Escudero C, Sánchez-García S, Rodriguez Del Rio P. Comprehensive review of current knowledge on egg immunotherapy. J Investig Allergol Clin Immunol. 2015;25:316–328.
- Gamboa PM, Garcia-Lirio E, Gonzalez C, Gonzales A, Martinez-Aranguren RM, Sanz Maria L. Is the quantification of antigen-specific basophil activation a useful tool for monitoring oral tolerance induction in children with egg allergy? J Investig Allergol Clin Immunol. 2016;26(1):25–30. doi:10.18176/jiaci.0004
- Giavi S, Vissers YM, Muraro A, et al. Oral immunotherapy with low allergenic hydrolysed egg in egg allergic children. Allergy. 2016;71:1575–1584. doi:10.1111/all.12905
- Grabenhenrich LB, Reich A, McBride D, et al. Physician’s appraisal vs documented signs and symptoms in the interpretation of food challenge test: the EuroPrevall birth cohort. Pediatr Allergy Immunol. 2018;29(1):58–65. doi:10.1111/pai.12811
- Grabenhenrich LB, Reich A, Bellach J, et al. A new framework for the documentation and interpretation of oral food challenges in population-based and clinical research. Allergy. 2017;72(3):453–461. doi:10.1111/all.13049
- Van Erp FC, Knulst AC, Meijer Y, Gabriele C, van der Ent CK. Standardized food challenges are subject to variability in interpretation of clinical symptoms. Clin Transl Allergy. 2014;4:43. doi:10.1186/s13601-014-0043-6
- Brand PL, Landzaaat-Berghuizen MA. Differences between observers in interpreting double-blind placebo-controlled food challenges: a randomized trial. Pediatr Allergy Immunol. 2014;25(8):755–759. doi:10.1111/pai.12313
- Glaumann S, Nopp A, Johansson SGO, Borres MP, Nilsson C, Sampson AP. Oral peanut challenge identifies an allergy but the peanut allergen threshold sensitivity is not reproducible. PLoS One. 2013;8(1):e53465. doi:10.1371/journal.pone.0053465
- Sampson HA, Gerth van Wijk R, Bindsley-Jensen C, et al. Standardizing double-blind, placebo-controlled oral food challenge: American Academy of Allergy, Asthma & Immunology – European Academy of Allergy and Clinical Immunology PRACTALL consensus report. J Allergy Clin Immunol. 2012;130:1260–1274. doi:10.1016/j.jaci.2012.10.017
- Santos A, Alpan O, Hoffmann HJ. Basophil activation test: mechanisms and considerations for it use in clinical trials and clinical practice. Allergy;. 2021;76:2420–2432. doi:10.1111/all.14747
- Schwager C, Kull S, Behrends J, et al. Peanut oleosins associated with severe peanut allergy-importance of lipophilic allergens for comprehensive allergy diagnostics. Allergy Clin Immunol. 2017;140(5):1331–1338. doi:10.1016/j.jaci.2017.02.020
- Jappe U, Schwager C. Relevance of lipophilic allergens in food allergy diagnosis. Curr Allergy Asthma Rep. 2017;17(9):61. doi:10.1007/s11882-017-0731-0
- Vissers YM, Iwan M, Adel-Patient K, et al. Effect of roasting on the allergenicity of major peanut allergens Ara h 1 and Ara h 2/6: the necessity of degranulation assays. Clin Exp Allergy. 2011;41(1):1631–1642. doi:10.1111/j.1365-2222.2011.03830.x
- Sabato V, van Hegel AJ, de Knop KJ, et al. Basophil activation reveals divergent patient-specific responses to thermally processed peanuts. J Investig Allergol Clin Immunol. 2011;21(7):527–531.
- Sancho AI, Rigby NM, Zuidmeer L, et al. The effect of thermal processing on the IgE reactivity of the non-specific lipid transfer protein from apple, Mal d 3. Allergy. 2005;60(10):1262–1268. doi:10.1111/j.1398-9995.2005.00876.x
- Eberlein B, Hann R, Eyerich S, et al. Optimizing of the basophil activation test: comparison of different basophil identification markers. Cytometry B Clin Cytom. 2015;88(3):183–189. doi:10.1002/cytob.21203
- Depince-Berger AE, Sidi-Yahya K, Jeraibt M, Lambert C. Basophil activation test: implementation and standardization between systems and between instruments. J Quant Cell Sci. 2017;91(3):261–269.
- Kim T, Yu J, Li H, et al. Validation of inducible basophil biomarkers: time, temperature and transportation. Clin Cytom. 2021. doi:10.1002/cyto.b.21991
- Lotzch B, Dolle S, Vieths S, Worm M. Exploratory analysis of CD63 and CD203c expression in basophils from hazelnut sensitized and allergic individuals. Clin Transl Allergy. 2016;6:45. doi:10.1186/s13601-016-0134-7
- Zenarruzabeitia O, Vitalle J, Orrantia A, et al. CD300c costimulates IgE-mediated basophil activation and its expression is increased in patients with cow milk’s allergy. J Allergy Clin Immunol. 2019;143(2):700–711. doi:10.1016/j.jaci.2018.05.022
- Sabato V, Verweij MM, Bridts CH, et al. CD300a is expressed on human basophils and seems to inhibit IgE/FcεRI dependent anaphylactic degranulation. Cytometry B Clin Cytom. 2012;82B:132–138. doi:10.1002/cyto.b.21003
- Clark GJ, Ju X, Tate C, Hart DN. The CD300 family of molecules are evolutionary significant regulators of leucocyte functions. Trends Immunol. 2009;30:209–217. doi:10.1016/j.it.2009.02.003
- Patil SU, Calatroni A, Schneider M, et al. Data driven programmatic approach to analysis of basophil activation tests. Cytometry B Clin Cytom. 2018;94(4):667–673. doi:10.1002/cyto.b.21537
- Santos AF, Du Toit G, Douiri A, et al. Distinct parameters of the basophil activation test reflect the severity and threshold of allergic reactions to peanut. J Allergy Clin Immunol. 2015;135(1):179–186. doi:10.1016/j.jaci.2014.09.001
- Mehlich J, Fischer J, Hilger C, et al. The basophil activation test differentiates between patients with alpha-gal syndrome and asymptomatic alpha-gal sensitization. J Allergy Clin Immunol. 2019;143(1):182–189. doi:10.1016/j.jaci.2018.06.049
- Behrends J, Schwager C, Hein M, Scholzen T, Kull S, Jappe U. Innovative robust basophil activation test using a novel gating strategy reliably diagnosing allergy with full automation. Allergy. 2021:1–13. doi:10.1111/all.14900
- Eberlein B. Basophil activation as marker of clinically relevant allergy and therapy outcome. Front Immunol. 2020;11:1815. doi:10.3389/fimmu.2020.01815
- Mukai K, Gaudenzio N, Gupta S, et al. Assessing basophil activation by using flow cytometry and mass cytometry in blood stored 24 hours before analysis. J Allergy Clin Immunol. 2017;139(3):889–899. doi:10.1016/j.jaci.2016.04.060
- Arif-Lusson R, Agabriel C, Carsin A, et al. Streaming basophil activation testing to enable assay miniaturization and automation of sample preparation. J Immunol Methods. 2020;481–482:112793.
- Aljadi Z, Kalm F, Ramachandraiah H, Nopp A, Lundahl J, Russomi A. Microfluidic immunoaffinity basophil activation test for point-of-care allergy diagnosis. J Appl Med. 2019;4(2):152–163. doi:10.1373/jalm.2018.026641
- Aljadi Z, Kalm F, Nilsson C, et al. A novel tool for clinical diagnosis of allergy operating a microfluidic immunoaffinity basophil activation test technique. Clin Immunol. 2019;209:108268. doi:10.1016/j.clim.2019.108268
- Agyemang A, Suprun M, Suarez-Farinas M, et al. A novel approach to the basophil activation test for characterizing peanut allergic patients in the clinical setting. Allergy. 2021;76(7):2257–2259. doi:10.1111/all.14752
- Puan KJ, Andianppan AK, Lee B, et al. Systematic characterization of basophil anergy. Allergy. 2017;72(3):373–384. doi:10.1111/all.12952
- Santos AF, Cuoto-Francisco N, Becares N, Kwok M, Bahnson HT, Lack G. A novel human mast cell activation test for peanut allergy. J Allergy Clin Immunol. 2018;142(2):689–691. doi:10.1016/j.jaci.2018.03.011